Full Length Research Paper
ABSTRACT
The increasing bacterial resistance to antimicrobial agents has rendered susceptibility testing an indispensable tool for appropriate antibiotic selection. This study is aimed at evaluating the technical methods of antibiogram in some medical laboratories in Cameroon. A descriptive cross-sectional study was carried out. The data collection was done with two material, the questionnaire and the observation sheet. We enrolled 13 laboratories trough a non-probabilistic technic (Quota sampling). Quality control of media and antibiotic discs as well as their conservation did not comply with the standards. Over 76.9% of laboratories did not have the Mac Farland standard range. One hundred percent of the laboratories used the 90 mm diameter petri dishes. Five to fourteen discs were deposit with a mean of 08 discs per Petri dish. The reading of inhibition zones was done by visual estimation in 56.8% of the laboratories. Only 38.5% of the laboratories had reference strains. The interpretation of the susceptibility testing’s crude results were not made by 92.3% of the laboratories. Most laboratories do not have a standard of antimicrobial susceptibility testing. The importance of the strict execution of susceptibility testing procedure should be integrated by the technicians.
Key words: Antimicrobial susceptibility testing, laboratories, standards.
INTRODUCTION
A limited number of methods for antimicrobial susceptibility testing (AST) of medically important microorganisms have survived the maturation of modern diagnostic clinical microbiology (Van Belkum and Dunne, 2013). Antimicrobial susceptibility testing is a technique used to measure the ability of an antibiotic to inhibit bacterial growth in vivo. This technique is universal and should not undergo any changes except updates There are few activities in the clinical microbiology laboratory that utilize more technologist time and laboratory resources than AST. It has been suggested that, at least in terms of direct relevance to the care of patients withinfection, AST may be the single most important activity performed in the clinical microbiology laboratory. AST results are often used to dictate specific management for individual patients, summary AST data is used to drive empiric antimicrobial therapy, and, finally, formulary decisions in some cases are made based on AST results from the laboratory. (Doern, 2011). The interpretative reading of the susceptibility testing has many parameters which must be taken into consideration before prescribing an antibiotic. With the growing increase in bacteria resistance to antimicrobial agents, susceptibility testing has become an indispensable tool in the judicious choice of antibiotics (Genne and Hans, 2003). There is natural resistance and acquired resistance to antibiotics, for example Escherichia coli is naturally resistant to penicillin while ampicillin resistance can be acquired.
Cameroon has many laboratories of different categories. The Bacteriology Unit is found in both public and private laboratories. Nowadays, antimicrobial susceptibility testing is a common practice in these laboratories, but many of them seem not to use standard methods for achieving the susceptibility testing. This study is aimed at assessing the technical methods of antimicrobial susceptibility testing in some medical laboratories in Cameroon and evaluating the gap between these practices and those of the benchmarks.
METHODOLOGY
During a period of six months we carried out a cross-sectional study during which we enrolled Public health institutions and Private laboratories by a non-probabilistic technic. After the identification of the target laboratories, we asked for their consents; then during a period of one week per laboratory, we observed every single steps of the realization of the antimicrobial susceptibility testing. Finally we compared our results to those required by the standard.
Participating laboratories
This cross-sectional survey was carried out at thirteen laboratories. These centers are located in 08 regions of Cameroon, and receive a large number of specimens from patients living in surrounding towns. Public and private medical laboratories which carry out antimicrobial susceptibility testing and agreed to participate were included in the study. Each laboratory was assigned a code for privacy reasons. For quality control purpose, our collection tools were based on the standards currently used. All the procedures used in this study were in reference to the current revision of the Helsinki Declaration.
An authorization to carry out this research was provided by the laboratory Heads. The survey protocol was approved by the Cameroon National Ethics Committee (Reference number: 2014/03/434/L/CNERSH/SP).
Interview data
At enrollment, standardized data collection forms were filled, including identification of each laboratory, the procedure for acquisition, transport and storage of materials, quality controls and the qualifications of the laboratory personnel.
Data collection
After obtaining an authorization from the administration, data were collected through an observation sheet. Information on the techniques used for the antimicrobial susceptibility testing from media preparation to the interpretation of the crude results were also collected and their practices compared to those of the standards.
Quality control
Our collection tools were based on the standards currently used in other countries and those used in the laboratories in Cameroon. The standards mostly found were those of the « Comite de l’Antibiogramme de la Societe Francaise de Microbiologie », CA-SFM (2013) and of the Clinical and Laboratory Standards Institute (CLSI, 2010).
Statistical analysis
Data analysis was done using CSPRO 4.1. Quantitative variables were expressed as mean ± standard deviation, and categorical variables as percentages. Descriptive analysis tools were used including those of the univariate descriptive statistics.
RESULTS
Characteristics of the laboratories
Of the 18 laboratories solicited, 13 agreed to participate, and gave a participation rate of 72.2%. Most of the labo-ratories (76.9%) were public institutions. The repartition of the laboratories according to the qualilification of the laboratory Head showed that 69.2% of the laboratories were headed by clinical biologist and the others by pharmacist biologist, biomedical scientists and laboratory technicians.
Appreciation of the culture media utilization
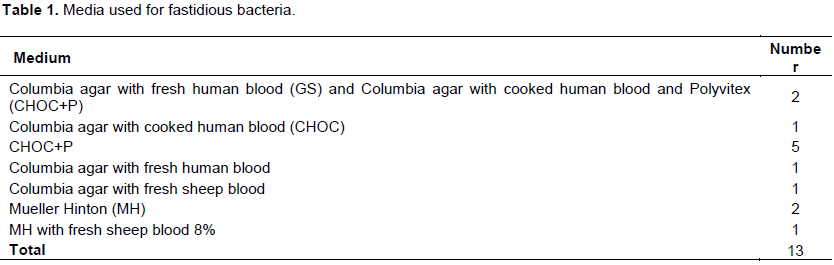
The different media used by the laboratories for the susceptibility testing of fastidious bacteria are shown in Table 1. We found out that 100% of the media used by the laboratories were homemade. They rigorously follow the instructions on the manufacturers’ manual. One of the laboratories did not autoclave media during preparation but heated on a Bunsen burner for 30 min before the spreading on petri dishes. One laboratory also used Columbia agar instead of Mueller Hinton (MH) for susceptibility testing of non-fastidious bacteria. None of the laboratories used MH-F (Mueller Hinton+5% horse blood) agar Table 2.
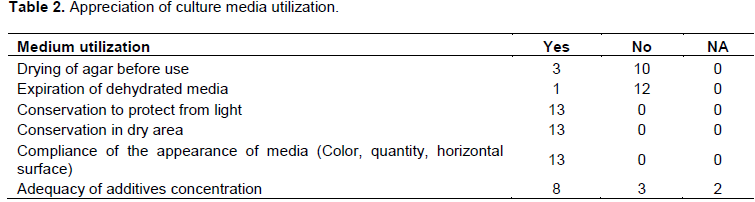
All the laboratories used 90 mm diameter Petri dishes. Only 2 laboratories used square Petri dishes. The media were on average 4.5 mm thick and they were stored in a refrigerator after preparation at an average temperature of 7.8°C. The duration of storage time varied from 02 weeks to 02 months with a mean of 03 weeks. Generally, the preservation of dehydrated MH medium was satisfactory. However, additives such as blood, multivitamin supplement was not always in the prescribed concentrations. The media were not dried before use in 10 laboratories.
We have also evaluated the storage and use of antibiotics discs. The discs were kept at an average temperature of 8.9°C (the ones in use and the stock). Only 2/13 laboratories kept their discs in closed containers with desiccants. In addition, 3/13 laboratories were using expired discs. Three quarters of laboratories (76.9%) did not have a Mc Farland standard. In one case, the Mc Farland was available but not used while in another the Mc Farland was used but not as recommended by the standards. We found only the 0.5 McFarland standard.
Appreciation of the general procedure
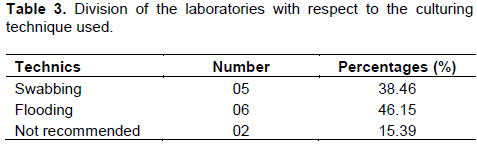
The flooding technique was the most commonly used. The colonies used were pure in most laboratories, however, only one laboratory used the densitometer to standardize their inoculum (Table 3).
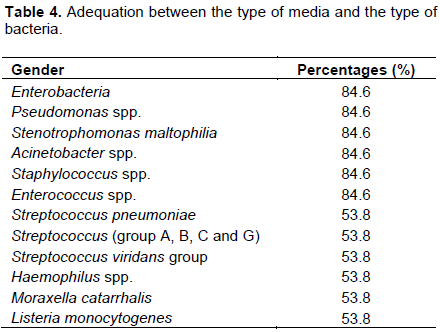
Visual estimation of the diameter of the inhibition zonewas a common practice. The choice of culture media was appropriate in 84.6% of the laboratories, however 76.92% of the laboratories did not use the recommended media for fastidious bacteria (Table 4). The law of 15-15-15 meaning it is necessary to use the bacterial inoculum within 15 min of preparation, placing antibiotic discs 15 min after swabing, and incubating 15 min after the deposition of the discs was not observed in any of the laboratories.
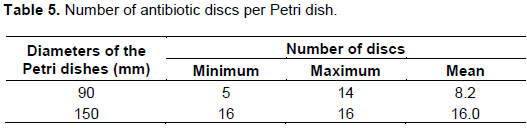
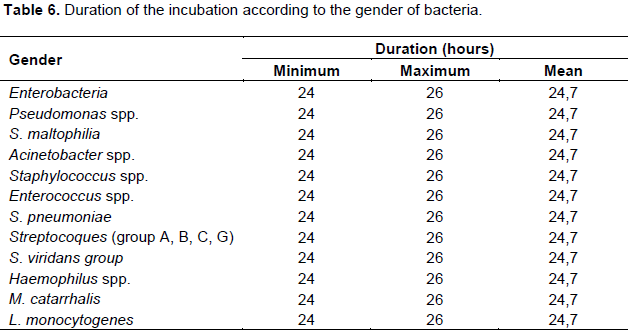
The number of discs placed on the agar varied between 5 and 14, with an average of 08 discs per Petri dish of 90 mm diameter (Table 5). The plates were incubated for 24 h at a temperature of 37 ± 1°C and fastidious bacteria were incubated in a CO2-enriched environment using a lit candle in a jar. The reading of the incubated Petri dishes was visual for 11 laboratories (Table 6).
Interpretation of the results
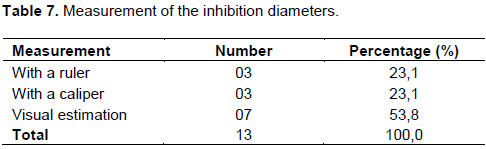
For all the laboratories, the reading of the inhibition zones were made ​​on the back of the agar but not on a black background as recommended by the standards of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) (Table 7). Over 53.8% of laboratories estimated the diameters of the inhibition zones with the naked eye while 46.2% used a ruler and/or calipers. Interpretative reading was not done by 12 of the laboratories. The standard reference most mentioned by the laboratory staff was the “CA-SFM”. Only 30.8% of laboratories used CA-SFM to categorize strains as sensitive (S), resistant (R) or intermediate (I). The other laboratories used the antibiotics manufacturer’s manuel written according to the CLSI standards.
Concerning the results issued, all laboratories mentionned the identified bacteria, the isolates were caterorized sensitive, resistant or intermediate according to their reaction to the different antibiotics tested. However, the method used, the manufacturer of media or discs, and the origin of the critical points were not included on the results.
Quality control of the procedure
The search for resistant phenotypes was not performed by any of the laboratories. Although 92.3% of the laboratories controlled the quality of the media prepared, this quality control was limited to sterility testing. Out of 69.2% of the laboratories did not control the quality of their antibiotic discs. For the other laboratories, the control was generally monthly, trimestrial and even semestrial. In some laboratories, this check was done when a new packet was opened. Only 38.5% of laboratories used reference strains to assess the overall performance of the test and the strains were those of Escherichia coli, Pseudomonas aeruginosa and Staphylococcus aureus. The strains were stored either on nutrient agar at room temperature and away from light or low-temperature in brain-heart infusion (BHI) with glycerol. Finally, only 15.4% of the laboratories were part of an external program of quality assessment in Bacteriology.
DISCUSSION
In 84.61% of the laboratory, the antimicrobial susceptibility testing was not done according to the standards nor were they updated. This is contrary to the review of Patel in 2012 who suggests standard reference methods should be used for identification so that the subject bacteria are consistently and correctly identified to the genus and/or species level. It could be due to either ignorance of the existance of references, or the difficulty to obtain these controls that need to be paid for.
Of the 13 laboratories that agreed to participate, 69.2% were headed by a clinical biologist. This is similar to the work of Nke et al. (2013), who found in their study in Yaounde, that all laboratory Heads were clinical biologists. This shows that our laboratories are headed by qualified specialists.
All the media used for susceptibility testing were homemade, but the type of media was not suitable with the type of bacteria in 11/13 of the laboratories. This is different from a study suggesting that the composition and preparation of the agar and broth media used should be determined, optimised, and documented in a detailed standard operating procedure (Patel, 2012). This shows that their choice was not based on the reference committee on susceptibility testing guidelines.
The storage temperature of the plates was generally respected, while their conservation, the thickness of the agar and the number of discs per petrie dish were not adequate; It is different from a review proposing that growth and incubation conditions (time, temperature, atmosphere e.g. CO2), agar depth, number of concentrations tested per broth and agar dilution should be determined, optimised, and documented in a detailed standard operating procedure (Patel, 2012). This could be explained by the fact that some of these laboratories do not follow the expert rules proposed by the standards..
Only 03 laboratories had a McFarland standard. In one of them the Mc Farland was available but not used and in the other two the use of this standard was not corect. This does not meet the requierements of the review of Patel in 2012 suggesting that the optimum concentration of the inocula must be determined to obtain accurate susceptibility results. This can be explained by the ignorance of the technicians concerning the standards
Eleven laboratories used the flooding technique for economy reasons. Most often, the users of this method did not bother to dry the agar before placing the discs. This was contrary to the “EUCAST” practice, which advises avoiding sub-inoculated agar. We found out that 16.7% of laboratories did not use any of the recommended techniques, but added a colony directly on the agar using a swab.
The temperature and especially the incubation period was not met. References recommended minimum 16 h and maximum 20 to 24 h (EUCAST, 2015, CA-SFM, 2013). Also, these standards recommend a temperature of 35 ± 1°C. This could be due to the fact that this duration was not actually measured but most of the time it is estimated .
Interpretive reading was not done by 12 of the laboratories This was contrary to the work of Leclercq et al. (2013) also Reller et al. (2009) who said the results of a susceptibility test must be interpreted by the laboratory prior to communicating a report to a patient’s physician. This coud be explained by the fact that the biologists are not in charge of only one bench and therefore have too much work.
In regards to the result sheet there were no mention of the method used, type of media or discs, nor the origin of the critical points. Quality control of media prepared was limited to sterility testing. This does not meet the requirements of the WHO and EUCAST that recommend checking the pH, the concentration of divalent cations, thymine and of thymidine, however it is always recommended to do a fertility test and / or specificity. The notion of reference strains is still not well understood in our laboratories; which explains why internal and external quality controls were not done regularly in ten of the laboratories.
CONCLUSION
These results suggest that most laboratories do not have a standard of antimicrobial susceptibility testing, and whenever they have one, they do not strictly comply with the guidelines. Moreover, the importance of the strict and correct execution of susceptibility testing procedure has not been well integrated by the technicians. Interpretative reading of the antibiogram should be learned by the head of laboratories in order to bring out the different phenotypes.
CONflICT OF INTEREST
There is no conflict of interest regarding any of the authors.
REFERENCES
|
CA-SFM. (2013). Comite de l'antibiogramme de la societe francaise de microbiologie. |
|
|
Clinical Laboratory Standard Institute (CLSI) (2010). Performance standards for Antimicrobial Susceptibility testing Sixteenth informational supplement. 2006; 26(25):M100-S16 Wayne, Pennsylvania. USA. |
|
|
Doern GV (2011). Antimicrobial susceptibility testing. J. Clin. Microbiol. 49 (9 Supplement):S4-S4. |
|
|
EUCAST, The European Committee on Antimicrobial Susceptibility Testing (2015). Breakpoint tables for interpretation of MICs and zone diameters. Version 5.0, 2015. |
|
|
Genné D, Hans HS (2003). De l'antibiogramme à la prescription d'un antibiotique. Forum Med Suisse N° 20. |
|
|
Leclercq R, Cantón R, Brown DF, Giske CG, Heisig P, MacGowan AP, Mouton JW, Nordmann P, Rodloff AC, Rossolini GM, Soussy CJ, Steinbakk M, Winstanley TG, Kahlmeter G (2013). EUCAST expert rules in antimicrobial susceptibility testing. Clin. Microbiol. Infect. 19(2):141-60. |
|
|
Nke A (2013). Evaluation des pratiques pré-analytiques dans quelques laboratoires d'analyses médicales de la ville de Yaoundé. Thèse de spécialisation en biologie clinique. |
|
|
Patel RM (2012). The guiding principles on antimicrobial susceptibility testing. Bull. Pharm. Res. 2(3):146-53. |
|
|
Reller LB, Weinstein M, Jorgensen JH, Ferraro MJ (2009). Antimicrobial susceptibility testing: a review of general principles and contemporary practices. Clin. Infect. Dis. 49(11):1749-1755 |
|
|
van Belkum A, Dunne WM (2013). Next-generation antimicrobial susceptibility testing. J. Clin. Microbiol. 51(7):2018-2024. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


