ABSTRACT
Acute hepatitis A (AHA) in children usually has generally benign course. In literature, there are several descriptions of gallbladder involvement in AHA, but there are few data on the pediatric population. Fifteen children living in a Romani camp or in the neighbourhoods with AHA were admitted. 57% of children who underwent abdomen ultrasounds showed a significant gallbladder involvement and none of the patients required further diagnostic exams or surgical evaluation. This high frequency of gallbladder involvement is not usually described in pediatric AHA. Furthermore, this is the first Italian AHA outbreak in Romani children population reported in medical literature.
Key words: Gallbladder wall thickening, children, hepatitis A, outbreak, Romani population.
Hepatitis A virus (HAV) is an RNA virus, member of Picornaviridae family, with fecal-oral transmission. In the last decades, the epidemiology of acute hepatitis A (AHA) in Italy has changed due to the improvement of social and hygienic conditions. In fact, by now it is characterized by low endemicity, with an incidence decline from 4/100000 in 1991 to 1.4/100000 in 2006 (Tosti et al., 2008). However, periodical outbreaks in susceptible populations have been described in different epidemiological settings (Pontrelli et al., 2008; Bordi et al., 2012).
There are no official data on hepatitis A seroprevalence or AHA incidence in Romani children population. Only one outbreak in a Greek Romani population has been described (Vantarakis et al., 2010), but considering the epidemiological characteristics, it is possible to predict a high-endemicity epidemiological context, similarly to that in low income countries (Jacobsen and Koopman, 2004). AHA in children usually has no particular clinical features, in comparison with adult form (Matheny and Kingery, 2012). It generally follows a benign course and most episodes heal spontaneously only with dietary and supportive care. A direct involvement of the gallbladder is not frequently described, both in adults and children. However, there are different forms of cholecystic disease reported during AHA in pediatric population. Some authors (Fuoti et al., 2008) have described the occurrence of acalculous cholecystitis while others (Fuoti, 2008) described gallbladder wall thickening (GWT). GWT is defined as a sonographic appearance of a wall thicker than 3 mm (Maudgal et al., 1984) that has been associated with several pathologic conditions and with acute viral hepatitis, especially hepatitis A and B (Kim et al., 2012; Chang et al., 2010; Yamada and Yamada, 2001).
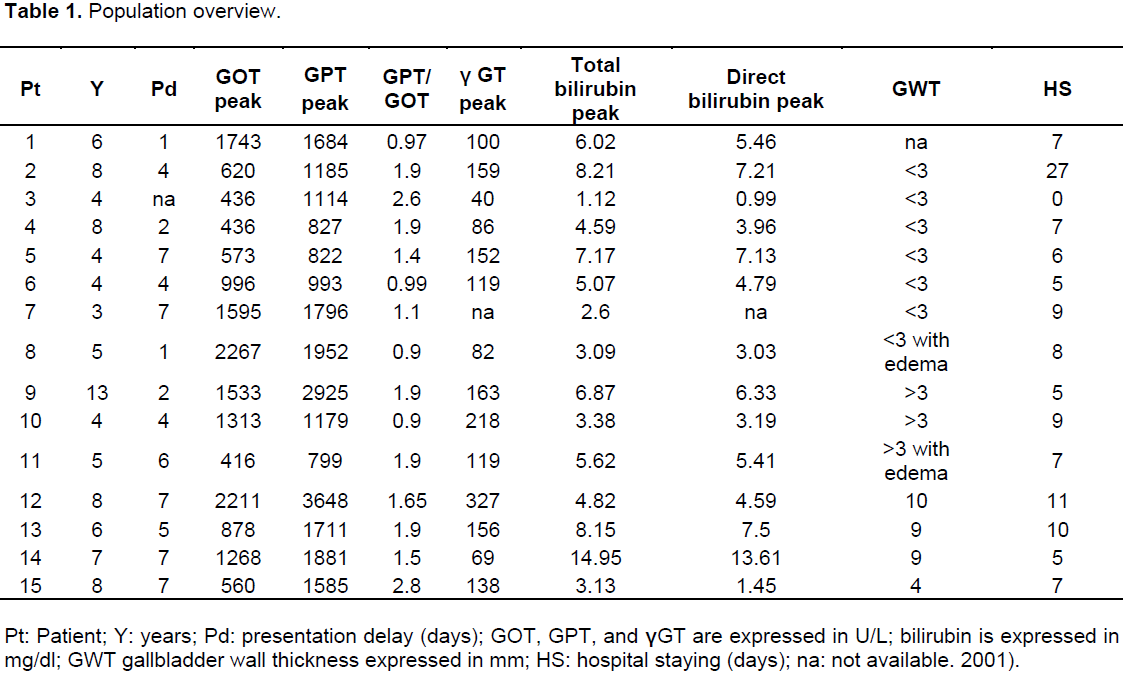
A case series report of 15 children who were diagnosed with AHA from September 2012 to December 2012 at Infectious Pediatric Diseases Department, Policlinico Umberto I Hospital (14 as in patients and one as outpatient) was described (Table 1). GWT was defined as a thickening >3 mm on an abdominal ultrasound (US). The clinical information of patients (pts) obtained through medical record included laboratory findings, predisposing aetiology of GWT, US findings, treatment, and outcomes. The study received approval from the local Ethics Committee, and informed consent was provided by all subjects and it was performed in accordance with the Declaration of Helsinki. The GWT was examined using a real-time sonography system equipped with a 3.5 to 5.0 MHz convex transducer and a 5.0 to 7.5 MHz linear transducer (Mylab 70 XVG Gold, Esaote, Genova, Italy). All patient pts were asked to fast overnight before examination. To measure the GWT, longitudinal or intercostal sonographic scans were used. The maximum thickness was selected. Any other US abnormalities were recorded.
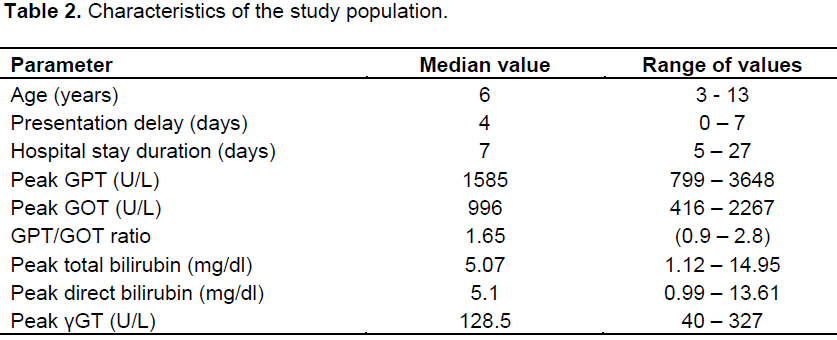
A total of 15 children were included in the study with a median age of 6 years. All the characteristics of patients are listed in Table 1. Ten patients came from a Romani official camp built by Rome council administration, while 4 came from other parts of the city and they were children who have had relationships with infected contacts, so it can be speculated that they got AHA through a person to person contact.
Regarding presentation symptoms, vomiting was reported as first manifestation in 7 pts; hyperchromic urine in 4 cases; abdominal pain, icterus or sub-icterus and fever were described each in 3 cases; diarrhea, asthenia, and anorexia in 2 cases. Finally, 1 patient presented without any symptom or sign and the diagnosis of AHA was based on laboratory examination.
Median presentation delay, namely, the time between the onset of the first symptoms or signs and the access to health care, was 4 days (range 0 to 7 days). After first examination, all children underwent blood tests, with detection of antibodies immunoglobin M (IgM) for HAV, glutamic pyruvate and oxaloacetic transaminase (GPT and GOT), gamma glutamyl transpeptidase (γGT), total and direct bilirubin, glycaemia, urea, serum creatinine, serum electrolytes, total serum proteins, serum albumin, coagulation indexes, and C reactive protein (CRP), for median values (Table 2).
A significant GPT and GOT increase have been recorded with a GPT/GOT mean value greater than one. Blood cell count, CRP, and γGT were within the reference range or only slightly increased, with no correlation with clinical features or prognosis.
Hyperbilirubinemia was recorded in 14/15 pts and in all cases, direct bilirubinemia was largely predominant. In 57% of the cases, a certain degree of gallbladder involvement was observed. Fourteen patients underwent abdomen US and among these, radiologist reported in 8 cases cholecystic abnormal findings, such as a GWT or pericholecystic edema (Table 1). Median hospital stay duration was 7 days (range 5 to 27 days). Please note that a patient, due to social problems, was discharged after 27 days, while 2 pts left against medical advice after 5 and 7 days, respectively (patients 1 and 9) (Table 1).
In the current study, clinical, laboratory, and radiological characteristics of 15 children with AHA, admitted in our pediatric infectious diseases ward were reported. These cases have occurred as a result of an AHA outbreak originating in a Romani camp in the neighbourhood of Rome, and then spreading to adjacent areas. There are few official data focused on sanitary condition and epidemiological characteristics of Romani children, and they should be considered as a special epidemiological subset, critically prone to communicable infectious diseases.
In this study, all children had a good clinical outcome and none had serious clinical complications, in conformity with AHA low mortality rate (2.18/1000) reported in literature (Zuccaro et al., 2012).
Presentation symptoms or signs were the classical one with abdominal pain, asthenia, anorexia, vomiting, hyperchromic urine, icterus or sub-icterus, fever, diarrhea. Mean presentation delay was few days and seemed to be shorter when sub-icterus, icterus or hyperchromic urine presented. This observation is easy to understand since these signs alarmed more parents, although the small number of patients has not been allowed to support these data statistically. It should also be considered that children’s parents were aware of AHA outbreak and so they could easily recognize signs as icterus or issuance of hyperchromic urine. In accordance with other study, a significant GPT and GOT increase was registered with a GPT/GOT mean value greater than one, a well-known evidence in viral acute hepatitis (De Ritis et al., 1957).
Hyperbilirubinemia was recorded in 93% of patients and in all cases direct bilirubinemia was largely predominant. This data differs from classical descriptions of AHA, where a mixed form (direct and indirect bilirubinemia) was reported (Matheny and Kingery, 2012). Moreover, in the 57% of patients, some degree of gallbladder involvement, such as a GWT or pericholecystic edema was observed.
In literature, there are several descriptions of gallbladder involvement in AHA, however, there are few data on pediatric population. Some reports describe rare forms of severe cholecystic involvement during hepatitis A infection (Petrov et al., 2012), with a prolonged course of hyperbilirubinemia; other reports indicate severe surgical complications, acalculous cholecystis (Fuoti et al., 2008) or minor cholecystic diseases associated with AHA, namely, GWT (Foulner, 1999; Maudgal et al., 1984). However, globally, cholecystic involvement is rarely reported in association with pediatric AHA. In our population with AHA, a high number of gallbladder pathological findings was reported. Although none of the children had a clinical evidence of cholecystic involvement, except direct hyperbilirubinemia and consequently none of the patients required further diagnostic exams or surgical evaluation.
Children with gallbladder involvement did not show a different clinical pattern, than other patients, and they did not have a different prognosis.
All patients received a therapy based on bed rest, a dietary regimen for liver disease and intravenous hydration. Two children, who presented with higher total bilirubin values (patients 2 and 14) (Table 1), received a brief course of steroid therapy, with prompt reduction of hyperbilirubinemia (Yoon et al., 2010; Saboo et al., 2012).
Sustained actions are necessary in order to better characterize the epidemiological profile and improve social integration, living conditions, and health-care access of Romani communities. In Italy, HAV vaccination that is highly active (Bonanni et al., 1998), is not routinely suggested, but it could be considered in selected population, such as Romani children, and this could be one of the strategies to reduce the risk of communicable diseases. Our clinical experience suggests that gallbladder involvement could be a common feature in course of AHA in children and it can be easily detected by abdominal US. Moreover, in absence of other signs, the slight gallbladder involvement does not seem to require additional diagnostic or therapeutic measures in pediatric population.
The authors have not declared any conflict of interest.
This work was supported in part by SIMIT Grant 2014.
REFERENCES
|
Bonanni P, Colombai R, Franchi G, Lo Nostro A, Comodo N, Tiscione E (1998). Experience of hepatitis A vaccination during an outbreak in a nursery school of Tuscany, Italy. Epidemiol. Infect. 121(2):377-80.
Crossref
|
|
|
|
Bordi L, Rozera G, Scognamiglio P, Minosse C, Loffredo M, Antinori A, Narciso P, Ippolito G, Girardi E, Capobianchi MR (2012). Monophyletic outbreak of Hepatitis A involving HIV-infected men who have sex with men, Rome, Italy 2008-2009. J. Clin. Virol. 54(1):26-9.
Crossref
|
|
|
|
|
Chang BJ, Kim SH, Park HY, Lim SW, Kim J, Lee KH, Lee KT, Rhee JC, Lim JH, Lee JK (2010). Distinguishing xanthogranulomatous cholecystitis from the wall-thickening type of early-stage gallbladder cancer. Gut. Liver 4(4):518-23.
Crossref
|
|
|
|
|
De Ritis F, Coltorti M, Giusti G (1957). An enzymic test for the diagnosis of viral hepatitis: The transaminase serum activities. Clin. Chim. Acta 369(2):148-52.
Crossref
|
|
|
|
|
Foulner D (1999). Sonographic gallbladder wall thickening in children: Association with acute hepatitis A. Austr. Radiol. 35(4):333-5.
Crossref
|
|
|
|
|
Fuoti M, Pinotti M, Miceli V, Villa MC, Celano MR, Amoruso C, Grumieri G, Carnelli V, Nebbia G (2008). Acute acalculous cholecystitis as a complication of hepatitis A: report of 2 pediatric cases. Pediatr. Med. Chir. 30(2):102-105.
|
|
|
|
|
Jacobsen KH, Koopman JS (2004). Declining hepatitis A seroprevalence: A global review and analysis. Epidemiol. Infect. 132(6):1005-22.
Crossref
|
|
|
|
|
Kim HJ, Park JH, Park DI, Cho YK, Sohn CI, Jeon WK, Kim BI, Choi SH (2012). Clinical usefulness of endoscopic ultrasonography in the differential diagnosis of gallbladder wall thickening. Dig. Dis. Sci. 57:508-515.
Crossref
|
|
|
|
|
Matheny SC, Kingery JE (2012). Hepatitis A. Am. Fam. Phys. 86(11):1027-34.
|
|
|
|
|
Maudgal DP, Wansbrough-Jones MH, Joseph AE (1984). Gallbladder abnormalities in acute infectious hepatitis: A prospective study. Dig. Dis. Sci. 29(3):257-60.
Crossref
|
|
|
|
|
Petrov AI, Vatev NT, Atanasova MV (2012). Cholestatic syndrome in viral hepatitis A. Folia Med. (Plovdiv). 54(1):30-5.
Crossref
|
|
|
|
|
Pontrelli G, Boccia D, DI Renzi M, Massari M, Giugliano F, Celentano LP, Taffon S, Genovese D, DI Pasquale S, Scalise F, Rapicetta M, Croci L, Salmaso S (2008). Epidemiological and virological characterization of a large community-wide outbreak of hepatitis A in southern Italy. Epidemiol. Infect. 136(8):1027-34.
Crossref
|
|
|
|
|
Saboo AR, Vijaykumar R, Save SU, Bavdekar SB (2012). Prolonged cholestasis following hepatitis a virus infection: Revisiting the role of steroids. J. Glob. Infect. Dis. 4(3):185-6.
Crossref
|
|
|
|
|
Tosti ME, Spada E, Romanò L, Zanetti A, Mele A (2008). Acute hepatitis A in Italy: Incidence, risk factors and preventive measures. J. Viral Hepat. 15 Suppl 2:26-32.
Crossref
|
|
|
|
|
Vantarakis A, Nearxou A, Pagonidis D, Melegos F, Seretidis J, Kokkinos P, Zarkadis I, Parasidis T, Alamanos Y (2010). An outbreak of hepatitis A in Roma populations living in three prefectures in Greece. Epidemiol. Infect. 138(7):1025-31.
Crossref
|
|
|
|
|
Yamada K, Yamada H (2001). Gallbladder wall thickening in mononucleosis syndromes. J. Clin. Ultrasound 29(6):322-325.
Crossref
|
|
|
|
|
Yoon EL, Yim HJ, Kim SY, Kim JH, Lee JH, Lee YS, Lee HJ, Jung SW, Lee SW, Choi JH (2010). Clinical courses after administration of oral corticosteroids in patients with severe cholestatic acute hepatitis A: Three cases. Kor. J. Hepatol. 16(3):329-33.
Crossref
|
|
|
|
|
Zuccaro O, Tosti ME, Mele A, Spada E (2012). Epidemiology of acute viral hepatitis in Italy: Results of the surveillance through SEIEVA (Sistema Epidemiologico Integrato dell'Epatite Virale Acuta). Rapporti ISTISAN-Istituto Superiore di Sanità, 24pp.
|
|