Full Length Research Paper
ABSTRACT
Incidence of chronic kidney disease of unknown etiology (CKDu) has emerged in South Asia and sub-Saharan Africa over last few years. CKDu is not attributed to diabetes, hypertension or other known causes of CKD. It affects younger individuals and is usually asymptomatic till advanced stages. Organochlorine pesticides (OCPs) are one of the proposed etiologies of CKDu. The present study was done to evaluate the serum level of certain commonly encountered OCPs (α-HCH, β-HCH, g-HCH, total HCH, Aldrin, Dieldrin, α- endosulfan, β-endosulfan, p,p’-DDT, p,p’-DDE) and total pesticide load (TPL) in patients with CKDu in comparison to patients with CKD of known etiology (CKDk) and to assess their correlation, if any. It was a case-control, cross-sectional study conducted in East Delhi. Subjects within the age group 18-60 years were enrolled under 3 groups: Group I: Healthy controls (n=30), Group II: Patients with CKDu (n=30), and Group III: Patients with CKDk (n=30). Detailed history, physical examination and routine investigations were done. OCP levels were estimated in all subjects by high performance liquid chromatography. The median serum levels of all OCPs were found higher in patients of CKDu in comparison to other groups. The difference was statistically significant for α-HCH, β-HCH, total HCH, α-endosulfan, p,p’-DDE and TPL. Higher fraction of CKDu patients presented in stage V CKD (66.34%). The presence of higher serum levels of OCP in patients with CKDu in comparison to CKDk at their corresponding CKD stages indicates their possible role in the etiopathogenesis of CKDu.
Key words: CKD of unknown etiology, etiopathogenesis, organochlorine pesticides.
INTRODUCTION
CKD a major health problem throughout the world, both for the number of patients and cost of treatment involved. Over the last decade, a new form of CKD, that is, CKDu has risen in some areas of Asia, especially Sri Lanka, and sub-Saharan Africa (Centre for Science and Environment (CSE)/Pollution Monitoring Laboratory (PML), 2012). CKDu has also been reported from UK (Lightstone et al., 1995). Data from CKD Registry of India revealed that CKDu is the second most common cause of CKD, next only to diabetes mellitus (Rajapurkar et al., 2012). Prevalence CKDu is approximately 10% worldwide and 16.4% in the Indian subcontinent (Rajapurkar et al., 2012; Ball et al., 2001; Parameswaran et al., 2011). Although, no specific agents have been identified, environmental toxins and heavy metals are thought to be the culprit behind CKDu (Rajapurkar et al., 2012). It is comparatively a slowly progressive disease starting in 2nd to 3rd decade, and usually remains asymptomatic till advanced stages. Peripheral edema and hypertension are less commonly encountered features of CKDu, which creates a trouble for its diagnosis. It resembles tubulo-interstitial nephritis similar to other toxic nephropathies and less glomerular involvement, unlike CKDk (Chandrajith et al., 2011). The affected individuals are mainly young male individuals exposed to fertilizers, pesticides and industrial chemicals containing OCPs.
OCPs such as hexachlorocyclohexane (HCH) and its isomers, aldrin, dieldrin, endosulfan α, endosulfan β, dichloro-diphenyl-trichloro-ethane (p,p-DDT) and dichloro-diphenyl-dichloro-ethylene (p,p-DDE) are mostly halogenated alkanes and alkenes that are bioactivated in kidney during the course of their metabolism and may induce kidney damage (Crinnion, 2009). OCPs cause increase in oxidative stress, as supported by an increase in markers of oxidative damage such as malondialdehyde, protein carbonyl, advanced oxidation protein products, leading to renal toxicity.
Humans are exposed to OCPs mainly via contaminated foods and bioaccumulate these lipophilic and hydrophobic pollutants in fatty tissues (Agency for Toxic Substances and Disease Registry (ATSDR), 2002; Kiviranta et al., 2005). No significant literature is available regarding association of higher level of serum OCPs with CKDu. Based on the prevalence of OCPs in general population, and a high prevalence of CKDu in Indian subcontinent, it can be hypothesized that OCPs may be one of the several etiologies of CKDu and this hypothesis needs further investigations to open the hidden doors of etiology of CKDu.
METHODOLOGY
The present study was a case-control, cross-sectional study, conducted during study period of November 2013 to April 2015 in East Delhi, after obtaining ethical clearance from Institutional Ethical Committee (IEC). The total sample size was 90. Subjects of 18-60 years were recruited from patients attending the Medicine Out-Patient-Department, Nephrology Clinic, Medical Emergency, or those who were admitted in the Medical wards. Healthy controls were selected from the relatives of patients and the staff of hospital. Subjects were enrolled under three groups having 30 individuals in each group as following: Group I: Healthy controls (HC) (n=30), Group II: Patients with CKDu (n=30), and Group III: Patients with CKDk (n=30).
Routine investigations and urinary protein excretion estimation were done in all individuals, after satisfying inclusion criteria. The following case definitions were followed:
CKDk: Individuals having CKD due to DM, HTN, hereditary causes, glomerulonephritis, obstructive uropathy, renovascular disease, graft dysfunction, tubulointerstitial disease due to administration of nephrotoxic drugs or any other known cause of CKD.
CKDu: Participants who had persistent albuminuria, that is, albumin-creatinine ratio (ACR) ≥30 mg/g or 24 h urinary protein >500 mg/day, were considered to have CKDu if they satisfied the following criteria: (1) No past history of glomerulonephritis, pyelonephritis, renal calculi, snake bite or any other known cause of CKD; (2) No history of diabetes mellitus; (3) Hypertensive patients were recruited, only if on pharmacological treatment, blood pressure below <140/90 mmHg; if not on treatment for hypertension, blood pressure below <160/100 mmHg.
GFR was calculated by following Modified Diet in Renal Disease (MDRD) study equation as follow:
Estimated GFR (mL/min/1.73 m2) = 1.86 × (Pcr)-1.154 × (age)-0.203 (Multiply by 0.742 for women) Patients with acute poisoning with OCPs were not enrolled in the present study to prevent bias. Serum OCP levels were measured in parts per billion (ppb) and their extraction was done using high performance liquid chromatography (HPLC) (Dua and Bush, 1984). Cleanup was done by the USEPA method 3620B using activated Florisil. Quantitative analysis was done by comparison of the peak area with those obtained from a chromatogram of a known mixed OCP concentration. Limits of detection for all components were 4 pg/mL. Few randomly selected samples, approximately 20%, were processed in duplicates for quality control check.
In the present study, serum levels of total 9 OCPs (α-HCH, β-HCH, g-HCH, α-endosulfan, β-endosulfan, aldrin, dieldrin, p,p’-DDE and p,p’-DDT) were measured. In addition, total hexachlorocyclohexane (HCH) and total pesticide load (TPL) were also evaluated.
Statistical analysis
All values were reported as either mean ± standard deviation or percentiles, depending upon distribution of data. Differences between mean were compared using one-way ANOVA followed by Tukey’s test. The association of estimated GFR with OCP levels was obtained by calculating co-efficient of correlation. P-value < 0.05 was taken as significant.
RESULTS
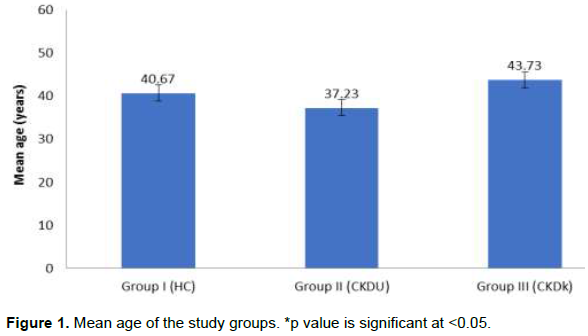
The mean age of subjects in group I, group II and group III was 40.67±12.65, 37.23±12.57 and 43.73±11.40 years, respectively (Figure 1). CKDu had predilection for younger age group. Male: female ratio was 1:2. Females tend to have higher concentration of most OCPs. BP was significantly higher in subjects in group III when compared with the subjects in groups I and II.
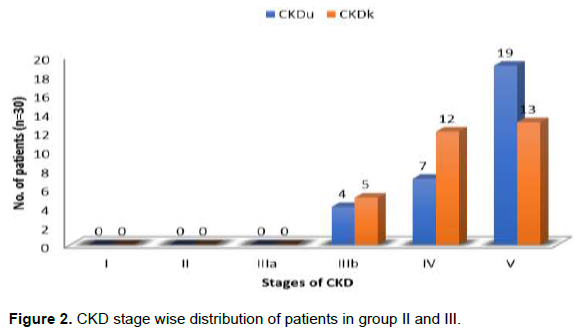
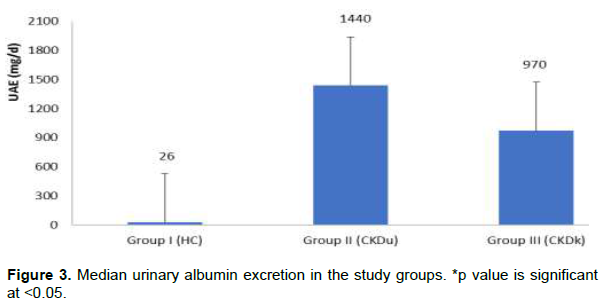
In the present study, 63.34% of patients in CKDu had stage V CKD as compared to 43.33% patients of CKD stage V in CKDk group (Figure 2). Median value of urinary albumin excretion (UAE) was found higher in CKD patients in comparison to healthy controls (Figure 3).
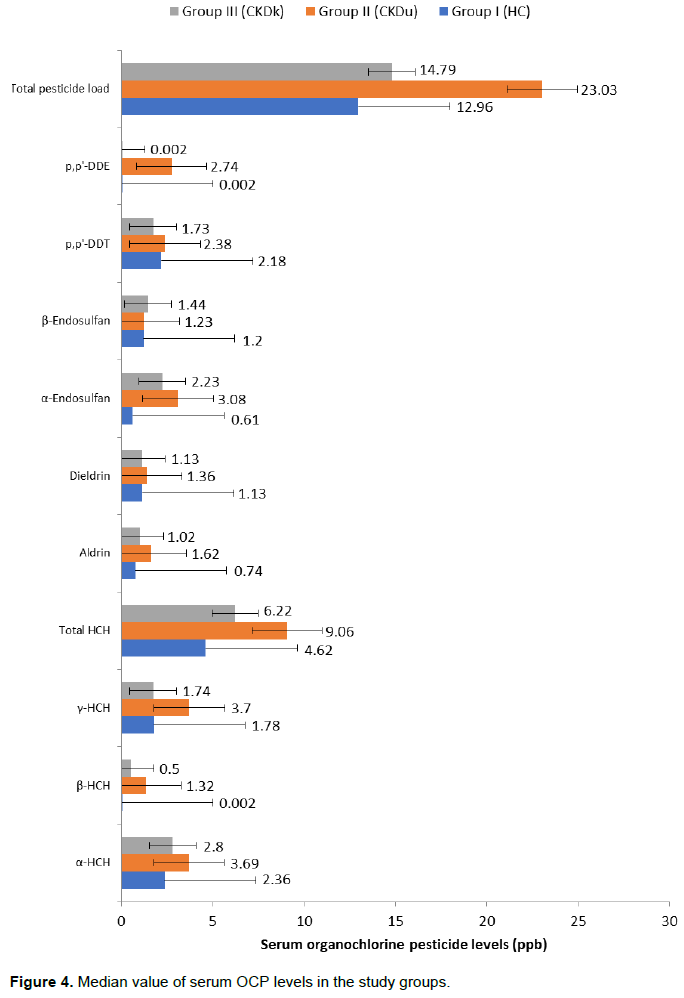
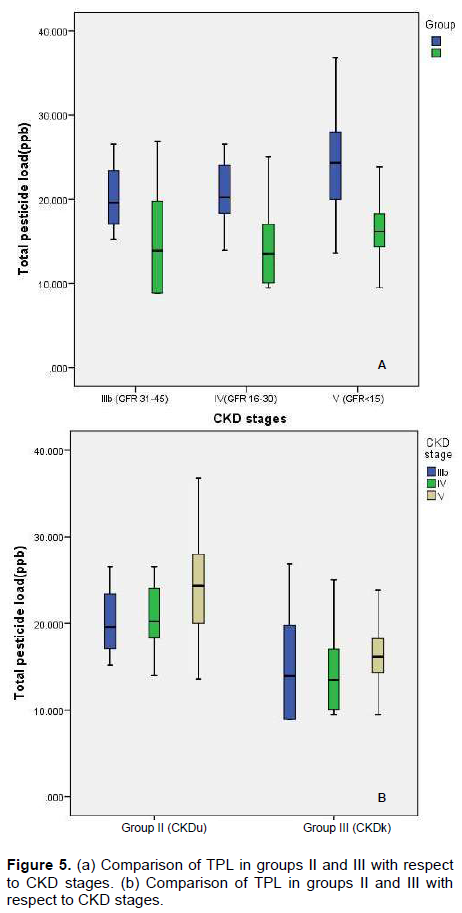
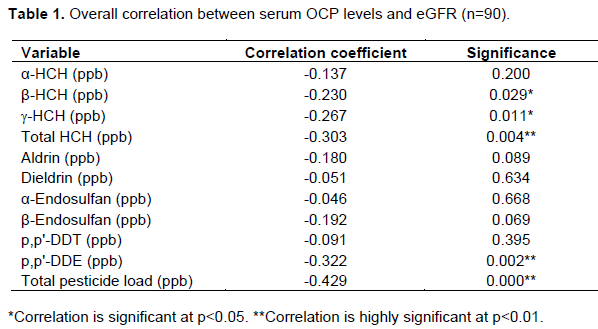
The median OCP levels were higher in CKDu group as compared to patients in HC and CKDk (Figure 4). Serum levels of α-HCH, β-HCH, total HCH, α-endosulfan, p,p’-DDE and TPL were significantly higher in subjects of group II (CKDu) as compared to other study groups (I and III) and the difference was statistically significant (p=<0.05). We observed that there were high serum levels of OCPs in CKDu compared to CKDk at all respective CKD stages (Figure 5a and b). eGFR was found lower in CKD patients when compared with healthy controls and declined with advancing stage of CKD. A negative correlation of eGFR with serum OCP levels was found, which was statistically significant with β-HCH, g- HCH, total HCH, p.p’-DDE and TPL (Table 1).
DISCUSSION
There exists a lot of disparities and inadequacy in the available literature with regard to the etiology of CKDu. No significant literature is available regarding the association of higher levels of serum OCPs with CKDu. There is growing knowledge that a higher level of serum OCPs might be one of the causative factors that may initiate and promote the progression of CKDu due to an imbalance in oxidative stress. Keeping this hypothesis in mind, the present study was done to assess the relationship between serum OCP levels with CKDu and to correlate them. In the present study levels of nine OCPs (α-HCH, β-HCH, g-HCH, α-endosulfan, β-endosulfan, aldrin, dieldrin, p,p’-DDE and p,p’-DDT) were estimated. In addition, total hexachlorocyclohexane (HCH) and total pesticide load (TPL) were also calculated.
The mean age in HC, CKDu and CKDk was 40.67±12.65, 37.23±12.57 and 43.73±11.40 years, respectively. In the present study, CKDu had predilection for a younger age group, in comparison to CKDk. This was in accordance to previous study of Rajapurkar et al. (2012), who also found that CKDu predominantly affects younger individuals. Jayatilake et al. (2013) also encountered younger population involvement in CKDu.
Females were found to have comparatively higher concentrations of DDTs than males and which might be due to the difference in metabolism (Dirtu et al., 2006; Kalantzi et al., 2011; Porta et al., 2012). Study by Jayatilake et al. (2013), in accordance with the present study, also found a higher prevalence of CKDu in females, that is, 16.9% compared to males which were 12.9%.
In the present study, significantly greater proportion (63.34%) of patients in group II (CKDu) had stage V CKD as compared to group III (CKDk) (43.33%). This might be due to the fact that CKDu is slowly progressive which usually remains asymptomatic until late stages (Jayatilake et al. 2013).
In the present study, median serum levels of all OCPs were higher in group II (CKDu) patients as compared to subjects in group I (HC) and group III (CKDk) and were increasing with the increasing stage of CKD. Serum levels of α-HCH, β-HCH, total HCH, α-endosulfan and p,p’-DDE were significantly higher in group II (CKDu) patients as compared to other study groups (I and III) and the difference was statistically significant (p=<0.05). The TPL, which represents sum of all pesticides detected, was also observed to be higher in patients of group II (CKDu) and the difference was highly significant (p=<0.001).
Overall, a negative correlation of eGFR with serum OCP levels, which was statistically significant for β-HCH, g-HCH, total HCH, p.p’-DDE and TPL.
With the growing evidence of role of OCPs in causing CKDu, this study indicates the importance of investigating the association of serum OCP levels in CKDu patients in a larger population. CKDu is a slowly progressive disease, somewhere starting in 2nd to 3rd decade, and usually asymptomatic till advanced stages. Peripheral edema and hypertension are not encountered frequently. These findings present a challenge for developers of CKD detection programs, as these patients do not exhibit the usual parameters that define high risk for CKD such as hypertension or diabetes and patients usually seek medical consultation in advanced stages.
CONCLUSION
CKDu affects individuals of younger age group as compared to CKDk and has a female preponderance. Patients of CKDu have higher serum OCP levels when compared with the patients of CKDk. There levels increased with the increasing stage of CKD indicating worsening of renal dysfunction with higher serum OCP levels. Patients of CKDu present in advanced stages of CKD in comparison to the patients of CKDk patients. Severity of renal dysfunction is more in CKDu patients when compared with patients of CKDk, which manifests as lower hemoglobin and serum albumin concentrations, higher blood urea and serum creatinine levels, and higher urinary albumin excretion. eGFR shows progressive decline with advancing stage of chronic kidney disease and this decline is more in CKDu affected patients in comparison to CKDk patients. There is a negative correlation between serum OCP levels and eGFR, which was statistically significant (p=<0.05) with β-HCH, g-HCH, total HCH, p,p'-DDE and total pesticide load.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors thank Department of Biochemistry of UCMS and GTB hospital for their support cooperation.
REFERENCES
|
Agency for Toxic Substances and Disease Registry (ATSDR) (2002). Toxicological profile for aldrin/dieldrin. Atlanta: US Department of Health and Human Services, Public Health Service, 2002. |
|
|
Ball S, Lloyd J, Cairns T (2001). Why is there so much end-stage renal failure of undetermined cause in UK Indo-Asians? QJM 94:187-193. |
|
|
Centre for Science and Environment (CSE)/Pollution Monitoring Laboratory (PML) (2012). Environmental contamination and its association with Chronic Kidney Disease of Unknown Etiology in North Central Region of Sri Lanka, 2012. |
|
|
Chandrajith R, Nanayakkara S, Itai K (2011). Chronic kidney diseases of uncertain etiology (CKDue) in Sri Lanka: geographic distribution and environmental implications. Environmental Geochemistry and Health 33(3):267-278. |
|
|
Crinnion WJ (2009). Chlorinated Pesticides: Threats to health and importance of detection. Alter Medicine Review 14:347-359. |
|
|
Dirtu AC, Cernat R, Dragan D (2006). Organohalogenated pollutants in human serum from Iassy, Romania and their relation with age and gender. Environment International 32(6):797-803. |
|
|
Dua VK, Bush CA (1984). Resolution of some glycopeptides of hen ovalbumin by reverse-phase high-pressure liquid chromatography. Analytical Biochemistry 137(1):33-40. |
|
|
Jayatilake N, Mendis S, Maheepala P, Mehta FR (2013). Chronic kidney disease of uncertain aetiology: prevalence and causative factors in a developing country. BMC Nephrology 14(1):180-189. |
|
|
Kalantzi OI, Geens T, Covaci A, Siskos PA (2011). Distribution of polybrominated diphenyl ethers (PBDEs) and other persistent organic pollutants in human serum from Greece. Environment International 37:349-353. |
|
|
Kiviranta H, Tuomisto JT, Tuomisto J, Tukiainen E, Vartiainen T (2005). Polychlorinated dibenzofuranes, and biphenyls in the general population in Finland. Chemosphere 60:854-869. |
|
|
Lightstone L, Rees AJ, Tomson C, Walls J, Winearls CG, Feehally J (1995). High incidence of end-stage renal disease in Indo-Asians in the UK. QJM 88(3):191-195. |
|
|
Parameswaran S, Geda SB, Rathi M (2011). Referral pattern of end-stage renal disease patients and its impact on outcome at a public sector hospital. National Medical Journal of India 24(4):208-213. |
|
|
Porta M, López T, Gasull M (2012). Distribution of blood concentrations of persistent organic pollutants in a representative sample of the population of Barcelona in 2006, and comparison with levels in 2002. Science of the Total Environment 423:151-161. |
|
|
Rajapurkar MM, John GT, Kirpalani AL (2012). What do we know about chronic kidney disease in India: first report of Indian CKD Registry. BMC Nephrology 13:1-8. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


