ABSTRACT
There is increasing interest in investigating the association between dental caries and childhood obesity, particularly among preschoolers where the evidence is limited. We aimed to measure the prevalence of obesity/overweight among preschool children aged 3 to 6 years, and to determine the relationship between obesity and dental caries in the primary dentition. A cross-sectional study was carried out in eight public and private preschools using a multi-stage stratified sample of 820 children. Waist circumference (WC) and body mass index (BMI) measurements were obtained. Caries was assessed using the National Institute of Dental Research’s decayed, missed or filled score (dmft). Based on BMI, 15% of children were obese and 10% were overweight. Based on WC, 13% of children were obese. The prevalence of obesity/overweight based on BMI was significantly higher among girls (p-value=0.014) and private preschools (p-value<0.001). Based on BMI, obese and overweight children had lower dmft scores than underweight and normal children (p-value<0.001). Based on WC, obese children had lower dmft scores than non-obese children (p-value<0.001). Obesity prevalence was high, particularly among girls and private preschool children. Caries activity was lower in overweight and obese children. Longitudinal studies are essential to investigate the association between caries and obesity in preschool children.
Key words: Children, obesity, overweight, dental caries, body mass index (BMI).
Childhood obesity has been highlighted as a serious and challenging public health problem (Mirmiran et al., 2010). Obesity in childhood is associated with precursors of adult illnesses and long term health consequences where overweight children are threatened of becoming overweight or obese adults besides the hazard of having chronic health conditions in the future (Nadeau et al., 2011). In addition, childhood obesity affects self-confidence and can negatively influence social interaction and cognitive development (Hanley et al., 2000).
Age-and gender specific body mass index (BMI) percentiles are commonly used to measure obesity in children. Overweight children as described by the Centers for Disease Control and Prevention are those having a BMI percentile at or above the 85th and below the 95th percentile, while obese children are those at or above the 95th percentile (CDC, 2010). Despite the fact that BMI is considered to be a reliable indirect measure of body fat, it has limitations. BMI does not specify body fat vs. muscle; hence, persons with elevated muscle mass may have an increased BMI without being overweight (Janssen et al., 2004). Recent research recommends using waist circumference (WC) as a better disease risk predictor than BMI (Janssen et al., 2002).
Although the relationship between childhood and adulthood obesity is alarming, the prevalence of obesity remains underestimated among preschoolers, and the general effects of obesity in this age group remain under recognized. A study conducted in Saudi Arabia, among 12,701 children from 1 to 18 years reported, a prevalence of overweight of 4.6 and 4.7% and of obesity of 10.0 and 9.8% among preschool boys and girls, respectively (El-Hazmi and Warsy, 2002). Another recent study in the United States conducted among 4,111 adolescents and children from birth through 19 years of age reported that 12% of preschool children aged 2 to 5 years were obese (Ogden et al., 2012).
Both environmental and genetic factors are risk moderators that influence obesity (Hetherington and Cecil, 2010). Similar to obesity, dental caries is a prevalent, multifactorial problem that affects children’s general health. Evidence supports a relationship between dental caries and negative eating habits (Dye et al., 2004), and current dietary intake which has been associated with obesity progression at young age (Gidding et al., 2006). Both, obesity and dental caries, are thought to share common risk factors: Lifestyle, nutrition, social, physical, and biological as well as cultural environmental factors (Spiegel and Palmer, 2012); thus a relationship between dental caries and weight seems logical.
There is a global interest in investigating the relationship between obesity and dental caries among children due to conflicting results in the literature (Alkarimi et al., 2014). Some studies reported a direct positive association between obesity and dental caries (Reifsnider et al., 2004; Willershausen et al., 2004), some reported a negative association (Granville-Gracia et al., 2008; Oliveira et al., 2008) and some concluded that there is no relationship between them (Bagherian and Sadeghi, 2013; Shahraki et al., 2013). Furthermore, several systematic reviews were conducted to investigate the relationship between obesity and dental caries. A systematic review by Hooley et al. (2012) included studies involving normal and overweight children and reported a positive association between dental caries and both high and low BMI. Another recent systematic review conducted by Li et al. (2015) concluded that there is conflicting evidence in regards to the association between children’s anthropometric measurements and dental caries over time.
Studies conducted in different regions in Saudi Arabia have reported a high obesity and overweight prevalence in children of different ages (Al-Rukban, 2003; El-Hazmi and Warsy, 2002; Collison et al., 2010), but very few studies have investigated its prevalence among preschoolers (Al-Dossary et al., 2010; El-Hazmi and Warsy, 2002). Furthermore, there is limited research investigating the association between obesity and caries among preschool children. Thus, the objectives of the current study were to investigate the prevalence of obesity in preschool children aged 3 to 6 years using BMI and WC, and to assess the association between obesity and caries in the primary dentition.
Study outline and sampling
This study was a cross-sectional study conducted in Jeddah, Saudi Arabia. Data collection took place between September 2014 and June 2015. The prevalence of overweight/obesity among the specified age group was 26% according to a previously conducted survey (Al-Dossary et al., 2010). The free web-based operating system Open Epi version 2 was used to calculate the sample size where the prevalence of obesity was set at 26% with confidence limits of 3%. The significance level was set at 0.05 and the power at 0.85. The total estimated sample size was 779 preschool children.
The sampling method used in the study was multistage stratified random sampling from the preschool children officially registered at the Ministry of Education in Jeddah city. Because the study focused on caries in the primary teeth, children enrolled in kindergarten-2 (KG-2) and kindergarten-3 (KG-3) were selected. Inclusion criteria were children aged 3 to 6 years who had primary dentition only and those who returned a consent form signed by their parent(s). According to the Saudi Ministry of Education in Jeddah, 14,808 children were enrolled in these kindergartens. First, preschools were randomly selected from an updated list of schools, which was stratified by district (North, East, South or West) and funding source (public or private). One preschool was selected from each stratum to give a total of 8 preschools. Second, from each preschool, two classes were randomly selected, one KG-2 and the other KG-3 to satisfy the required sample size.
The study was approved by the ethical committee of the Faculty of Dentistry at King Abdulaziz University (KAUFD) (# 028-16). Prior to visiting the selected preschool, approval was taken from the Ministry of Education in Jeddah and preschool principles. Consent forms having detailed information about the conducted study were given to the students on the first visit. On the second visit, examination was done only for children who brought back the signed parental consent form. The teachers, administrative preschool staff, and the students enrolled were given a brief orientation before starting the measurement and examination procedures.
Data collection
Anthropometric measurements
Height, weight, and WC were measured by three coauthors who received training prior to data collection. The anthropometric measurements were taken by three coauthors after calibration. To assess intra-examiner reliability, 10 patients attending KAUFD clinics were examined over two points in time, one week apart (kappa score 0.85). To assess inter-examiner reliability 20 patients attending KAUFD clinics were examined (kappa score 0.77). In case of any disagreement, a consensus was reached by retaking the measurement. Measurements for WC, height, and weight were taken twice for each child and the average was used. Height and WC were measured with measuring tape (non-elastic). Height was measured as the distance between the highest point of the head and the floor, while WC was measured at the level of the superior iliac crest. Weight was measured using an electronic weight scale. Children were barefooted wearing minimal clothing, without any jackets or accessories (Li et al., 2006).
Dental charting
Dental charting was performed by two coauthors, different from those who took the height, weight and WC measurements. A detailed rubric for dmft scoring (Broadbent and Thomson, 2005) was followed for calibration prior to study initiation. Thirty patients participated in a pilot study to calculate inter-examiner reliability (Kappa score was 0.90). To assess the intra-examiner reliability, 10 pediatric patients attending KAUFD clinics were examined over two points in time with a one-week interval (kappa score was 0.85). In case of any disagreement, measurements were retaken to come to an agreement. Dental examination was performed under torch light and basic infection control measures were employed. A round-ended dental probe, a sterile flat surface mirror in addition to gauze and cotton rolls was used for examination. If teeth had temporary restorations they were scored as d. If teeth had fissure sealants or white spot lesions they were marked as sound. Upon examination, a confidential referral letter to KAUFD discussing the child’s oral condition and treatment needs was sent to his/her parent.
Data analysis
In this study the 2 measurements (BMI and WC) were used to classify children as overweight and obese. BMI was calculated according to the formula BMI = weight (in kg)/height2 (in m). Children were grouped into four categories using age and gender specific criteria: Underweight (BMI less than 5th percentile), normal weight (BMI between 5th and 84th percentile), overweight (BMI between 85th and 94th percentile), and obese (BMI more than 95th percentile). The BMI percentiles reported by Al Herbish et al. (2009) for the Saudi population and the cut-off points reported by Barlow (2007) were used. Regarding WC, the percentiles reported by Bassali et al. (2010) were used and obese children were defined as those with WC higher than the 90th percentile for age and sex. The dmft classification was used to measure dental caries in the primary teeth (Broadbent and Thomson, 2005)
To describe continuous baseline and demographic charac-teristics, medians and interquartile ranges (IQR) were reported. To describe categorical baseline, demographic characteristics, obesity status and dental caries, frequencies and percentages were reported. Chi-square test was used to test associations between obesity status and sex and type of preschool. The associations between dmft and sex, type of preschool and obesity status based on WC were tested using Wilcoxon (Mann-Whitney) test. The association between dmft and obesity status based on BMI was tested using Kruskal-Wallis test, followed by Dunn test if the results were significant. In addition, the relationship between BMI and WC (as continuous variables) and dmft was tested using Spearman’s correlation. The significance level was set at P<0.05. Stata Version 13.0 was used for all data management and statistical analyses (Stata Corp, College Station, Texas, USA).
Consent forms were distributed to 1,000 children. The total number of children included in the study was 820, giving a response rate of 82%. Table 1 displays their characteristics. Females represented 49% of the sample. The sample age ranged from 3 to 6 years old, with a mean age of 5.5 ± 0.8 years. Children were enrolled in private (73%) and public (27%) preschools. The median BMI was 15 (IQR 14 to 16) kg/m2 and the median WC was 52 (IQR 49 to 56) cm. Based on the BMI, 7% of preschoolers were underweight and 68% were normal while 15% were obese and 10% were overweight. Based on the WC, 13% of preschoolers were considered obese.

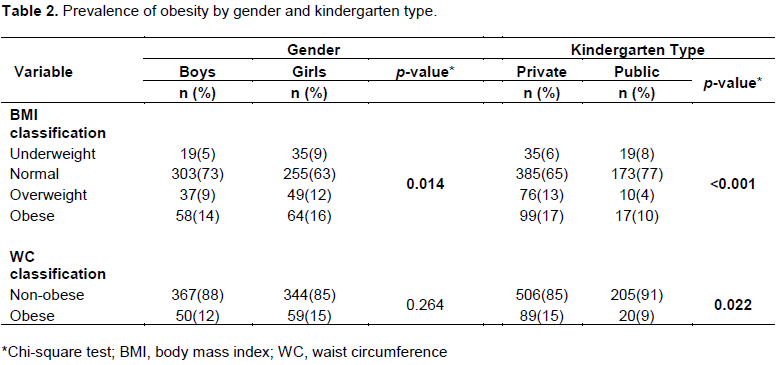
The prevalence of obesity by sex and preschool type is presented in Table 2. Girls had higher prevalence of overweight/obesity as well as underweight than boys based on BMI (p-value<0.001), however the differences were non-significant based on WC. In private preschools, the prevalence of overweight/obesity based on BMI (30%) was significantly higher than public preschools (14%, p-value<0.001). Private preschools also had a significantly higher proportion of children (15%) classified as obese based on WC compared with public preschools (9%, p-value=0.022).

Table 3 shows the association between gender, preschool type, obesity status, and caries. Children from public preschools had higher median dmft scores (7, IQR 2 to 11) than children from private preschools (1, IQR 0 to 5, p-value<0.001). No significant differences in dmft scores were found between girls and boys (p-value<0.285). There was a significant association between obesity status based on either BMI or WC and dmft scores (p-value<0.001). Based on BMI, the highest median dmft scores were among normal weight children (3, IQR 0 to 8) followed by underweight children (2.5, IQR 0 to 8) and then overweight (2, IQR 0 to 5) and obese children (0, IQR 0 to 4). The multiple comparisons showed that dmft scores were significantly lower among obese and overweight children compared to normal and underweight children. Based on WC, obese children had lower median dmft scores (0, IQR 0 to 4) than non-obese children (3, IQR 0 to 7, p-value<0.001). A significant weak negative correlation existed between BMI and dmft (Spearman’s rho= -0.16, p-value<0.001), while a non-significant weak negative correlation existed between WC and dmft (Spearman’s rho = -0.07, p-value=0.066).

Dental caries in children are reported to be associated with anthropometric outcomes, but the evidence is conflicting. To date, no study has been conducted in Saudi Arabia to evaluate the relationship between overweight/obesity prevalence and dental caries among preschool children. Thus this cross-sectional study investigated the prevalence of obesity in preschool children aged 3 to 6 years old using BMI and WC and assessed the association between obesity and caries in the primary dentition.
The current study showed that the total prevalence of overweight and obesity among preschool children was 10 and 15%, respectively. The results are generally consistent with findings of other studies in Saudi Arabia. One study reported obesity and overweight rates of 18.1 and 19.2%, respectively, among preschool children aged 2 to 4 years in the Eastern Province (Al-Dossary et al., 2010). Another survey conducted in different regions of Saudi Arabia found that the total prevalence of overweight in boys and girls aged 1 to 6 years was 4.6 and 10%, respectively and of obesity was 4.7 and 9.8%, respectively. The highest prevalence of obesity was observed among the 2 to 3 year olds (El-Hazmi and Warsy, 2002). A lower prevalence of obesity was found in Tehran where the prevalence of obesity and overweight among children aged 3 to 5 years was 5.0 and 2.2%, respectively (Esmaillzadeh et al., 2006). The differences between the obesity prevalence in the current study and others might be attributed to the different cultural and dietary habits between the regions as well as the different methods used for assessing overweight/obesity.
The high prevalence of obesity reported among our study population can be attributed to changing nutritional and lifestyle habits (Amin et al., 2008). For instance, there has been an increase in the consumption of high sugar beverages and fruit juices (Al-Dossary et al., 2010)and replacement of traditional food with fast food as a result of maternal employment (Baker et al., 2005). Furthermore, physical activity is limited and more time is being spent engaging in seated activities (El-Hazmi and Warsy, 2002)such as watching television and playing computer and video games.
Girls had higher prevalence of overweight/obesity and underweight than boys based on BMI, but the differences were non-significant based on WC. The difference in results might be due to the different measurement tools and cut off criteria used. A study conducted among school-aged children found a significantly higher prevalence of obesity among boys and a significantly higher prevalence of overweight among girls (El Mouzan et al., 2010). In addition, a study reported that males showed a higher prevalence of obesity in all age groups studied (Al-Dossary et al., 2010), whereas another study reported higher prevalence of overweight/obesity among girls (Jagadesan et al., 2014). However, these studies investigated older age groups than the preschoolers in our study; hence, the differences are difficult to interpret.
The relationship between overweight/obesity prevalence and type of preschool was examined and the results showed a significant difference between private and public preschools. Our findings agree with (Patnaik et al., 2011)who reported significantly higher prevalence of overweight/obesity among private school children aged 5 to 10 years in India. The results also agree with Jagadesan et al. (2014)and Patnaik et al. (2015)who both reported high overweight/obesity prevalence among children in private schools. Several studies have outlined potential reasons for these differences. The type of lunch/snacks provided in private preschools (mainly refined carbohydrates with no vegetables or fruits) might play a role (Mwaikambo et al., 2015). Furthermore, children in public preschools are assumed to come from families with lower socioeconomic status, who might bring lunch from home or might be given a small amount of money to buy food from preschool premises. On the other hand, children in private preschools are more likely to be provided with enough money to buy more than one snack per day. Other studies (Duncan et al., 2011; Pabayo et al., 2010)relate significant differences in obesity between public and private preschoolers to other factors as means of transportation to and from school. However, this cannot explain the differences reported in the current study as preschoolers aged 3 to 5 years are usually dropped off at school in a car or a bus, and do not arrive on foot due to their young age.
The findings of the present study showed that children from public preschools had significantly higher dmft scores than children from private ones. These results are in agreement with a Brazilian study, which found caries to be more prevalent in public school children and suggested that socioeconomic status may be associated with the prevalence of caries (Granville-Garcia et al., 2008). In addition, Kaiser et al. (2002) reported that low socioeconomic status of children, measured by their limited education and income, was linked to higher caries and food insecurity. They also reported that children occupying low socioeconomic domestics were unable to meet the food pyramid guidelines in comparison to other children.
Our study revealed that lower dmft scores were found among overweight and obese children in comparison to underweight and normal weight children. One possible explanation is that obese/overweight children might consume more fatty foods than underweight/healthy children, but might not consume more foods high in sugar. Our results conflict with Hong et al. (2008)who reported a non-significant relationship between caries and childhood obesity except among children ages 60-72 months. They explained that both are age associated conditions and accordingly bigger children are more prone to have a stronger association. On the other hand, our results agrees with findings of Sheller et al. (2009) who found a significant number of underweight children with severe early childhood caries. They believed that pain and discomfort from caries might have prevented these children from consuming adequate nutrition and thus resulted in underweight. In addition, Werner et al. (2012) reported an association between obesity and caries in the primary teeth but did not explain why obese/overweight children had fewer caries. Studies have found dental caries and obesity coexisting among children with low family income (Marshall et al., 2007) and that those having high dental caries experience and high BMI are found to share similar behavioral practices (Cinar and Murtomaa, 2011). These findings might be an explanation for the association between dental caries and obesity.
This study has some limitations. It is a cross-sectional survey, providing data at one point in time, so temporality is ambiguous and causal relationships cannot be established. In addition, the findings might not be representative of the whole country, as it was conducted in only one city. Lastly, the current study did not collect data on common risk factors of obesity and dental caries, which might distort the relationship between them.
In conclusion, obesity prevalence was high, particularly in girls and private preschool children. Caries prevalence was lower in overweight and obese than normal and underweight preschoolers. It is important for authorities developing obesity prevention programs to implement nutritional health education that provides children with the skills required to make healthy food choices. There is an urgent need to increase physical education hours, with greater focus on educating children and parents about the hazards of overweight/obesity. Pediatric dentists play a challenging role in reducing obesity, by going beyond health education, and providing dietary counseling and motivating behavior for better dietary choices to enhance an active behavior change. Further longitudinal studies are needed to investigate the association between caries and obesity in preschool children.
The authors have not declared any conflict of interests.
REFERENCES
|
Al Herbish AS, El Mouzan, MI, Al Salloum AA, Al Qureshi MM, Al Omar AA, Foster PJ, Kecojevic T (2009). Body mass index in Saudi Arabian children and adolescents: a national reference and comparison with international standards. Ann. Saudi Med. 29:342.
Crossref
|
|
|
|
Al-Dossary SS, Sarkis PE, Hassan A, Ezz El Regal M, Fouda AE (2010). Obesity in Saudi children: a dangerous reality. East Mediterr. Health. 16:1003-1008.
|
|
|
|
Alkarimi HA, Watt RG, Pikhart H, Sheiham A, Tsakos G (2014). Dental caries and growth in school-age children. Pediatrics 133:616-623.
Crossref
|
|
|
|
Al-Rukban MO (2003). Obesity among Saudi male adolescents in Riyadh, Saudi Arabia. Saudi Med. J. 24:27-33.
|
|
|
|
Amin TT, Al-Sultan AI, Ali A (2008). Overweight and obesity and their relation to dietary habits and socio-demographic characteristics among male primary school children in Al-Hassa, Kingdom of Saudi Arabia. Eur. J. Nutr. 47:310-318.
Crossref
|
|
|
|
Bagherian A, Sadeghi M (2013). Association between dental caries and age-specific body mass index in preschool children of an Iranian population. Indian J. Dent. Res. 24:66-70.
Crossref
|
|
|
|
Baker S, Barlow S, Cochran W, Fuchs G, Klish W, Krebs N, Strauss R, Tershakovec A, Udall J (2005). Overweight children and adolescents: a clinical report of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 40:533-543.
Crossref
|
|
|
|
Barlow SE (2007). Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 120(4):164-192.
Crossref
|
|
|
|
Bassali R, Waller JL, Gower B, Allison J, Davis CL (2010). Utility of waist circumference percentile for risk evaluation in obese children. Int. J. Pediatr. Obes. 5:97-101.
Crossref
|
|
|
|
Broadbent JM, Thomson WM (2005). For debate: problems with the DMF index pertinent to dental caries data analysis. Commun. Dent. Oral Epidemiol. 33(6):400-409.
Crossref
|
|
|
|
CDC (2010). CDC. Information on overweight and obesity.
View
|
|
|
|
Cinar AB, Murtomaa H (2011). Interrelation between obesity, oral health and life-style factors among Turkish school children. Clin. Oral Investig. 15:177-184.
Crossref
|
|
|
|
Collison KS, Zaidi MZ, Subhani SN, Al-Rubeaan K, Shoukri M, Al-Mohanna FA (2010). Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health 10:234.
Crossref
|
|
|
|
Duncan S, Duncan EK, Fernandes RA, Buonani C, Bastos KD, Segatto AF, Codogno JS, Gomes IC, Freitas IF (2011). Modifiable risk factors for overweight and obesity in children and adolescents from São Paulo, Brazil. BMC Public Health. 11: 1.
Crossref
|
|
|
|
Dye BA, Shenkin JD, Ogden CL, Marshall TA, Levy SM, Kanellis MJ (2004). The relationship between healthful eating practices and dental caries in children aged 2–5 years in the United States, 1988-1994. J. Am. Dent. Assoc. 135:55-66.
Crossref
|
|
|
|
El Mouzan MI, Foster PJ, Al Herbish AS, Al Salloum AA, Al Omer AA, Qurachi MM, Kecojevic T (2010). Prevalence of overweight and obesity in Saudi children and adolescents. Ann. Saudi Med. 30:203-208.
Crossref
|
|
|
|
El-Hazmi MA, Warsy AS (2002). The prevalence of obesity and overweight in 1-18-year-old Saudi children. Ann. Saudi Med. 22:303-307.
|
|
|
|
Esmaillzadeh A, Mirmiran P, Azadbakht L, Etemadi A, Azizi F (2006). High prevalence of the metabolic syndrome in Iranian adolescents. Obesity 14:377-382
Crossref
|
|
|
|
Gidding SS, Dennison BA, Birch LL, Daniels SR, Gilman MW, Lichtenstein AH, Rattay KT, Steinberger J, Stettler N, Van Horn L (2006). Dietary recommendations for children and adolescents: a guide for practitioners. Pediatrics 117:544-559.
Crossref
|
|
|
|
Granville-Garcia AF, De Menezes VA, De Lira PI, Ferreira JM, Leite-Cavalcanti A (2008). Obesity and dental caries among preschool children in Brazil. Revista de Salud Pública. 10:788-795.
Crossref
|
|
|
|
Hanley AJ, Harris SB, Gittelsohn J, Wolever TM, Saksvig B, Zinman B (2000). Overweight among children and adolescents in a Native Canadian community: prevalence and associated factors. Am. J. Clin. Nutr. 71:693-700.
|
|
|
|
Hetherington MM, Cecil JE (2010). Gene-environment interactions in obesity. Forum Nutr. 63:195-203.
Crossref
|
|
|
|
Hong L, Ahmed A, Mccunniff M, Overman P, Mathew M (2008). Obesity and dental caries in children aged 2-6 years in the United States: National Health and Nutrition Examination Survey 1999-2002. J. Public Health Dent. 68:227-233.
Crossref
|
|
|
|
Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N(2012). Body mass index and dental caries in children and adolescents: a sys¬tematic review of literature published 2004 to 2011. Syst. Rev. 1:57.
Crossref
|
|
|
|
Jagadesan S, Harish R, Miranda P, Unnikrishnan R, Anjana RM, Mohan V (2014). Prevalence of overweight and obesity among school children and adolescents in Chennai. Indian Pediatr. 51:544-549.
Crossref
|
|
|
|
Janssen I, Katzmarzyk PT, Ross R (2002). Body mass index, waist circumference, and health risk: evidence in support of current National Institutes of Health guidelines. Arch. Intern. Med. 162:2074-2079.
Crossref
|
|
|
|
Janssen I, Katzmarzyk PT, Ross R (2004). Waist circumference and not body mass index explains obesity-related health risk. Am. J. Clin. Nutr. 79:379-384.
|
|
|
|
Kaiser LI, Melgar-Quin˜onez HR, Lamp CL, Johns MC, Sutherlin JM, Harwood JO (2002). Food security and nutritional outcomes of preschool-age Mexican- American children. J. Am. Diet. Assoc. 102:924-929.
Crossref
|
|
|
|
Li C, Ford ES, Mokdad AH, Cook S (2006). Recent trends in waist circumference and waist-height ratio among US children and adolescents. Pediatrics 118:e1390-8.
Crossref
|
|
|
|
Li LW, Wong HM, Peng SM, McGrath CP (2015). Anthropometric measurements and dental caries in children: a systematic review of longitudinal studies. Adv. Nutr. 6(1):52-63.
Crossref
|
|
|
|
Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy SM (2007). Dental caries and childhood obesity: roles of diet and socioeconomic status. Commun. Dent. Oral Epidemiol. 35:449-458.
Crossref
|
|
|
|
Mirmiran P, Sherafat-Kazemzadeh R, Jalali-Farahani S, Azizi F (2010). Childhood obesity in the Middle East: a review/Revue sur l'obésité de l'enfant au Moyen-Orient. Eastern Mediterranean health J. 16:1009.
|
|
|
|
Mwaikambo SA, Leyna GH, Killewo J, Simba A, Puoane, T (2015). Why are primary school children overweight and obese? A cross sectional study undertaken in Kinondoni district, Dar-es-salaam. BMC public health. 15:1.
Crossref
|
|
|
|
Nadeau KJ, Maahs DM, Daniels SR, Eckel RH (2011). Childhood obesity and cardiovascular disease: links and Prevention strategies. Nat. Rev. Cardiol. 8:513-525.
Crossref
|
|
|
|
Ogden CL, Carroll MD, Kit BK, Flegal KM (2012). Prevalence of obesity and trends in body mass index among US children and adolescents, 1999-2010. Jama. 307:483-490.
Crossref
|
|
|
|
Oliveira LB, Sheiham A, Bonecker M (2008). Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur. J. Oral Sci. 116:37-43.
Crossref
|
|
|
|
Pabayo R, Gauvin L, Barnett TA, Nikiéma B, Séguin L (2010). Sustained active transportation is associated with a favorable body mass index trajectory across the early school years: findings from the Quebec Longitudinal Study of Child Development birth cohort. Prev. Med. 50:S59-S64.
Crossref
|
|
|
|
Patnaik L, Pattanaik S, Sahu T, Rao EV (2015). Overweight and Obesity among Adolescents, A Comparative Study between Government and Private Schools. Indian Pediatr. 52:779-781.
Crossref
|
|
|
|
Patnaik S, Patnaik L, Patnaik S, Hussain M (2011). Prevalence of overweight and obesity in a private school of Orissa, India. Internet J. Epidemiol. 10:1.
|
|
|
|
Reifsnider E, Mobley C, Mendez DB (2004). Childhood obesity and early childhood caries in a WIC population. J. Multicult. Nurs. Health 10:24.
|
|
|
|
Shahraki T, Shahraki M, Omrani Mehr S (2013). As¬sociation between body mass index and caries frequency among Zahedan elemen¬tary school children. Int. J. High Risk Behav. Addict. 2:122-125.
Crossref
|
|
|
|
Sheller B, Churchill SS, Williams BJ, Davidson B (2009). Body mass index of children with severe early childhood caries. Pediatr. Dent. 31:216-221.
|
|
|
|
Spiegel KA, Palmer CA (2012). Childhood dental caries and childhood obesity: different problems with overlapping causes. Am. J. Dent. 25:59-64.
|
|
|
|
Werner SL, Phillips C, Koroluk LD (2012). Association between childhood obesity and dental caries. Pediatr. Dent. 34:23-27.
|
|
|
|
Willershausen B, Haas G, Krummenauer F, Hohenfellner K (2004). Relationship between high weight and caries frequency in German elementary school children. Euro. J. Med. Res. 9:400-404.
|