Full Length Research Paper

ABSTRACT
The aim of this study was comparing two orthodontic bracket bonding techniques (direct and indirect), with regard to the following variables: plaque index; gingival index, evaluation of gingival crevicular fluid, and white spots on tooth enamel. Seventeen patients were randomly selected (10 men and 7 women) with a mean age of 15.8 years, and these were subjected to comprehensive orthodontic treatment (braces), totaling a sample size of 260 teeth examined. The experimental model used was the split-mouth technique, in each patient, the maxillary brackets in one hemi-arch were bonded by the direct, and in the other by the indirect technique, the same occurring in the mandibular arch. Assessments were performed in the following time intervals: pre-bonding, one, three and six months after initial placement of the brackets. The data were subjected to statistical analysis by the Kruskal-Wallys test (Dunn's post-test) to assess the intra-group evolution of the variables. The Wilcoxon test was used for comparison between groups. The brackets bonded to teeth by the direct technique showed a higher number of surfaces with the presence of bacterial plaque and bleeding, when compared with the indirect technique, in time intervals of 3 and 6 months. For measurement of fluid, direct bonding showed increased index in 3-month evaluation. The occurrence of white spots showed no statistical difference between groups. As conclusion, indirect technique shows less oral health impairment with a lower incidence of plaque accumulation, bleeding and fluid.
Key words: Orthodontics, indirect bonding, periodontics, gingivitis, dental caries.
INTRODUCTION
The bracket bonding technique conventionally used by orthodontists is the direct type, in which the bracket is placed directly on the tooth. However, this technique has some disadvantages, such as performing it in areas of difficult access in the mouth, such as the region of posterior teeth out of the correct position in the arch, the tiredness and stress of both the orthodontist and patient, leading to incorrect bracket bonding in patients, and unsuccessful final positioning of the teeth (Ciuffolo, Tenisci and Pollutri, 2012; Nichols; Gardner and Carballeyra, 2013).
With the aim of overcoming these disadvantages, indirect bonding appeared. In this technique, the brackets are positioned on the patient's plaster casts, using resin composite, and by means of a pre-formed tray, the brackets are transferred to the patient's teeth (Ciuffolo et al., 2012; Silverman et al., 1972). In indirect bonding, the precision of bracket position may be more easily obtained by the multidimensional visualization of the teeth, which in turn contributes the accuracy in the final positioning of the teeth (Bozelli et al., 2013; Castilla et al., 2014; Mizrahi, 1982). When correctly performed, the indirect technique leads to reduction in stress of the patient and professional at the time of placing the appliance, by diminishing the chair-time (Bozelli et al., 2013; Castilla et al., 2014; Ciuffolo, Tenisci and Pollutri, 2012; Deahl et al., 2007; Gange, 2000).
However, as yet there are few orthodontists who routinely use indirect bonding, because there are persistent doubts about the consistency and predictability of the brackets bonding to the teeth, cost of material (Gayake et al., 2013), and precision in positioning the brackets (Castilla et al., 2014; Koo, Chung and Vanarsdall, 1999). Another factor pointed out as being controversial is the excessive amount of adhesive material left around the brackets with the use of the indirect bonding technique (Gayake et al., 2013; Kanashiro et al., 2014).
In general, fixed appliance prevent the maintenance of good oral hygiene, particularly when brackets are bonded with excessive adhesive material, thus favoring bacterial plaque accumulation (Al-Anezi and Harradine, 2012; Jordan and LeBlanc, 2002; Nassar et al., 2009), which in turn could lead to the occurrence of gingival inflammation (Al-Anezi and Harradine, 2012; Miles, 2010) and enamel demineralization - white spots (O'Reilly et al., 2013; Tufekci et al., 2011). If on the one hand, indirect bonding allows the removal of excess resin during the act of laboratory bonding; on the other hand, it does not allow the predictability of adhesive flow during its clinical stage (Ciuffolo et al., 2012; Kanashiro et al., 2014; Miles, 2010; Mohode, 2012).
By virtue of the orthodontic bracket tending to be an accessory that retains plaque (Al-Anezi and Harradine, 2012; Jordan and LeBlanc, 2002; Nassar et al., 2009), and knowing that indirect technique is a procedure increasingly being used by orthodontists (Ciuffolo et al., 2012; Gange, 2000; Silverman et al., 1972). The aim of this research was to compare the plaque index, gingival index, evaluate the gingival crevicular fluid and index of white spots on tooth enamel in patients submitted to bracket bonding by means of the direct and indirect techniques.
MATERIALS AND METHODS
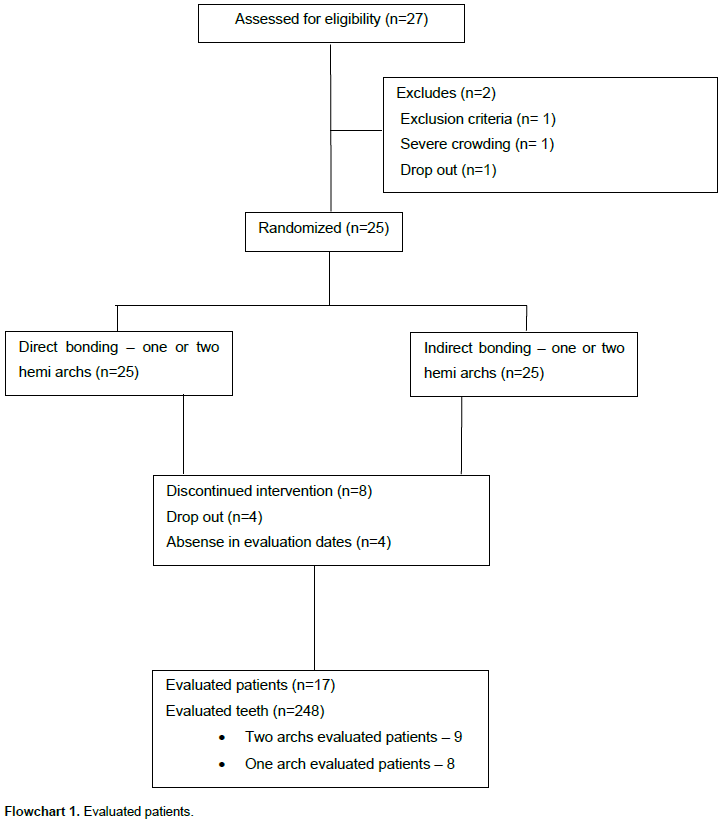
This was a prospective, randomized study, conducted between August 2013 and October 2014. Before conducting it, the study was approved by the Ethics Committee on Research in Human Beings of the State University of West Paraná, under report No.16610513.5.0000.0107. The criteria for inclusion in the research were: the need for treatment with a fixed appliance, and symmetrical malocclusion when evaluated in the sagittal direction. The exclusion criteria were: very severe crowding, abnormality in the morphology of dental crowns, caries, and extensive restorations. For the research, 17 patients were randomly selected (10 men and 7 women, with a mean age of 15.8 years) from among those who requested standard orthodontic documentation for the confirmation of clinical diagnosis and preparation of planning, totaling a sample number of 248 teeth for the research, according to Flowchart 1.
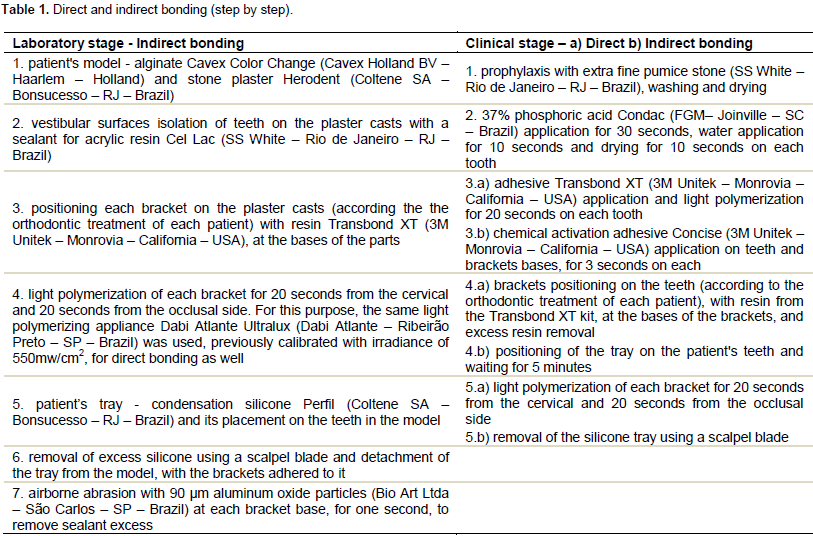
Assembly of the orthodontic appliance of these patients occurred in accordance with the split-mouth model, in which metal orthodontic brackets, of the Roth prescription (Morelli – Sorocaba – SP – Brazil), were bonded to the maxillary right and mandibular left hemiarches by means of the direct technique; and bonded to the maxillary left and mandibular right hemiarches, by the indirect technique (Nassar et al., 2013). This protocol explains the manner in which this research was considered randomized, since each patient had brackets bonded by means of the two techniques. All the patients were instructed regarding the mechanic control (modified Bass technique plus dental floss). The same operator performed the laboratory stage of indirect bonding, and the clinical stages of direct and indirect bonding, according to Table 1. All the evaluations were performed by the same, previously calibrated operator, as follows:
Plaque index and gingival index
A clinical exam of each patient was performed before bonding, and in the return visits at one, three and six months, in order to observe: a) Plaque index of Silness and Loe, by the presence or absence of bacterial plaque on the vestibular, palatine, mesial and distal surfaces of the incisors, canines and premolars, with designation of codes 0 for absence or 1 for presence of visible plaque (Silness and Loe, 1964) and b) Gingival index of Loe and Silness, in which the gingival inflammatory condition was evaluated by the presence or absence of bleeding in vestibular and palatine sulcus (Loe and Silness, 1963), by means of probing with a millimeter probe (Williams #23). After this, the percentages of surfaces with the presence of bacterial plaque and bleeding were calculated. Using these data, the relationship of difference in resin remainders on the direct and indirect bonding with the presence of plaque and gingival index was evaluated.
Gingival crevicular fluid
Before bonding, and at one, three and six months after the insertion of the appliance, gingival crevicular fluid was collected from the vestibular sulcus of the central incisors, canines and second premolars of each of the patients in the study for the evaluation of gingivitis. This collection was made by introducing a small absorbent paper cone into each sulcus, and evaluating it for thirty seconds (Hinrichs et al., 1984).
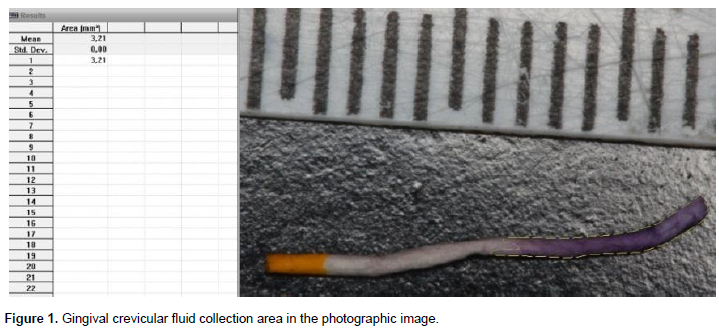
After the removal of each cone, they were inserted in a solution with 99ml of absolute alcohol (ethanol) and 1 g of nynhydrin (2,2-dihydroxy-hydrydin-1,3-dione) marker for 2 min. This substance is generally used for the detection of primary amines, particularly of amino acids, because when they react with these free amines, a dark blue or purple color, known as Ruhemann purple, is produced (Hinrichs et al., 1984). After being marked and dried, the cones were photographed by the same researcher, in accordance with the following standards: resolution – all the images were obtained with a Canon EOS T3i (Canon Inc. – Taiwan) camera, with a circular flash in automatic mode, opening at 32, opening speed at 1/60 and ISO 100; focus – all the photographs were taken with focus 1-1.02-0.31 mm, against a black background; distance – seeing that all the cones were photographed with the same focus, the distance required between the camera and cone it order to obtain clarity, was always the same. The gingival crevicular fluid collection area in the photographic image was measured by means of the program ImageTool (San Antonio, Texas, USA). To calibrate the program, it was necessary to place a ruler on the cones in the photos to make marks in millimeters, and after this the area marked on each cone was measured with the software in mm2 (Figure 1).
White spot index
In the same clinical exams mentioned above, the presence of white spots on the enamel of the vestibular and palatine surfaces of those teeth was verified. The sites examined were classified as presence or absence of white spots; the percentage value of surfaces with the presence of white spots was calculated in order to compare the two techniques (O'Reilly et al., 2013; Tufekci et al., 2011).
Statistical analysis
After six months of obtaining information from the sample units of indirect bonding and those of direct bonding, the data were evaluated by the statistical method, using the program Biostat 5.0 (Instituto Mamirauá – Belém – Pará - Brazil). The data obtained were submitted to statistical analysis: the Kruskal-Wallis (Dunn post-test) to evaluate the intra-group evolution of the variables. The Wilcoxon test was used for inter-group comparisons. To evaluate the reliability of the measurements obtained with reference to inflammatory fluid, after one month, new measurement of the images were made, in order to measure the method error (systematic - paired t-test and casual - Dahlberg formula).
RESULTS
The mean method error, either systematic or casual, showed there was no statistically significant difference between the measurements obtained for the area of the cones in the quantitative evaluation of crevicular fluid (p>0.05).
Table 2 shows the percentages of the plaque index for direct and indirect bonding. In the direct bonding group, there was a significant increase in plaque index, showing a remarkable difference between the time intervals before bonding and the periods of 3 and 6 months (p<0.01). Whereas, in the indirect bonding group, there was no statistically significant variation in the plaque index (p>0.05). For the inter-group comparisons a larger number of faces with presence of bacterial plaque was detected for the direct bonding groups in the periods of 3 months (p<0.05) and 6 months (p<0.01).
Table 3 shows the percentages of the gingival index for direct and indirect bonding. In the direct bonding group, there was a significant increase, showing a remarkable difference between the time intervals before bonding and the periods of 3 and 6 months (p<0.01). Whereas, in the indirect bonding group, there was no statistically significant variation in the gingival index (p>0.05). For the inter-group comparisons a larger number of surfaces with presence of bleeding were detected for the direct bonding groups in the periods of 3 months (p<0.05) and 6 months (p<0.01).


Table 4 shows the data for the areas of the cones (inflammation - gingival crevicular fluid) for the direct and indirect bonding groups. In the direct bonding group there was a significant increase in inflammation between the first and second evaluations, and this remained stable until the last exam (p<0.01). Whereas, in the indirect bonding group, there was no statistically significant variation in inflammation (p>0.05). For the inter-group comparisons a higher level of inflammation was detected for the direct bonding groups in the period of 3 months (p<0.01).

Table 5 shows the percentages of the occurrence of white spots for direct and indirect bonding. In the groups evaluated there was no significant increase in white spots over time (p>0.05). For the inter-group comparison no significant differences were detected between the techniques for white spots in the periods evaluated (p>0.05).

DISCUSSION
Although the indirect bonding technique was recom-mended in the 1970s (Silverman et al., 1972), the topic has sometimes been discussed again in the world literature (Bozelli et al., 2013; Castilla et al., 2014; Ciuffolo et al., 2012; Deahl et al., 2007; Gange, 2000; Gayake et al., 2013; Hodge et al., 2014; Kanashiro et al., 2014; Koo et al., 1999; Miles, 2010; Mohode, 2012; Nichols et al., 2013). At present, it is routinely used in the lingual technique, and eventually in the technique for brackets bonded from the vestibular side, when the professional has the intention to hasten the clinical act of positioning the brackets, thereby reducing chair-time, with this factor being an aspect on which there is unanimity in the studies (Bozelli et al., 2013; Castilla et al., 2014; Ciuffolo et al., 2012).
However, a relevant variable to be considered during orthodontic treatment is the maintenance of periodontal health, since the orthodontic bracket tends to be an accessory that retains bacterial plaque (Al-Anezi and Harradine, 2012; Jordan and LeBlanc, 2002; Nassar et al., 2009). The doubt that motivated this study was precisely whether the type of adhesive - with chemical polymerization - used in the indirect technique, would have more chance of causing deleterious effects on the periodontium. This is because, in this type of technique there is no predictability about the flow of the adhesive in its clinical stage (Ciuffolo et al., 2012; Kanashiro et al., 2014; Miles, 2010; Mohode, 2012), due to the lack of access caused by the transfer tray.
On the other hand, the control of excess resin appears to be better in the indirect technique, since the excess is removed around the brackets on the teeth in the plaster cast - laboratory stage (Ciuffolo et al., 2012), differently from the direct technique, in which the excess is removed from the tooth itself. This is difficult in areas to which access is difficult, and may lead to altering the position of the bracket (Hodge et al., 2004). The scarcity of articles in literature about the periodontal condition with the use of the indirect technique, and about the relationship with the adhesives used in this technique, has resulted in the choice of four aspects evaluated: the plaque index, gingival index, gingival crevicular fluid and the white spot index.
In this study, it was observed that the evolution of the data with regard to bacterial plaque and bleeding occurred in the same manner (Tables 2 and 3), with a significant increase in direct bonding, showing a remarkable difference between the time interval before bonding and the periods of 3 and 6 months. In the indirect bonding group, there was no statistically significant variation in the two above-mentioned indices. For the inter-group comparisons a larger number of surfaces with presence of bacterial plaque were detected for the direct bonding groups in the periods of 3 and 6 months. The results of increase in difficulty with per-forming oral hygiene, and consequent high plaque and bleeding indices were expected (Klöehn and Pfeifer, 1974; Steinberg and Eyal, 2004; Zachrisson and Zachrisson, 1972) but the surprising result was the better response of the indirect technique, with regard to these parameters, given that this has not been tested comparatively in the literature.
Although researches commonly use the plaque index and gingival index (Loe and Silness, 1963; Silness and Loe, 1964) for periodontal evaluation in orthodontics, another aspect evaluated in this study was the gingival crevicular fluid. The methodology chosen for this purpose was by marking absorbent paper cones used to collect this fluid as a chemical marker (Hinrichs et al., 1984), which was shown to be efficient, since the results of this requisite also pointed towards the superiority of maintaining good periodontal conditions by means of the indirect bonding technique (Table 4).
Another factor that pointed out the better results of the indirect technique, by means of validation of the evaluations performed, was the split-mouth design of the study, because the periodontal parameters in the initial evaluation were shown to be equal from a statistical point of view. Moreover, starting with the same oral hygiene condition in order to make comparisons about bonding techniques, there was no influence of confounding factors, such as the systemic status of the patient, dexterity for performing brushing and use of dental floss.
By virtue of the similarity of the results of plaque index, gingival index and gingival crevicular fluid, associated with the good relationship of the indirect technique with plaque control found in the literature (Dalesandri et al., 2012) it would seem just to affirm that the removal of excess resin composite would have more relevance in the maintenance of periodontal health, than the control of eventual excess of adhesive.
This periodontal superiority of the indirect technique did not reflect on the white spot index, which showed no statistical differences between the direct and indirect techniques (Table 5). This raises the hypothesis of its appearance not being related to types of adhesive or the manner in which the accessories were bonded, but rather the fixed orthodontic treatment itself, as has been related in the literature (Mizrahi, 1982; Srivastava et al., 2013; Tufekci et al., 2014). Mizrahi (1982) and Tufekci et al. (2014) determined the prevalence of white spots before and after orthodontic treatment, with the former relating a significant increase of 12.3% in prevalence and 60% for the opacity index (Mizrahi, 1982), and the latter author observed an incidence of 38% for the period of six months, 46% for twelve months, while there was 11% for the control group (Tufekci et al., 2014). Due to the indirect technique better results, its clinical application is valid to minimize the undesirable periodontal effects, since that clinical results are also good.
CONCLUSIONS
The indirect technique showed a lower level of com-promise of oral health, since both the plaque indices, gingival indices and quantity of gingival crevicular fluid did not alter significantly with the passage of time in this technique, differently from the direct technique. There was no difference between the bonding techniques with regard to the appearance of white spots.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Al-Anezi AS, Harradine NW (2012). Quantifying plaque during orthodontic treatment. Angle Orthod. 82(4):748-753. |
|
|
Bozelli JV, Bigliazzi R, Barbosa HA, Ortolani CL, Bertoz FA, Faltin Junior K (2013). Comparative study on direct and indirect bracket bonding techniques regarding time length and bracket detachment. Dental Press J. Orthod. 18(6):51-57. |
|
|
Castilla AE, Crowe JJ, Moses JR, Wang M, Ferracane JL, Covell DA (2014). Measurement and comparison of bracket transfer accuracy of five indirect bonding techniques. Angle Orthod. 84(4):607-614. |
|
|
Ciuffolo F, Tenisci N, Pollutri L (2012). Modified bonding technique for a standardized and effective indirect bonding procedure. Am. J. Orthod. Dentofacial Orthop. 141(4):504-509. |
|
|
Dalesandri D, Dalesandri M, Bonetti S, Visconti L, Paganelli C (2012). Effectiveness of na indirect bonding technique in reducing plaque accumulation around braces. Angle Orthod. 82(2):313-318. |
|
|
Deahl ST, Salome N, Hatch JP, Rugh JD (2007). Practice-based comparison of direct and indirect bonding. Am J Orthod Dentofacial Orthop 132(6):738-742. |
|
|
Gange P (2000). More on indirect bonding. Am. J. Orthod. Dentofacial Orthop. 117(1):18A. |
|
|
Gayake PV, Chitko SS, Sutrave N, Gaikwad PM (2013). The direct way of indirect bonding--the combined effect. Int J Orthod Milwaukee 24(3):15-17. |
|
|
Hinrichs JE, Bandt CL, Smith JÁ, Golub LM (1984). A comparison of 3 systems for quantifying gingival crevicular fluid with respect to linearity and the effects of qualitative differences in fluids. J. Clin. Periodontol. 11(10):652-661. |
|
|
Hodge TM, Dhopatkar AA, Rock WP, Spary DJ (2004). A randomized clinical trial comparing the accuracy of direct versus indirect bracket placement. J. Orthod. 31(2):132-137. |
|
|
Jordan C, LeBlanc DJ (2002). Influences of orthodontic appliances on oral populations of mutans streptococci. Oral Microbiol. Immunol. 17(2):65-71. |
|
|
Kanashiro LK, Robles-Ruíz JJ, Ciamponi AL, Medeiros IS, Dominguez GC, de Fantini SM (2014). Effect of adhesion boosters on indirect bracket bonding. Angle Orthod. 84(1):171-176. |
|
|
Klöehn JS, Pfeifer JS (1974). The effect of orthodontic treatment on the periodontium. Angle Orthod. 44:127-134. |
|
|
Koo BC, Chung CH, Vanarsdall RL (1999). Comparison of the accuracy of bracket placement between direct and indirect bonding techniques. Am. J. Orthod. Dentofacial Orthop. 116(3):346-351. |
|
|
Loe H, Silness J (1963). Periodontal disease in pregnancy - Prevalence and severity. Acta Odontol. Scand. 21:533-551. |
|
|
Miles P (2010). Indirect bonding--do custom bases need a plastic conditioner? A randomised clinical trial. Aust. Orthod. J. 26(2):109-112. |
|
|
Mizrahi E (1982). Enamel demineralization following orthodontic treatment. Am. J. Orthod. 82:62-67. |
|
|
Mohode R (2012). Minimizing adhesive flash during indirect bonding of a lingual retainer. J. Clin. Orthod. 46(4):233-234. |
|
|
Nassar PO, Bombardelli CG, Walker CS, Neves KV, Tonet K, Nishi RN, Bombonatti R, Nassar CA (2013). Periodontal evaluation of different toothbrushing techniques in patients with fixed orthodontic appliances. Dental Press J. Orthod. 18(1):76-80. |
|
|
Nichols DA, Gardner G, Carballeyra AD (2013). Reproducibility of bracket positioning in the indirect bonding technique. Am. J. Orthod. Dentofacial Orthop. 144(5):770-776. |
|
|
O'Reilly MT, De Jesús Vi-as J, Hatch JP (2013). Effectiveness of a sealant compared with no sealant in preventing enamel demineralization in patients with fixed orthodontic appliances: a prospective clinical trial. Am. J. Orthod. Dentofacial Orthop. 143(6):837-844. |
|
|
Silness J, Loe H (1964). Periodontal disease in pregnancy - Correlation between oral hygiene and periodontal condtion. Acta Odontol. Scand. 22:121-135. |
|
|
Silverman E, Cohen M, Gianelly AA, Dietz VS (1972). A universal direct bonding system for both metal and plastic brackets. Am. J. Orthod. 62(3):236-244. |
|
|
Srivastava K, Tikku T, Khanna R, Sachan K (2013). Risk factors and management of white spot lesions in orthodontics. J. Orthod. Sci. 2(2):43-49. |
|
|
Steinberg D, Eyal S (2004). Initial biofilm formation of Streptococcus sobrinus on various orthodontics appliances. J. Oral Rehabil 31(11):1041-1045. |
|
|
Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ (2011). Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 81(2):206-210. |
|
|
Tufekci E, Pennella DR, Mitchell JC, Best AM, Lindauer SJ (2014). Efficacy of a fluoride-releasing orthodontic primer in reducing demineralization around brackets: an in-vivo study. Am. J. Orthod. Dentofacial Orthop. 146(2):207-214. |
|
|
Zachrisson S, Zachrisson BU (1972). Gingival condition associated with orthodontic treatment. Angle Orthod. 42:26-34. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


