Case Report

ABSTRACT
Dens invaginatus is a developmental malformation resulting from the invagination of the enamel organ into the dental papilla. Type 1 invagination, is most common form. However, it may be easily overlooked because of the absence of any significant clinical signs of this anomaly. Since the risk of necrosis and pulp complication is higher in such dental malformation, an early identification of the affected tooth is important and the prophylactic management is recommended. The aim of this report is to describe an unusual case presenting invagination affecting four teeth. The clinical and radiographic features will also be highlighted and the prophylactic treatment explained.
Key words: Anomalous teeth, dens in dente, dens invaginatus, maxillary central incisor.
INTRODUCTION
Dens invaginatus is a dental malformation caused by an infolding of the enamel organ into the adjacent dental papilla during the development of the tooth before calcification has occurred (Rajasekharan et al., 2014).
The exact aetiology of dens invaginatus is unclear. Uncontrolled growth of a portion of the enamel epithelium, external forces exerted on the developing tooth germ by the growing dental arch, and adjacent developing tooth germs have been suggested to explain this dental malformation. Other theories include, trauma and infection during tooth development was also proposed to explain these dental anomalies. In addition, there is significant evidence suggesting a genetic component in the development of dens invaginatus (Bose, 2014).
This developmental malformation is more common than we generally thought. The prevalence of the dens invaginatus varies between 0.3 and 10%. The wide ranges of the prevalence are explained by the different inclusion and exclusion criteria to diagnosis dens invaginatus and the geographical difference of the population studied (Çolak et al., 2012).
Maxillary lateral incisor is the most commonly affected teeth (90%), frequently with bilateral occurence (43%), followed by central incisors, canines, premolars and molars. Invagination of mandibular incisors is rare and it has only been reported in isolated case reports (Bose, 2014).
The clinical presentation of dens invaginatus depends to its severity. It can range from a pronounced cingulum or occlusal pit to a deep foramen caecum that may be the first clinical sign of an invaginated tooth (Chandramani, 2012; Çolak et al., 2012). Other changes in the form can be observed, including a peg or barrel shaped anatomy, incisal notching, an increased labio-lingual or mesio-distal dimension and a prominent palatal cingulum (Bose, 2014).
The most commonly used classification system was proposed by Oehlers (1957) and Çolak et al. (2012). Based on the radiographic appearance of the invagination, three-forms of the anomaly are described.
Type I is a minor form with an enamel-lined infolding confined to the crown, not extending beyond the amelo-cemental junction.
Type II extend below the cemento-enamel junction and ends in a blind sac.
It does not communicate with the periodontal ligament but may communicate with the pulp space.
Type III invaginations extend through the root and communicate with the periodontal ligament laterally (type IIIa) or at the apical foramen (type IIIb).
Despite the fact that the type 1 invagination is the most common form, (73%) there is today a lack of studies and reports how to manage such invaginations.
However, early management of such malformations is crucial. Indeed, invaginations are inaccessible to cleaning. Therefore, the risk of micro-organism to reach and to infect the pulpal tissue is important, that may lead to pulp necrosis (Bose, 2014; Çolak et al., 2012)
In this present paper, we report an unusual case presenting four invaginations on the maxillary incisors in which prophylactic management was proposed.
CASE REPORT
A healthy, 22 year-old female patient was referred to our department by the patient’s general dental practitioner for the extraction of the wisdom teeth. The routinely clinical examination, showed a pronounced cingulum and a deep foramen caecum on the palatal surface of the maxillary incisors.
The gentle probing of the foramen revealed a carious lesion presenting rough surface covered with plaque and discolored tissue around the foramen (Figure 2).
Moreover, the teeth respond normally to the cold vitality test, with no pain on percussion and palpation. Moreover the periodontal probing depths were not >2 mm.
The radiographic examination revealed a deep fissuring pointing towards the pulp with a radiolucent pocket surrounded by a radio- opaque enamel border revealing the presence of an invagination. The radiographic appearance of the invagination is confined to the crown, not extending beyond the amelo–cemental junction (Figure 3). Therefore, a diagnosis of dens invaginatus (Oehlers’ Type 1) was established on the maxillary incisors and prophylactic managements of these invaginations were proposed to the patient in order to prevent any pulpal complications.
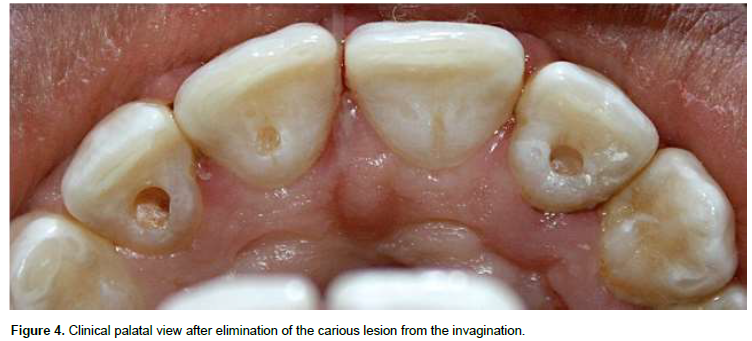
After buccal infiltration using 3% mepivacaine with epinephrine (Medicaine, Médis, Tunisia), the lumen of the invagination was reamed using a round bur. All softened and carious lesion were also removed (Figure 4).
The next step was disinfecting the cavities using 2% chlorhexidine and a flow composite resin was used to seal the cavities as recommended by the manufacturer (Nextcomp flow, Meta Biomed, Chungbuk, Korea) (Figure 5).
DISCUSSION
Invagination is more common than we thought. Due to geographical differences and the inclusion/exclusion criteria, it’s prevalence varies between 0.3 and 10% (Çolak et al., 2012). Dens invaginatus (Oehlers’ type 1) appears to be the most common from (73%) among this malformation (Çolak et al., 2012). As reported by several authors, maxillary lateral incisor is the most commonly affected tooth (90%) frequently with bilateral occurence (43 %) followed by central incisors (Bose, 2014). This case, provide an uncommon finding with four invaginations affecting maxillary incisors. As far as we know, there is no report in the literature of such clinical configuration. It could be the first case described in the literature.
Clearly observed in this case the deep foramen caecum is always the first clinical sign to suspect an invaginated tooth (Chandramani, 2012; Çolak et al., 2012). Nevertheless, despite the presence of a prominent palatal cingulum and an increased labio-lingual dimension on the affected tooth, the crown remains normally shaped (Figures 1 and 2). It is in agreement with Oehlers who described three different morphological types of the invaginated teeth: Normal-shaped crowns, peg shaped crowns and crowns with Talon cusp.


Until today, there is a lack of consensus on the criteria describing invaginated teeth. For some authors, palatal notch or pit constitutes an invagination, whereas, others consider the presence of a deep foramen caecum as an invagination. This lack of consensus for describing invagination is one of the reasons that explains the wide range of the prevalence of the invaginated teeth 0.3 to 10% (Çolak et al., 2012)
Oehlers classification is based on the radiological aspect of the invagination. Clearly observed on the preoperative radiograph, Type 1 invagination is defined as a minor form with an enamel-lined infolding confined to the crown, not extending beyond the amelo-cemental junction (Figure 3). Although no clinical evidence of the presence of an invagination on the left central incisors, the close radiological aspect between the two central incisors leads to consider it as a one.


It is well documented that the risk of pulp necrosis or complication on invaginated tooth is high. Indeed, due to the clinical and histologic presentation, the invagination is inaccessible to cleaning and micro-organism penetrates
easily through a hypominerelized enamel. It has been also shown that channels may exist between the invagination and the pulp which may lead the pulp to be infected (Chandramani, 2012).
For these reasons, a preventive approach was recommended to treat such dental malformations (Thakur et al., 2014). Composite restoration procedure has been widely used to seal the lumen of the invagination. Moreover, the use of calcium hydroxide to cover the bottom and the buccal wall of the lumen and the use of glass ionomer as a definitive restoration were also described (Thakur et al., 2014).
When the tooth is vital, with no signs of pulpal complications and when the prophylactic management is carefully performed, success can be expected in type 1 invagination with a high success rates. Contrarily to the prophylactic management of type 2 invagination which appears to be less predictable (Çolak et al., 2012; Thakur et al., 2014).
CONCLUSION
Dentist may be unfamiliar with the invaginated teeth. Therefore, knowing the clinical and radiographic manifestations is important to early identify this dental malformation. Care should be taken to properly manage these invaginations in order to avoid any plulpal complications. Composite restoration provides a simple way to prophylactically treat such lesions. When the procedure is carefully performed, with an early identification, success can be expected with a high survival rate. This present report shows a rare case presenting four type 1 invaginations.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
REFERENCES
|
Bose BB (2014). A Variant Form of Dens Invaginatus in Permanent Maxillary Canine. Int. J. Dental Sci. Res. 2(4B):1-3. |
|
|
Chandramani B (2012). Dens Invaginatus: A Radiographic Analysis. |
|
|
Çolak H, Tan E, Aylıkçı BU, Uzgur R, Turkal M, Hamidi MM (2012). Radiographic study of the prevalence of dens invaginatus in a sample set of Turkish dental patients. J. Clin. Imaging Sci. P 2. |
|
|
Rajasekharan S, Martens L, Vanhove C, Aps J (2014). In vitro analysis of extracted dens invaginatus using various radiographic imaging techniques. Eur. J. Paediatr. Dent. 15(3):265-270. |
|
|
Thakur S, Thakur NS, Bramta M, Gupta M (2014). Dens invagination: A review of literature and report of two cases. J. Natural Sci. Biol. Med. 5(1):218. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


