Full Length Research Paper
ABSTRACT
Metabolic syndrome (MetS) has been variously defined because of varying emphasis placed on its components - dyslipidaemia, hypertension (HBP), hyperglyecmia (HG) and abnormal weight. MetS may be associated with diabetes (DM), HBP, chronic kidney disease (CKD) and apparent health (AH). Unfortunately, the frequency of the diagnostic combination of the risk factors in these conditions has not been reported because it could have therapeutic implications. Data generated in earlier studies on 1107 subjects were analyzed. MetS was diagnosed according to the NCEP-ATP 111 criteria. The frequency of the ten possible diagnostic combinations of the risk factor of MetS was counted and analyzed in each condition associated with the syndrome. The triad, truncal obesity (TO), HBP and decreased high density lipoprotein cholesterol (LHDC) recorded the highest frequency in AH subjects, (males 58.8 and females 38.1%) Among the male patients, HBP, HG and decreased LHDC had the highest frequency (DM, 29.9%; HBP 31.8%; CKD 35.5%). The frequency of the diagnostic triads in the female patients differed from that of the males. The combination of TO, HBP and hypertriglyceridaemia (HTG) absent among the male patients gave the highest frequency in female hypertension and CKD patients. The risk factors combination of TO, HBP and LHDLC can be used for screening MetS in the study population especially among the AH subjects. Moreover, TO appears to be the single most significant risk factor for MetS in the population.
Key words: Metabolic syndrome, truncal obesity, diabetes, hypertension, chronic kidney disease, risk factors.
INTRODUCTION
Metabolic syndrome (MetS) is a multiplex risk factor that arises from insulin resistance (IR) accompanying abnormal adipose deposition and function. The MetS has been severally defined by various bodies and authors including World Health Organization, WHO (1999); European Group for the Study of Insulin Resistance (EGIR) (Balkua and Charles 1999); National Cholesterol Education Programme-Adult Treatment Panel III (NCEP-ATP III) (Expert Panel 2001); American Association of Clinical Endocrinologists (AACE) (Einhorn et al., 2003:9); International Diabetes Federation (IDF) (Albert et al., 2005); and American Heart Association/National Heart, Lung, and Blood Institute (Grundy et al., 2005).
The differences in the various definitions lie in the emphasis placed on the components of the cluster which encompass atherogenic dyslipidaemia (HTG) and LHDLC, HBP, HG, a pro-thrombotic and pro-inflammatory state (World Health Organisation, 1999; Pasquale et al., 2008; Albert et al., 2005). The criteria selected by the NCEP-ATP111 to identify individuals with the MetS simplified the definition to require 3 of the following 5 components: abdominal obesity/increased waist circumference; (TO) measured as waist circumference ≥102 cm for men and ≥ 88cm for women; impaired fasting glucose, ≥5.6mmol/l; high fasting triglyceride, ≥1.7 mmol/l; LHDLC≤ 1.0mmol/l for men, ≤ 1.3 mmol/l for women and HBP, ≥ 130/85 mmHg (National Cholesterol Education Programme-Adult Treatment Panel III (NCEP-ATP III) (2001).
MetS is often associated with other metabolic disorders such as DM, HBP (World Health Organisation, 1999), and CKD can occur in AH individuals. Metabolic syn-drome is the end result from years of taking in “a modern day diet”, high in refined carbohydrate such as breads, starches and sweets. As diet differs with countries, it is possible that the combination of the risk factors of the syndrome may differ likewise. Several studies of different ethnic groups suggest different patterns of clustering of the risk factors in MetS, (Sakkinen et al., 2001; Chen et al., 1999; Gray et al., 1998; Meigs et al., 1977). The frequency and combination of the risk factors in these conditions have not been reported. This study analyses a previous study to determine the composition and frequency of the diagnostic criteria as defined by NCEP-ATP 111 in respect of the associated disorders because could have therapeutic implications.
MATERIALS AND METHODS
Data generated in earlier study by Ogbu (2009) were analyzed. The study was a cross-sectional study done between March and August on 1107 subjects including 366 DM (men, 210), 436 HBP (men, 214), 168 CKD patients (men, 86) and 137 (men, 68) AH subjects. The subjects were all aged ≥30 years at the time of study. Subjects on anti-lipid drugs, pregnant or lactating mothers and those below the obtained from Hospital Ethic Committee and written informed consent was obtained in each case before sample collection. Fasting blood samples, (3ml), were collected from subjects between 8 and 11 am each day using standard methods (Dacie and Lewis, 1975) and allowed to clot at room temperature. The samples were spun and sera harvested and used for the determination of triglyceride, (TG), and HDLC by method of Buccolo and David (1973) and Allain et al. (1974), respectively. CromatestR Mono-reagent kits were used for the biochemical determinations.
Analyses of data were done with GraphPad prism version 2 statistical programme. MetS was diagnosed according to the NCEP-ATP 111 criteria (National Cholesterol Education Programme-Adult Treatment Panel III (NCEP-ATP III) (2001).
The risk factors selected by NCEP-ATP 111 are TO/increased waist circumference; (TO) ≥102cm for men; ≥ 88cm for women; HBP ≥135/85 mmHg; HG ≥5.6 mmol/l; LHDLC ≤1.0mmol/l for men and ≤1.3mmol/l for women; HTG ≥1.7 mmol/l. Out of these there can be ten possible combinations for diagnosis of MetS;
(1) [TO. HBP. HG].
(2) [TO. HBP. LHDLC]
(3) [TO HBP. HTG]
(4) [TO. HG. LHDLC]
(5) [TO. HG. HTG]
(6) [TO. LHDLC. HTG]
(7) [HBP. HG. LHDLC]
(8) [HBP. HG HTG]
(9) [HG LHDLC. HTG]
(10) [HG. LHDLC. HTG]
The occurrence of each of these combinations was counted in the test subject groups and their frequency determined.
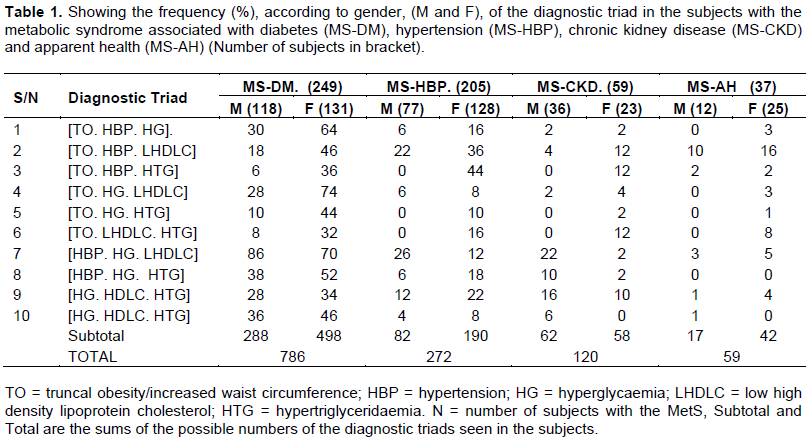
Where a subject had only three of the risk factors the count is one; four risk factors in an individual give four combinations of the triad while the presence of all five risk factors gives ten separate combinations. The reason for using this approach is that all the risk factors could not have appeared at the same time in an individual. At one time the subject may have 3, later 4 and eventual all 5 and in any possible combination. Hence the subtotal and total numbers would differ from the number of subjects with the Met. . Prevalence was calculated as a percentage of the subtotal in a group.
RESULTS
The previous study recorded a prevalence of 51% for outpatients and 27% for AH subjects. MS-DM had the highest prevalence of 68% followed by MS-HBP, MS-CKD and MS-AH; 47%, 35% and 26%, respectively.
Table 1 shows the frequency of the individual triads in subjects with MetS while Table 2 shows the calculated prevalence of each diagnostic triad.
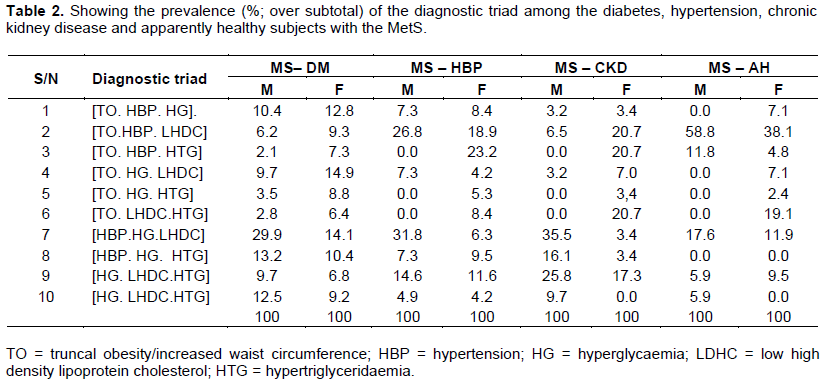
In the present study; the combination of [TO, HBP and LHDLC] recorded the highest prevalence both in male and female MS-AH subjects, (58.8 and 38.1%, respectively) followed by [HBP. HG. LHDLC] combination in the males (17.6%) and [TO. LHDLC. HTG]; (19.1) in the female subjects. Other combinations together recorded a prevalence of <25% among the males and <50% among the female AH subjects thus making TO, HBP, LHDLC and HG the most prevalent among the AH individuals with the MetS.
Among the male DM, HBP and CKD patients, [HBP, HG and LHDLC] has the highest prevalence; 29.9, 31, 8, 35.5%, respectively, followed by [HBP. HG. HTG] (13.2%) in DM, [TO. HBP. HTG] in HBP (26.8%) and [HG. LHDLC. HTG] (25.8%) in CKD. These were the dominant triads in the male patients.
The most frequent abnormalities in these male patients were HBP and HG while the most frequent abnormalities in female patients were the frequency of the diagnostic triads in the female patients differed from that of the males. [TO. HBP. HTG] that recorded zero prevalence among the male patients gave the highest frequency in female hypertension and chronic kidney disease patients. Three combinations of [TO. HBP. HTG], [TO. HBP. HTG] and [TO. LHDLC. HTG] gave same peak prevalence value (20.7%), in chronic kidney disease patients.
The frequency of the triads was more evenly distributed among the female patients than their male counterparts in whom some of the combinations were absent especially among the MS-HBP, MS-CKD and MS-AH groups. The highest frequency recorded by a single triad in the female patients is 23.2% as against 35.5% among the male patients.
DISCUSSION
Starting with the AH subjects, the most prevalent triad in both males and females was TO, HBP and LHDLC. The prevalence of overweight and obesity has increased dramatically both in developed and developing countries of the world in the last 20 years (Hedley et al., 2004). Obesity is a strong and independent risk factor for type 2 diabetes mellitus, coronary heart disease (CHD), stroke, some types of cancer, hypertension, dyslipidaemia, gallbladder disease, sleep apnoea, osteoarthritis (Krauss et al., 1998; Musta et al., 1999), as well as psychosocial consequences, such as a limitation of capacity for physical activity, (Fontaine et al., 1996, WHO, 2000). Weight gain in adults carries with it the risk of coronary heart disease, HBP and type 2 diabetes is proportional to the weight gained (Hedley et al., 2004; Musta et al., 1999). The absence of weight gain particularly among adult of more than 50 years of age does not indicate that fat has not accumulated. Muscle mass is to a varying degree replaced by fat, much of it within the abdomen leading to increasing waist circumference. TO has been reported to be a more a sensitive indicator of IR/MetS than BMI (Fontaine et al., 1996). Moreover, TO is an indicator of visceral body fat mass (World Health Organisation, 2000). IR is a prevalent medical condition that accompanies type 2 diabetes, obesity, hypertension, metabolic syndrome and polycystic ovarian disease (Huang et al., 1998). Visceral fat is of the white type and it is resistant to the anti-lipolytic action of insulin (Willet et al., 1995). Previous study revealed that all AH individuals with excess waist circumference had the MetS (Ogbu, 2009). Analysis also revealed that an average of 74.4% of the triads contain excess waist circumference among the AH subjects. In that case, TO may be a sensitive predictor of the MetS that appear in an individual before the appearance of other risk factors. This suggests that the parameter may be used in screening for the MetS in the test population, especially among AH subjects. The significance of TO diminished among the patients accounting for <50% especially among the male subjects. The lower prevalence of excess WC in the patients may be due to illness but not due to absence of visceral fat accumulation. Traditional biomarkers replaced excess WC in the patients; HG in MS-DM, HBP in MS-BPH and HTG in MS-CKD. However, the significance of LHDLC is obvious especially among the male subjects. The definition of metabolic syndrome includes dyslipidaemia of the HTG, LHDLC type. This combination is the hallmark of the metabolic syndrome and risk factor for ischaemic heart disease (Downs et al., 1998). Fortunately HTG is not common in AH-MetS.
The IR occasioned by excess visceral fat mass gives rise to hyperinsulinaemia which can cause HBP by one or a combination of four mechanisms; (i) sodium ion retention; (ii) sympathetic nervous system over-activity; (iii) disturbed membrane ion transport; (iv) proliferation of vascular smooth muscle cells (Ogbu and Chukwukelu, 2015).
Visceral fat is of the white type and it is resistant to the anti-lipolytic action of insulin (Willet et al., 1995). Lipolysis, therefore, occurs freely in the subject with excess visceral fat releasing TG into the circulation. There is also raised level of hepatic production of triglycerides-rich very low density lipoproteins in MetS as a result of IR. Cholesterol ester transfer protein, (CETP), transfers cholesterol from HDL to VLDL in exchange for TG. Hence serum TG increases while HDLC decreases. This will account for the high prevalence of the triad TO, HBP and decreased HDLPC among the AH subjects.
CONCLUSION
The risk factor combination of TO, HBP, LHDLPC can be used for screening for MetS in the study population especially among the AH subjects.
CONFLICT OF INTERESTS
The authors have not declared any conflicts of interests.
REFERENCES
|
Albert KGMM, Zimmet P, Shaw J(2005)International Diabetic Federation, (IDF), Epidemiology Task Force Consensus Group. The Metabolic Syndrome - a new worldwide definition. Lancet 366(9491):1059-1062. |
|
|
Allain CC, Poon LS, Clau CGS, Richmond W, Fu PD (1974). Enzymatic determination of total cholesterol. Clinical chemistry 20(4):470-475. |
|
|
Balkau B, Charles MA(1999) Comment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistance (EGIR). Diabetes medication 16: 442-443. |
|
|
Buccolo G, David H (1973). Quatitative determination of serum triglycerides by the use of enzymes. Clinical Chemistry 19(4):4760 482. |
|
|
Chen W, Srinivasan SR, Elkasabany A, Berenson GS (1999). Cardiovascular risk factor clustering features of insulin resistance syndrome, (Syndrome X) in a biracial (blck-white) population of children, adolescents and young adults: The Bogahisa Heart Study. American Journal of Epidemiology 150(7):667-674. |
|
|
Dacie JV, Lewis SM (1975). Practical Haematology (1 - 20). 5th Edition ELBS and Churchill Livingstone pp. 609-609. |
|
|
Downs JR, Clerafeld M, Weiss S, Whitney E, Shapiro DR, Beere' PA, Langendorf A, Stein EA, Kruyger W, Gotto AM.Jr (1988). Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels. Journal of American Medical Association 279(20):1615-1622. |
|
|
Einhorn D, Reaven GM, Cobin RH, Ford E, Ganda OP, Handelsman Y, Hellman R, Jellinger PS, Kendall D, Krauss RM, Neufeld ND, Petak SM, Rodbard HW, Seibel JA, Smith DA, Wilson PW (2003) American College of Endocrinology position statement on the insulin resistance syndrome. Endocrine Practice 9(3):237-252. |
|
|
Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults, (2001). Executive Summary of the Third Report of the National Cholesterol Evaluation Programme/ Adult Treatment Panel 111 (NCEP/ATP111). Circulation 106(25):3143-3421 |
|
|
Fontaine KR, Cheskin LJ, Barofsky I (1996). Health-related quality of life in obese persons seeking treatment. Journal of Family Practice 43(1):265-270. |
|
|
Gray RS, Fabsitz RR, Cowan LD, Lee ET, Howard BV, Savage PJ (1998). Risk factor clustering in the insulin resistance syndrome: The Strong Heart Study. American Journal of Epidemiology 148:869 -878. |
|
|
Grundy SM, Cleeman JI, Daurels SR, Donato KA, Eckel RH, Franklin B, Gordon DJ, Krauss RM, Savage PJ, Smith SR, Jr Spertus JA, Costa F (2005 b). Diagnosis and management of the metabolic syndrome; a statement for healthcare professionals: an American Heart Association/National Heart, Lung, and Blood Institute scientific Statement. Circulation 112(21):2735-2752. |
|
|
Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM (2004). Prevalence of overweight and obesity in US children, adolescent and adults, 19992002. Journal of American Medical Association 291(23):2847-2850. |
|
|
Huang Z, Willet WC, Manson JE, Rosner B, Stampfer MJ, Speizer FE, Colditz GA (1998). Body weight, weight change and the risk of hypertension in women. Annals of Internal Medicine 128(1):81-88. |
|
|
Krauss RM, Winston M, Fletcher RN, Grundy SM (1998). Obesity: impact of cardiovascular disease. Circulation 98(15):1472-1476. |
|
|
Meigs JB, D' Agostino RBS, Wilson PW, Gupples LA, Nathan DM, Singer DE (1977). Risk variable clustering in the insulin resistance syndrome: the Framingham Offspring Study. Diabetes 46(10):1594- 1600. |
|
|
Musta A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH (1999). The disease burden associated with overweight and obesity. Journal of American Medical Association 282(16):1523-1529. |
|
|
Ogbu Innocent SI, Chukwukelu Ekene E (2015). Relative Significance of Waist Circumference, Body Mass Index and Waist-Hip Ratio as Predictors of the Metabolic Syndrome in an Apparently Healthy Nigerian Population. Journal of Disease and Global Health 4(1):17-21. |
|
|
Ogbu Innocent SI (2009). Incidence of metabolic syndrome among hospital-based patients in the University of Nigeria Teaching Hospital and apparently healthy people in Enugu metropolis an PhD thesis submitted to the University of Calabar, Nigeria. |
|
|
Pasquale Strazzullo , Antonio Barbato, Alfonso Siani, Francesco P Cappuccio, Marco Versiero, Pierluigi Schiattarella, Ornella Russo, Sonia Avallone, Elisabetta della Valle, Eduardo Farinaro. Diagnostic criteria for metabolic syndrome: a comparative analysis in an unselected sample of adult male population. Metabolism. 2008 Mar; 57(3):355-361. |
|
|
Sakkinen PA, Wahl P, Cushman M, Lewis MR, Tracy RP (2001). Clustering of procoagulation, inflammation and fibrinolysis variables with metabolic factor in insulin resistance syndrome.American Journal of Epidemiology 152(10):897-907. |
|
|
Willet MC, Manson JE, Stampfer MJ, Colditz GA, Rosner B Speizer CH, Hennekens CH (1995). Weight, weight change and coronary heart disease in women: risk within the 'normal' weight range. Journal of American Medical Association 273(6):461-465. |
|
|
World Health Organization (1999). Definition, diagnosis and classification of diabtes mellitus. Geneva, WHO department of Non-Communicable disease Surveillance. |
|
|
World Health Organization (2000). Obesity; preventing and managing the global epidemic. Report of a WHO Consultation. WHO Technical Report Series 894:1-263. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


