Full Length Research Paper

ABSTRACT
Since December 2019, COVID-19 disease caused by SARS-CoV-2 virus has spread world-wide as pandemic causing large number of infected persons and lot of deaths of COVID patients. There is currently no definite medicine for treatment of the disease as well as any preventive measure. With the progress of multiplication of viruses in the human, activation and amplification of host immune response take place causing massive release of varieties of cytokines like interleukin (IL)-1, IL-6, IL-17, etc., and different types of interferons (IFNs), tumour necrosis factor (TNF) to form cytokine storm. From studies of COVID-19 patients in hospital, it has also been noted that uncontrolled inflammation due to elevated levels of cytokine (cytokine storm) is responsible for causing severity of the disease. In this article the properties of cytokine, types of cytokine and other details have been discussed. The mechanism of signalling of cytokine to immunity and the reason for causing cytokine storm with its role in causing fatalities in COVID 19 patients have also been pointed out. Low infection of virus persists in upper airway that causes similar to seasonal respiratory illness but with severe infections virus remains in the lower respiratory tract leading to lung injury, acute respiratory distress syndrome (ARDS) and sometimes death. The role of cytokine storm in causing severity of disease has been discussed.
Key words: Cytokine, IL-6, IL-17, IL-33 families, signalling mechanism, immunity, cytokine storm, role in COVID-19.
INTRODUCTION
Cytokines are the most important topics in research on inflammatory diseases since more than fifty years when interferon (IFN) was discovered. Recently this has gained great importance to immunologists, doctors and even to common people in the present pandemic situation of COVID-19. Primarily, cytokines act as lymphocyte growth factors as well as function as pro-inflammatory and anti-inflammatory molecules and also promote immune response to antigen. With the identification of varied functions of cytokine, it has now been played an important role in medicine in various disciplines in diagnostic, prognostic and as therapeutic agents in human disease (Dinarello, 2007).
Cytokines are large group of varied proteins that are released from mammalian cells. These are non-structural proteins with low molecular weight which have a regulatory function on inflammation, immunity and hematopoiesis. Cytokines also fall under a category of signalling molecules. There are other names of cytokines on the basis of cells from which it is produced or from the target of action or on their presumed function. Cytokines made by lymphocytes are called lymphokine, monokine (that made by monocytes), chemokine (showing chemotactic activities), and interleukin (cytokines made by one leukocyte and acting on other leukocytes). The activities of cytokine vary on the basis of their action. When it acts on the cells that secrete them, then it is called autocrine action. When acting on nearby cell, then it shows paracrine action. When cytokine acts on distant cells, then it is called endocrine action. In certain cases, the function of one cytokine is stimulated by different cytokines. Again one cytokine may stimulate its target cells to make additional cytokines (Zhang and An, 2007). With the advancement of research on cytokines, correlations have been found in different diseases like heart disease, Alzheimer’s disease, type 1 and type 2 diabetes, and many other inflammatory disorders.
The molecular weight of cytokines is nearly 30 kDa consisting of about 300 amino acids. Cytokines have a high degree of α helical structure and the molecules share a similar polypeptide fold with four α helical bundles (Gulati et al., 2016). In response to a number of stimuli cytokine, a regulatory protein or glycoprotein, is secreted by white blood cells and various other cells. Interleukins, a type of cytokines, have been designated from IL-1 to IL-29 till now and many more will be discovered in future. When cytokines bind to the receptor of the target cell then it triggers signal transduction pathway which may alter gene expression in the target cell. It has been noted that the affinity between cytokine and receptor is very high so it can exhibit effects on target cells at very low concentration.
Cytokines are similar to hormones in their biological activities like inflammation, acute phase reaction, systemic inflammatory response syndrome, wound healing etc. But there are some differences as cytokines act on a wider spectrum of target cells while hormones act on a specific cell. Again cytokines are not produced in any specialized cells or from any gland. Cytokines are secreted proteins and their sites of action could not be predicted.
CYTOKINE FAMILIES
Cytokine families, produced by various cells of the patients include interleukins, chemokines, colony-stimulating factors (CSF), interferons and the transforming growth factors (TGF) and tumour necrosis factor (TNF) families. All these are structurally related and have sequence similarity but with diverse cytokine functions via important regulatory cell membrane receptor with ligand. The TNF/TNF receptor superfamily contains immuno- regulatory cytokines such as, TNF-α,Lymphotoxins and cellular ligands (CD40L) which does activation of B cell and T cell and also promote apoptosis through another cellular ligand FASL (CD95). Cytokines can be classified into family groups on the basis of secondary and tertiary structure into three main groups.
(i) Long chain-4 helix bundles: IL-6, IL-11, C-NTF, LIF, oncostatin-M (OSM), erythropoietin (EPO), G-CSF, growth hormone (GH), prolactin, IL-10, IFN-alpha, IFN-Beta.
(ii) Short chain 4-helix bundles: IL-2, IL-4, IL-7, IL-9, IL-13, IL-3, IL-5, GMCSF.
(iii) Beta-trefoil structure: In molecular biology the beta trefoil structure is a protein fold consisting of six beta hairpins. Each beta hairpin is formed by two beta strands. Together they form a beta barrel with a triangular “cap” each consisting of three hairpins.
Cytokines can also be classified as Type 1 Cytokine that are produced by Th1 T helper cells and Type 2 produced from Th2 T helper cells. The example of Type 1 cytokines are IL-2, IFN-Gamma (IFN–γ), IL-12 and TNF-Beta. While Type 2 Cytokine includes IL-4, IL-5, IL-6, IL-10 and IL-13.
Many cytokines are secreted through secretory pathways, so they are called Glycoproteins. Genes encoding cytokines produce varieties of cytokines through alternative splicing instead of a single type with slightly different biological activities. The expression of cytokine gene is regulated at the transcriptional level, translational level and during protein synthesis. The main producers of cytokines are helper T cells and macrophages although cytokines can be transiently induced and secreted by all nucleated cells. Once cytokine is released from producer cells their behaviour and circulations are regulated by soluble receptors and specific or unspecific binding proteins. The regulation of cytokines also takes place at the receptor level on target cells as well as on the signalling pathway. Another important peculiar behaviour of cytokines is called Pleiotropic effectors meaning thereby that some cytokines show multiple biological activities or sometimes overlapping activities where a single cell frequently interacts with multiple cytokines showing almost identical responses. Again cytokines may synergize or antagonize the actions of other factors and thus increasing the severity of the infections. Sequence analysis of cytokines of human shows similarity with primates or non-human. Some of the cytokines of primates show about 93 to 99% homology at the protein and nucleic acid level with human sequences.
However, cytokines have an important role in inducing innate immunity for host defence. They play critical role in doing the effective response of leucocytes and parenchymal cells in the detection of microorganisms with the help of receptors. Different cytokine families are discussed subsequently.
INTERLEUKIN FAMILY
Interleukin is a naturally occurring protein in the human and animal body that takes part in controlling the immune system of the body. There are varieties of interleukin forming a family which is again a subset of a cellular messenger called cytokines. Interleukins are produced rapidly within the cells after getting a stimulus from any infectious agent. As soon as the interleukin is produced, it attacks the target cell through a receptor molecule present on the surface of the cell. Interleukins also have pro-inflammatory and anti-inflammatory properties. The primary function of interleukins is to modulate growth, differentiation and activation during inflammation and to give immune responses (Angel et al., 2020). Its production is a self-limited process and mRNA for the synthesis of interleukin is unstable thus giving a transient synthesis. It sometimes influences other interleukin synthesis as for example, interleukins of IL-1 promotes lymphocyte activation leading to a release of another new type of interleukin IL-2. The interleukins were first identified in 1970 in leukocytes and their actions were noted on other leukocytes thus its name was given as interleukins because its action was found between leukocytes. Later it was found that interleukins may be synthesised by many other cells (Angel et al., 2020), (Encyclopaedia Britannica). So far 40 types of interleukins are known and they are designated numerically from IL-1 to IL-40. Only some important types will be discussed here.
Interleukin-6 family
This family consists of IL-6, IL-11, ciliary neurotrophic factor (CNTF), leukemia inhibitory factor (LIF), oncostatin M (OSM), cardiotrophin-1 (CT-1), cardiotrophin-like-cytokine (CLC) and IL-27. Members of this family use the common signalling receptor subunit glycoprotein of 130 kDa (gp130). gp130 is actually a signal inducer. The functions of these members are (i) stimulation of B- cells; (ii) induction of the hepatic acute phase proteins; (iii) metabolic and neurotrophic functions; (iv) IL-6 receptor that neutralizes monoclonal antibody (Tocilizumab) used for the treatment of autoimmune disorders (Tanaka et al., 2014); and (iv) form a large family of mediators for co-ordinating the immune system and many other physiological functions (Rose-John 2018). Interleukin-6 was originally identified as a factor for inducing immunoglobin production in activated B cells and so it was sometimes called B cell differentiation factor or B-cell stimulatory factor. But IL-6 has been found to show many functions outside the B-lymphocyte system like other interleukins or cytokines. So its function can be called pleiotropic meaning thereby that one type of protein or gene shows multiple functions. In other words, it is used by various cells or the cascade-like signalling function that affects various targets. Sometimes they function in a redundant manner that is multiple cytokines exert similar activities utilising common receptor subunits and common intracellular signalling pathways. Blockade of IL-6 family cytokines has been found to be beneficial in auto-immune diseases, but with bacterial infections and metabolic side effects have been observed. Blocking IL-6 family of cytokines has also been found to be beneficial in autoimmune diseases, but there is a risk of bacterial infections and metabolic side effects (Stephan, 2018).
Molecular studies of various cytokines including IL-6 have revealed the importance of their role in controlling diseases and in the formation of receptor complex. Its importance has increased to a great extent after molecular cloning of IL-6 by Hirano et al. (1986) and Hirano (2014).
With the advancement of molecular cloning and structural analysis of receptors for these cytokines it has been established that a multi-chain receptor complex is formed by the IL-6 interleukin family, called IL-6R complex, that uses common signal transducing subunit (gp130) for their activities. It has also been noted that gp130 has no IL-6 binding capability by itself but plays an important role in the formation of high affinity IL-6 binding sites in association with Il-6/IL-6R complex via transduction of the IL-6 signal (Taga and Kishimoto, 1997). Besides immunoglobin production in B lymphocytes by IL-6, it has some activities on hematopoietic lineages as it shows different activities on (i) proliferation of myeloma andplasmacytoma cells; (ii) expansion of hematopoietic progenitors; (iii) proliferation and differentiation of megakaryocyte progenitors; (iv) inhibition in proliferation of a mouse myeloid leukaemia cell line M1 and (v) proliferation and differentiation of T lymphocytes into cytotoxic T cells (Taga and Kishimoto, 1997).
In addition to the important effect of IL-6 on the immune system, it often displays hormone like characteristics affecting homeostatic processes.
Although IL-6 has a protective role in many infections, the same cytokine promotes the maintenance of arthritis and some other diseases. In one experiment it has been noted that mouse strain with transgenic expression of IL-6 develops various disorders including multiple myeloma, neurological disease when IL-6 is overexpressed in the central nervous system. Pulmonary fibrosis and hypertension were formed when IL-6 is overexpressed in the lungs and plasmacytosis when IL-6 was expressed under control of the enhancer of the gene encoding human immunoglobin chain (Hunter and Jones, 2015). Recently, IL-6 has been used as a target in medical practice for infective and cancerous diseases including COVID-19. It has been noted that there is a role of cytokine, particularly IL-6, in doing hyperinflammatory response in patients of COVID 19. IL-6 has been identified as a lympohokine that induces the maturation of B cells into (Dinarello, 2007) secreting cells and promotes survival and maintenance of long-lived plasma cells. The link between IL-6 and B cell is characterized by increased concentration of IL-6, B cell hyperplasia associated with anaemia, increased concentration of C-reactive protein (CRP), fevers, etc. Thus, IL-6 represents a keystone cytokine in infection, cancer and inflammation in which it causes disease progression or support the maintenance of immunological reactions (Hunter and Jones, 2015).
Prolonged inflammation induces many diseases like cancer, obesity and metabolic disorders that again show large accumulation of cytokines IL-6. The drug Tocilizumab has been found to be effective in inflammatory disorders (Mauer et al., 2015).
Interleukin 1 family
This family contains 11 members such as, IL-1α, IL-1β, IL-1 receptor-antagonist (IL-1Ra), IL-18, IL-33, IL-36α, IL-36β, IL-36γ, IL-36Ra, IL-37, and Il-Hγ2 cytokines (Turner et al., 2014). This family has 11 cytokines and 10 receptors. These cytokines are produced from macrophages and monocytes. Of these members IL-1α is a potent pro-inflammatory cytokine with a stimulatory effect on CD4+ T cells and to promote differentiation of the T helper cells (αTh17) and T helper cell lineages. Biochemical analysis of IL-1 shows two types IL-1α and IL-1β of similar molecular weight which work through the same receptor to produce immunological effect. Their X-ray crystal structures exhibit their protein folds in such a manner that both IL-1α and IL-1β have the ability to use the same receptor IL-1Ra (Fields et al., 2019). As IL-1 family is the potent modulators of inflammation, their activities are regulated in gene transcription, gene expression and during secretion and also at the time of binding with the receptor.
All cytokines of IL-1 family have N-terminal domain of varying length from more than 100 amino acids (IL-33) to just a single amino acids IL-36Ra (Fields et al., 2019). Proteases remove the N-terminal domain to make mature signalling-competent cytokines. These competent cytokines then bind to the cell surface receptors to initiate signalling which is highly conserved in IL-1 family.
The main function of IL-1 family members is to alter the host response to inflammatory condition for infectious agent and others. IL-1α/β and IL-18 are highly inflammatory cytokines and dysregulation of their expressions can lead to severe pathological effects. Their expressions are regulated through both soluble receptors (type 2 IL-1 receptor) and natural antagonist proteins (IL-1Ra and IL-18 binding proteins) as well as alternatively spliced forms of both ligands and receptors (Schmitz et al., 2005).
Mechanism of signalling in IL-1 family
Normally, the signalling action is initiated via binding of cytokine IL-1α with the specific receptor IL-1RI with nM affinity (high affinity). After binding with the primary receptor, a shared co-receptor IL-1RAcP then binds to the composite surface of the cytokine and primary receptor complex to form a ternary complex. The binding affinity of IL-1RAcP is about 100 fold weaker from that of IL-1β/IL-1RI complex. The ectodomains of these receptors are attached to Toll/interleukin-1 receptor (TIR) domains that reside in the cytoplasm (Fields et al., 2019). With the formation of the trimeric complex containing the cytokine, primary receptor and accessory protein, the cytoplasmic TIR domain of the two receptors are brought together to initiate downstream signalling through Myd88-dependent signalling pathway. Myd88 is a protein in human that is encoded by a gene MYD88. This protein acts as an adapter, connecting proteins that receive signals from outside the cell to the proteins that relay signals inside the cell.
Many cytokines such as IL-1 and TNF-α are toxic because of their pro-inflammatory activities. Consequently, many cytokine inhibitors or drugs have been developed. These drugs or chemicals are called cytokine antagonists. They can inhibit action of cytokines by acting directly on receptors or binding to cytokines for preventing their actions. Antagonistic cytokines can regulate the action of cytokines at the receptor level by binding with the primary receptor which will prevent to form trimeric complex as no accessory proteins can bind with the complex. In this way the signalling action of IL-1 is stopped. This can also be achieved by decoy receptors. Decoy receptor is a receptor that is able to recognize and bind cytokines and prevents initiation of signal activation. That means it acts as a signal inhibitor which inhibits signal. IL-IR2 was one of the first identified decoy receptors. It binds IL-1α and IL-1β to inhibit its binding to IL-1R1. Other decoy receptors TNFRSF6 and DcR3 are found in human malignant tissue. They act as a decoy receptor for TNF cytokine members.
One characteristic of IL-1 signalling is that these cytokines show redundancy in action, thereby, they are capable of binding to the similar or genetically alike receptors. For example, the receptor IL-1RI binds IL-1α and IL-1β and IL-1Ra and the inhibitory receptor IL-1RII bind the same three cytokines with different affinities (Fields et al., 2019). The IL-36 is the most promiscuous primary receptor in the IL-1 family that binds three cytokines IL-36α, IL36β and IL-36 γ as well as a single antagonist cytokine or receptor IL-36Ra.
Interleukin 33 (IL-33)
It is one of the important members of the IL-1 family and is a key component of innate and adaptive immune responses in human. The receptor of IL-33 is ST2 which has no ligand and so this receptor is called orphan receptor. IL-33 has a structural homology with cytokines of the IL-1 family such as IL-1α, IL-1β and IL-18. Similar to IL-1β and IL-18, IL-33 may require processing by Caspase 1 for its biological activity. It has also been found that IL-33 like IL-1α shows dual function both as proinflammatory cytokine and as transcriptional repressor. IL-33 is present in the heterochromatin of mitotic chromosomes and exhibits transcriptional repressor properties (Carriere et al., 2007). It induces its biological activity with the interaction of heterodimer containing IL-1 receptor-like 1 (ST1) and accessory protein of IL-1 receptor (Ronan et al., 2011). IL-33 has two forms like transmembrane forms present in Th2 cells and mast cells. Another form is the soluble or secreted form that increases the secretion of Th2 cytokines (IL-4, IL-5 and IL-13) for inducing Th2 immune responses in inflammatory diseases.
As IL-33 is expressed in several tissues and cell types like endothelial cells, epithelial cells and fibroblast-like cells during homeostasis and inflammation, it is responsible for causing many diseases like arthritis, Crohn’s disease, auto-immune diseases, chronic hepatitis, chronic pancreatitis and pulmonary disease including pulmonary inflammation and chronic obstructive pulmonary disease (COPD). It has also been reported that IL-33 is the key player of forming all stages of COVID-19 such as asymptomatic, mild to moderate, severe to critical and chronic fibrotic condition (Zizzo and Philip, 2020). It also functions as an alarm signal (Alarmin) released upon cell injury to alert immune cells expressing the ST2 receptor (IL-1RL1). Viral infections like influenza virus, respiratory syncytial virus, SARS-CoV-2 and others induce the release of IL-33 from primary bronchial epithelial cells that can damage lung epithelium cells (Cayrol and Girard 2018).
Interleukin 17 family (IL-17)
This family contains six structurally related cytokines from IL-17A to IL-17F with receptor of five members IL-17RA to IL-17RE (Figure 1). This cytokine plays an important role in the host immunity against infectious diseases and chronic inflammatory disease. The sequence homology studies have revealed that nearly 50% homology is found between IL-17A and IL-17F cytokines. IL-17B and IL-17D showing less than 40% sequence homology and17% homology, respectively are found between IL-17E and IL-17A (Xiaoping et al., 2011). IL-17 members of the family contain six isoforms and their molecular weights range from 20 to 30 kDa.
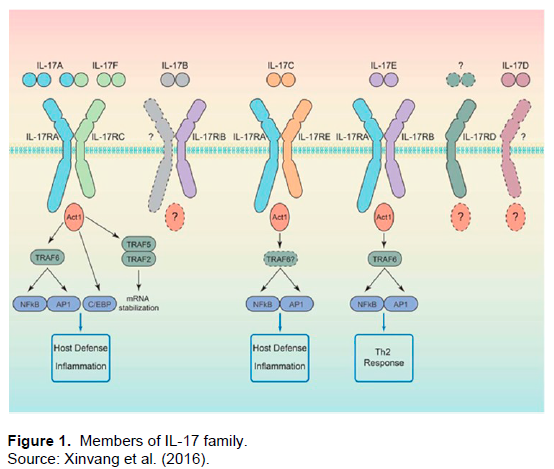
IL-17 cytokine is produced from various cell types like Th17 cells, γδT cells, NKT cells, lymphocyte cells (ILC3s), Tc17 cells, neutrophils and mast cells. Th17 cells are the primary source of IL-17. This cytokine interacts with several mediators like Granulocyte-
Macrophage Colony Stimulating factor (GM-CSF), interferon-gamma (IFNγ) IL- 22, tumour necrosis factor alpha (TNFα) to exert its proinflammatory effect (Yun et al., 2020; Xinvang et al., 2016), leading to the production of inflammatory molecules, chemokines, antimicrobial peptides and remodelling proteins. It has a great impact on host defence, cell trafficking, immune modulation and cell repair processes.
The gene for human IL-17 is cloned from CD4+ T cells and each member of IL-17 family shows distinct pattern of gene expression in different cells. IL-17A and IL-17F show their expressions in a small group of activated T cells and the response of the cell increases during inflammation. IL-17B is expressed in several peripheral and immune tissues and IL-17D is expressed in the nervous system and skeletal muscles. IL-17E is found only in peripheral tissues.
It has been noted that viral defence depends more on Type 1 IFNs rather than IL-17. But there are evidences that IL-17 has some role in viral immune responses which can be beneficial or detrimental to the host. However, IL-17 signalling is counterproductive in certain viral settings, by contributing to the cytokine storm that characterizes disease pathology (Onisha and Gaffen, 2010). Again the members of IL-17 are also important for the clearance of the extra-cellular bacteria Salmonella aureus, Klebsiella pneumonia, Citrobacter rodentium which infect the skin, lung and colon, respectively (Jin and Dong, 2013).
Several immune regulatory functions in infectious and inflammatory diseases are associated with IL-17A and IL-17F. The targets of IL-17A are fibroblasts, epithelial cells and macrophages via the expression of many pro-inflammatory cytokines and chemokines. When IL-17A is overexpressed in epithelial cells of lungs then occurrence of airway inflammation happens. In case of the overexpression of IL-17F in the lungs, increased expressions of proinflammatory cytokine and chemokine are observed with airway inflammation along with the infiltration of neutrophils and macrophages. However, IL-17A and IL-17F have protective responses against infections at mucosal and epithelial layers of intestine, skin, lung and oral cavity through induction of molecules that stimulate epithelial barrier function (Monin and Sarah, 2018). IL-17A and IL-17F induce a proinflammatory condition in the body with increased production of cytokine, chemokine and matrix metalloproteinase (MMP). These processes bring the immune cells to the site of infection to fight with the invading pathogen through accumulation of neutrophils.
In septic patients, fungal infection is increasingly frequent with a high risk of mortality. Sepsis is the result of a severe infection and causes drastic changes in the body to affect the function of different organs like heart, brain and kidneys leading to respiratory or heart failure and death. It has also been noted that IL-17A produces immunoprotective effects in controlling pneumonia caused by fungal pathogens like Aspergillus fumigates, Pneumocystis jirovecii (previous name Pneumocystis carinii), Cryptococcus neoformans and Candida albicans following induction of cytokines and chemokines. But these cytokines also have paradoxical effects on the\ development of systemic fungal infections by increased secretion of proinflammatory cytokines (Thomas, 2021).
Mechanism of signalling of IL-17 family
The mechanism of signalling of this family is not well studied. But it has been noted that IL-17 binds to five receptors IL-17 RA to IL-17RE to mediate signalling system on target cells for their biological activities. All these receptors have a conserved signalling motif SEFIR domain in the intracellular domain and a fibronectin III-like region in the extracellular region. Il-17 cytokines can initiate signal through IL-17 RA/IL-17 RC receptor complex. IL-17B uses specific receptors IL 17RB and IL-17RE. IL-17A and IL-17F use the same IL27RA/IL-17RC receptor (Liji, 2021). IL-17A/IL-17C interacts with IL-17R to stimulate inflammatory reactions through the activation of mitogen activated protein kinase (MAPK), nuclear factor kappa B (NF-?B), CCAAT/enhancer binding protein, januskinase (JAK)/phosphatid-yl inositol 3 kinase (PI3K) and JAK/STAT signalling (Ge et al., 2020). This cytokine can also activate signalling process through TOLL-IL-1 receptor-domain containing adapter inducing interferon-β, myeloid differentiation primary response gene (MyD88) and the adapter proteins. But IL-17 alone cannot produce a robust inflammatory response by itself. It can produce strong inflammatory response synergistically with other inflammatory mediators like tumour necrosis factor (TNF).
Effect of virus on immunity
The immune system is essential to the body. Otherwise the bodies of human and animal will be opened to attack from bacteria, viruses, parasites, etc. So immunity keeps us healthy. The immune system is spread throughout the body. When the immunity is present in the body from birth then this type of immunity is called innate immunity. There is another type of immunity called adaptive (acquired) immunity which has been developed after the entry of pathogens into the body. Once this immunity is developed, the body remembers pathogens or enemies so the immune system works for long time after the entry of same pathogen. Other type of immunity is called passive immunity where the immunity is borrowed from other source. For example, baby receives antibodies from mother but it does not last long.
The initial infection of virus or pathogen on the epithelial cells of the respiratory tract triggers innate immune system which prevents further infection and progress of disease. But some viruses suppress the activation of both innate immune system and the response of interferon and cytokines leading to the hyperactivation of inflammatory macrophages. Then the adaptive immunity becomes active by producing secretory immunoglobulin A (IgA) that guards the mucosal barriers. This has been detected in COVID patients within blood, saliva and nasopharyngeal samples following the blood test of COVID patients. In this condition lymphocyte counts are low but both B and T cells show specific antiviral responses with high number of plasma cells that secrete specific antibodies (IgG and IgA) to attack spike protein of virus of COVID-19. It has also been noted that cytokines mediate inflammation and local immunity.
Another interesting thing has been noted that SARS-CoV-2 infection causes disturbances in the nasopharyngeal microbiome and patients with critical COVID-19 patients show dysbiosis that is causing disbalance between the disturbed microbiome after infection and person’s natural microbiome. That induces a condition of ill health in natural microbiome by decreasing some cytokines that are important in controlling the infection of virus (SARS-CoV-2). Thus bacterial communities or microiobmes in nasopharyngeal area are closely associated with local and systemic inflammatory signalling and antibody responses during COVID-19. The individual differences in the amount of interferon or cytokine secreted by nasal bacteria might be the cause of differential responses by different individuals to SARS-CoV-2 (Liji, 2021). The pathological test of nasal microbiome might be used as new criteria for identification of risk individuals of COVID-19 patients.
After the infection of viruses both innate and adaptive immune responses interact with each other to produce immune protection to the body. There is a time limit for adaptive responses generally 4 to 7 days after infection.
But the innate responses occur immediately after infection of virus. As the innate immunity of the body is weak for clearing the virus, then the adaptive immunity is the key factor for complete elimination of the virus. If the adaptive immunity fails to clear the virus completely then the systemic inflammation occur with the uncontrolled release of inflammatory cytokines leading to the severity of the disease.
CYTOKINE STORM
Although cytokines play an important role in immunity but sometimes they attack its own cells and tissues by producing uncontrolled cytokine then this phenomenon is called cytokine storm. In other words, when the body releases too much cytokine then it is known as cytokine storm.
It is an over-reaction of the immune system in which excess cytokine triggers an onslaught of white blood cells in the infected area of the body resulting inflammation following tissue damage and organ failure. The cytokine storm like condition was noted in 1993 but at that time the term hypercytokinemia or graft versus host disease (GVHD) was used (Ferrara et al., 1993; Roy, 2020; Roy, 2021).Since 2000, the term cytokine storm becomes popular in medical science after the spread of infectious disease COVID 19. In general acute inflammation begins with five key symptoms like rubor or redness, tumor or swelling, calor or heat, dolor or pain and functiolaesa or loss of function (Cuffari, 2021). With the occurrence of inflammation, increased blood flow leads to send plasma proteins and leucocytes on the site of injury or inflammation. The hyperactive immune response through cytokine storm is characterized by the release of interferons, interleukins, tumour necrosis factors, chemokines and several other mediators. During SARS epidemic caused by SARS–CoV-1, the cytokine storm was associated with adverse outcomes (Huang et al., 2005; Sinha, 2020). It has also been noted that interleukin-6 (IL-6), a proinflammatory cytokine, is a key mediator for producing cytokine storm in COVID patients causing severity to fatalities in patients. Cytokine storms are a common complication not only to COVID-19 patients but also to other diseases such as multiple sclerosis and pancreatitis and even in other influenza viruses, SARS, MERS and Bird Flu. The fatality rate is linked with an outcome of uncontrolled cytokine response.
Role of cytokine storm in the fatalities of COVID-19
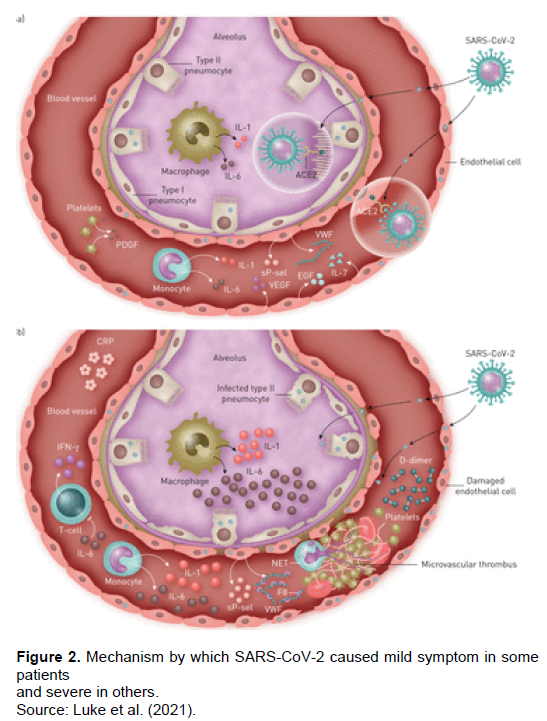
In the severe form of infection of SARS-CoV-2 and life-threatening pneumonia the acute respiratory distress syndrome (ARDS) is observed along with elevation of inflammatory cytokines (Cytokine Storm) leading to the increase of fatality rate in COVID-19. Low pathogenic Coronaviruses infect upper airway and cause seasonal respiratory illness. But highly pathogenic viruses of SARS-CoV-2 with long incubation period of 2 to 14 days, there is a chance of malfunctioning of cytokines leading to hyper-cytokinemia (Luke et al., 2021). The immune system of the body is overactivated when many cytokines like TNFα, IL-1, IL-6, IL-12, IFNα, and IFNβ are produced. Early in the pandemic, high levels of inflammatory cytokines such as interleukins (IL-6) were observed in patients with poor outcomes (Luke et al., 2021). The immune response in case of common influenza having short incubation time is followed by vigorous response of inflammatory cytokines such as interferon (type I/III) which helps to clear the virus.
Compared with other cytokine storm syndromes, such as haemophagocytic lymphohistiocytosis (HLH), which are characterised by an excessive and deleterious immune response led to the idea of a maladaptive immune response driving COVID-19 related morbidity and mortality. Many research findings show that IL-6 levels of more than 80 pg/ml and C-reactive protein are best indicator for diagnostic the condition for respiratory failure and death (Luke et al., 2021). Normally the immune system fights with pathogens to clear them from the body but when it loses control with excess production of cytokines the immune system kills own cells of the body which is called “Suicide Attack” leading to the damage to arteries, veins and capillaries causing leakage of blood and plasma. All these factors make the blood pressure very low to a dangerous level and condition becomes finally similar to septic shock.
Detailed immunological studies by comparing patients with moderate versus severe COVID-19 showed some differences in the expression of inflammatory cytokines. Patients with moderate disease having no ICU requirement have low expression of inflammatory cytokines and some increased tissue growth factors like epidermal growth factor, platelet derived growth factor and vascular endothelial growth factor. In case of patients with severe disease requiring ICU admission had highly elevated pro-inflammatory cytokines (Figure 2) such as IL-1α, IL-1β, Il-6, IL-18 and TNF-α in addition to C- reactive protein (CRP) leading to low innate anti-viral defence state (Luke et al., 2021). It has also been reported that the elevated levels of IL-6 become 1000 times more than normal in case of severe patients where the elevated serum IL-6 content may be 100-1000 pg/ml (Huang et al., 2020).
When SARS-CoV-2 enters the body its body and then the immune system tries hard to fight with the virus by producing multiple immune system cannot recognise new virus as enemy at first. So the virus takes time to multiply rapidly within the cytokines that may cause cytokine storm. Thus it can be said that the direct effect of the virus, immune response and excessive release of inflammatory factors are responsible for producing cytokine storm in the pathogenesis of COVID-19 (Gao et al., 2021).
There is another view to explain the cause of the severity of disease. It is also known that Coronavirus enters directly into the body with the help of its spike protein to the target cells via interaction with cellular receptor angiotensin converting enzyme ACE2. This ACE2 was highly expressed in alveolar epithelial cells, vascular endothelial cells, intestinal epithelial cells, cardiomyocytes and renal proximal tubular cells. It has been demonstrated that the binding of Coronavirus spike protein to ACE2 leads to down regulation of ACE2 resulting in excessive production of vaso-constrictor AngII and reduced production of vasodilator angiotensin 1-7 (Diana et al., 2020). AngII has a role in acting as a proinflammatory cytokine via angiotensin receptor 1 (AT1R). Then AngII-AT1R axis activates NF-?B and metalloprotease 17, facilitating the production of the mature form of epidermal growth factor receptor (EGFR) ligands and TNF-α. The induction of metalloprotease 17 changes the membrane form of IL-6 Rα to the soluble form (sIL-6Rα) followed by the activation of STAT3 via the sIL-6Rα-IL-6 complex leading to a hyper-inflammatory state ( Del Valle et al 2020).
This hyper-inflammatory state is responsible for causing severity and death in COVID-19 disease. The blockade of TNFα may be used to treat many auto-immune inflammatory diseases so the therapeutic method for blocking TNFα or IL-6 may be used to reduce fatalities in COVID-19 patients.
Researchers are trying to identify biomarkers that can predict which patients will deteriorate in uncontrolled inflammatory response (cytokine storm) which can help to take therapeutic measure. To enhance the cytokine assay a new technique of immunoassay, the next generation ELISA test called ELLA test is used to get result within three hours of sample collection making these results actionable (Diana et al., 2020).
Most of the drugs used today are from prior observations of disease produced by SARS and MERS, so the treatment used in case of SARS-CoV-2 is a matter of chance. More and more researches will be needed throughout the world to find out the correct therapeutic agents at a rapid pace to control the elevated levels of inflammatory cytokine in reducing fatalities leading to find out the correct treatment of COVID-19.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Angel A, Vaillant J, Ahmad Q(2020), Interleukins. Published in Stat Pearls Publishing LLC. ( http:/creative commons.org/license/by/4.0) |
|
|
Cuffari B (2021).. What is a Cytokine Storm? News Medical Life Sciences. 5th May. |
|
|
Carriere V, Roussel L, Ortega N, Lacorre DA, Americh L, Aguilar L, Girard JP (2007). IL-33, the IL-1-like cytokine ligand for ST2 receptor, is a chromatin-associated nuclear factor in vivo. Proceedings of the National Academy of Sciences 104(1):282-287. |
|
|
Cayrol C, Girard JP (2018). Interleukin?33 (IL?33): a nuclear cytokine from the IL?1 family. Immunological reviews 281(1):154-168. |
|
|
Del Valle DM, Kim-Schulze S, Huang HH, Beckmann ND, Nirenberg S, Wang B, Gnjatic S (2020). An inflammatory cytokine signature predicts COVID-19 severity and survival. Nature medicine 26(10):1636-1643. |
|
|
Dinarello CA (2007). Historical insights into cytokines. European Journal of Immunology 37(1):34-45. |
|
|
Ferrara JM, Abhyankar S, Gilliland DG (1993). Cytokine storm of graft-versus-host disease: a critical effector role for interleukin-1. Transplantation Proceedings 25(1):1216-1217. |
|
|
Fields JK, Günther S, Sundberg EJ (2019). Structural basis of IL-1 family cytokine signaling. Frontiers in immunology 10:1412 :1-20 |
|
|
Gao YM, Xu G, Wang B, Liu BC (2021). Cytokine storm syndrome in coronavirus disease 2019: A narrative review. Journal of Internal Medicine 289(2):147-161. |
|
|
Ge Y, Huang M, Yao YM (2020). Biology of interleukin-17 and its pathophysiological significance in sepsis. Frontiers in Immunology 11 1558: 1-13. |
|
|
Gulati K, Guhathakurta S, Joshi J, Rai N, Ray AJMI (2016). Cytokines and their role in health and disease: a brief overview. MOJ Immunology 4(2):1-9. |
|
|
Hirano T (2014). Revisiting the 1986 molecular cloning of interleukin 6. Frontiers in Immunology 5(456):1-3. |
|
|
Hirano T, Yasukawa K, Harada H, Taga T, Watanabe Y, Matsuda T, Kishimoto T (1986). Complementary DNA for a novel human interleukin (BSF-2) that induces B lymphocytes to produce immunoglobulin. Nature 324(6092):73-76. |
|
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Cao B (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet 395(10223):497-506. |
|
|
Huang KJ, Su IJ, Theron M, Wu YC, Lai SK, Liu CC, Lei, H. Y. (2005). An interferon?γ?related cytokine storm in SARS patients. Journal of Medical Virology 75(2):185-194. |
|
|
Hunter CA, Jones SA (2015). IL-6 as a keystone cytokine in health and disease. Nature Immunology 16(5):448-457. |
|
|
Jin W, Dong C (2013). IL-17 cytokines in immunity and inflammation. Emerging microbes and infections 2(1):1-5. |
|
|
Liji T (2021). Novel Host-viral -microbiome interactions during COVIS-19 may determine outcome. News Medical Life Sciences. |
|
|
Luke YC, Biggs CM, Jamal S, Stukas S, Wellington CL, Sekhon MS (2021). Soluble interleukin-6 receptor in the COVID-19 cytokine storm syndrome. Cell Reports Medicine 2(5):100269. March (2021). |
|
|
Mauer J, Denson JL, Brüning JC (2015). Versatile functions for IL-6 in metabolism and cancer. Trends in immunology 36(2):92-101. |
|
|
Monin L, Gaffen SL (2018). Interleukin 17 family cytokines: signaling mechanisms, biological activities, and therapeutic implications. Cold Spring Harbor perspectives in biology 10(4):a028522. |
|
|
Onishi RM, Gaffen SL (2010).Interleukin?17 and its target genes: mechanisms of interleukin?17 function in disease. Immunology 129(3):311-321. |
|
|
Sinha P (2020). Is Cytokine storm a relevant to COVID-19? JAMA Internal Medicine 180(9):1152-1154.. |
|
|
Ronan Le Goffic, Arshad MI, Rauch M, L'Helgoualc'h, A, Delmas B, Piquet-Pellorce C,Samson M (2011).Infection with influenza virus induces IL-33 in murine lungs. American Journal of Respiratory cell and molecular biology 45(6):1125-1132. |
|
|
Rose-John S (2018). Interleukin-6 family cytokines. Cold Spring Harbor perspectives in biology 10(2):a028415. |
|
|
Satyesh CR (2020). Corona Virus-Origin, Replication and Remedy for Future Threat. Science and Culture 86(6):137-143. |
|
|
Satyesh CR (2021). Corona Virus and Pandemic. Published in Lambert Academic Publishing . An International Book Service Ltd. Member of Omni Scriptum Publishing Group. Mauritius. |
|
|
Schmitz J, Owyang A, Oldham E, Song Y, Murphy E, McClanahan TK, Kastelein RA (2005). IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity 23(5):479-490. |
|
|
Taga T, Kishimoto T (1997). Gp130 and the interleukin-6 family of cytokines. Annual Review of Immunology 15(1):797-819. |
|
|
Tanaka T, Narazaki M, Ogata A, Kishimoto T (2014).A new era for the treatment of inflammatory autoimmune diseases by interleukin-6 blockade strategy. In Seminars in immunology 26(1):88-96. Academic Press. |
|
|
Turner MD, Nedjai B, Hurst T, Pennington DJ (2014). Cytokines and chemokines: At the crossroads of cell signalling and inflammatory disease. Biochimica et Biophysica Acta (BBA)-Molecular Cell Research 1843(11):2563-2582. |
|
|
Xiaoping Z, Angkasekwinai P, Dong C, Tang H (2011). Structure and function of interleukin-17 family cytokines. Protein and Cell 2(1):26-40. |
|
|
Xinvang S, He X, Li X, Qian Y (2016). The roles and functional mechanisms of interleukin-17 family cytokines in mucosal immunity. Cellular and Molecular Immunology 13(4):418-431. |
|
|
Zizzo G, Cohen PL (2020). Imperfect storm: is interleukin-33 the Achilles heel of COVID-19?. The Lancet Rheumatology. www.thelancet.com/rheumatology Vol 2 December 2020 |
|
|
Zhang JM, An J (2007). Cytokines, inflammation and pain. International anesthesiology clinics 45(2):27. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


