Full Length Research Paper
ABSTRACT
Obesity and uncontrolled weight gains is associated with changes in anthropometric variables and hematological parameters. Therefore, this study aims to assess anthropometric variables and hematological parameters among people with obesity. This study was carried out at Central Hospital, Sapele, General Hospital, Oghara and Biomed Diagnostic Centre, Sapele in Southern Nigeria. 415 subjects with age between 18 and 65 years were enrolled for this study including 312 obese experimental subjects (comprising of 111 males and 201 females) and 103 non-obese normal control subjects (comprising 40 males and 63 females). 5.0 ml of venous blood was collected from all subjects into EDTA container and full blood count was determined using Sysmex XN330 automated hematology analyzer. Anthropometric variable of all subjects were measured using standard methods. Monocyte count of obese and non-obese individuals was 6.40±0.23×109/L and 5.14±0.18×109/L when Neutrophil-lymphocyte ratio (NLR) of obese and non-obese people was 1.57±0.21 and 1.18±0.05, respectively. Waist height ratio (WHtR) of obese people was 27.56±0.30 inch/m while WHtR of non-obese/normal people was 17.83±0.22 inch/m. Obese and non-obese people had waist hip ratio of 0.92±0.01 and 0.90±0.01 respectively. Hip circumference (HC) of obese subject was 49.56±0.48 inch and HC of non-obese people was 33.37±0.53 inch. Nevertheless, body mass index (BMI) and mean height of obese people were 36.82±0.55 kg/m2 and 1.66±0.01 m while BMI of non-obese people were 20.43±0.29 kg/m2. Of all hematological parameters, only monocyte and NLR values were higher in people with obesity than in non-obese people and the value of all measured anthropometric variables were higher in obese subject than in non-obese people.
Key words: Anthropometric variables, hematological parameters, Sapele.
INTRODUCTION
Obesity is a medical condition in which excess fat has accumulated in our body to the level that produces adverse effect on health (WHO, 2015). A combination of too much calories intake and sedentary life style are the major causes of obesity, which ultimately results in the formation of excess adipose tissue either in the visceral or in the subcutaneous cavity (Lau et al., 2007). But, small number of obesity is also due to hereditary, medical reasons, decreased variability in ambient temperature and interference with lipid metabolism (Bleich et al., 2008). The main treatment for obesity consists of diet control and physical exercise (Lau et al., 2007; LeFevre and Michael, 2014).
The excessive storage of body fat usually leads to overweight or obesity, which impairs movement, muscular compliance and alter the posture of the body and is regarded as one of the most causes of poor health globally (Dentali et al., 2009).
Obesity is determined with the use of anthropometric variables such as (a) body mass index (BMI) - an accurate reflection of body fat percentage in the majority of the adult population (Mei et al., 2002), (b) waist hip ratio (which assessed body fat distribution and cardiovascular disease risk factor) (Sweeting, 2007; Gray and Fujioka, 1991) (c) waist Circumference (WC) - a major dependent parameter applied for the indirect estimation of increased visceral fat, (d) Weight-Height ratio (WHtR) - a better utility pool in the assessment of central obesity and related cardiovascular risk (Siavash et al., 2008). Nevertheless, obesity is said to occur when the BMI of individual is repeatedly above 30.0 (Haslam and James, 2005).
Ultimately, obesity has emerged as a global health issue and one of the leading preventable causes of mortality globally and uncontrolled weight gains is associated with poor economic productivity, poor health status, reduction in life expectancy (Haslam and James, 2005) as well as changes in anthropometric variables and hematological parameters. Therefore, this study aims to assess the anthropometric variables and hematological parameters among people with obesity in Sapele south-south Nigeria.
Inclusion criteria
People whose BMI were above 30.0 were recruited as subject while people with BMI below 30 were recruited as control group and both groups were within the age ranges of 18 and 65 years and resident in Sapele and its environ.
Exclusion criteria
People whose BMI were below 30.0 and pregnant women, known hypertensive patient, patient with demonstrable ascites, intra-abdominal masses, malignancy, renal disease, liver disease, diabetes mellitus, HIV infection, current oral anticoagulant use, recent surgery (<3 months), and those who refused consent were excluded from this study.
MATERIALS AND METHODS
This is a cross sectional and descriptive study carried out at Central Hospital, Sapele, General Hospital, Oghara and Biomed Diagnostic Centre, Sapele. A total of four hundred and fifteen subjects were enrolled for the study. These include three hundred and twelve obese subjects (comprising of 111 males and 201 females), one hundred and three non-obese subjects (comprising 40 males and 63 females) used as control.
Study area
Sapele is a city located in central part of Delta State, South-South Nigeria. It is positioned at a height of 9 m above sea level at latitude of 5.89° and a longitude of 5.68°. Sapele has a population of about 174,273 (Population census, 2006) and accommodates different tribes such as: Okpe, Urhobo, Itsekiri, Ibo, Ijaw, Isoko, Hausa, Edo, Yoruba, Ibibio, Nupe, Tiv, Fulani. The common diets in this locality are starch, yam, garri, rice, beans, plantain, palm oil, fish, meat, periwinkle the role of the people culture and food choice on obesity prevalence in this locality remains unclear.
Sample collection
Four and half milliliters of venous blood was collected from all participant into EDTA container. The blood sample was analyzed for full blood count within one hour of collection using Sysmex XN330 automated hematology analyzer.
Data analysis
Data analysis was done using Microsoft Excel 2010 and Statistical Package for Social Sciences (IBM SPSS) version 21.0 software. The collated results were expressed as mean and standard deviation and inferential analysis adopted include Student’s t-test. Statistical significance was set at P<0.05.
Ethical approval
Ethical Clearance for this study was obtained from the Ethics committee of Central hospital, Sapele Medical Zone, Sapele, on 8th of December, 2016 with Reference number SNZ/A.31VOL.3/54. Informed consent was also obtained from individuals as well as completed structured questionnaire.
In addition, study was conducted in accordance with the Declaration of Helsinki.
Hematological parameter measurement
The hematological parameters were measured via full blood count with EDTA blood as follows; the EDTA sample was placed in a position where the aperture is immersed in the blood and the aspirator button was pressed.
A suspension of blood cell passes through a small orifice simultaneously with an electric current. After measurement, the result of the cell count and hematological parameters were displayed on the screen and result recorded.
Anthropometric measurement
The anthropometric variables such as: weight (Wt), height (Ht), waist (W), Hip Circumference (HC), body mass index (BMI), waist to hip ratio (WHR), and waist to height ratio (WHtR) of the study subjects were calculated, measured and recorded as shown below:
Height
Height of a subject was measured by asking subject to wear light clothes and put off their shoes, hats or head gear and to stand with back to the tape measure then hold their head in a position where he or she can look straight at a spot, head high, on the opposite wall. A flat rule was placed on the subject’s head, so that the hair, if present was pressed flat. Height was measured to the nearest meter (m) at the level where the flat rule touched the rigid tape.
Weight
Weight was determined using a weighing scale. Weight of a subject was measured by asking him or her to take off heavy outer garments, empty their pockets and step on the weighing scale and reading obtained from the scale reader.
Body mass index (BMI)
Body mass index was calculated at a ratio of an individual’s weight (kg) to height (m2). BMI categories and graded as follows: BMI units of kg/m2, normal weight = 18.5 to < 25, overweight = 25 to < 30 and Obese ≥30.
Waist circumference
Waist circumference was obtained using flexible non stretching tape (Iloh et al., 2012). The subjects were asked to stand straight with arms at the side and feet together. The iliac crest and lower rib cage was first identified by palpation. The waist circumference was taken as the midpoint between the lower border of the lower rib cage and iliac crest in a horizontal plane parallel to the floor as proposed by Iloh et al. (2012).
Waist hip ratio (WHR)
Hip circumference was obtained by the use of a measuring tape to the nearest centimeter. The waist to hip ratio was obtained by dividing waist circumference by hip circumference.
Waist height ratio (WHtR)
Waist height ratio was computed by the formula waist circumference divided by height.
Blood pressure
Blood pressure was obtained using auscultatory method with standard mercury in glass Accuson Sphygmomanometer (Iloh et al., 2013). Prior to the measurement, subject was sited and allowed to rest for 5 min. The left hand muscle was relaxed and the forearm was supported with the cubital fossa at the heart beat level. A cuff of suitable size was applied evenly at the exposed arm. The cuff was inflated until the manometer reading was about 30 mmHg above the level at which the pulse disappeared and then slowly deflated. Then, the Korotkoff sounds were monitored using a Litman Stethoscope placed over the brachial artery. Systolic blood pressure was recorded at the pressure at which the first heart sounds were heard while diastolic blood pressure was taken as the pressure at the point when the heart sounds disappeared. Blood pressure was also measured in the right arm as described for the left arm in order to rule out significant inter arm blood pressure difference and the arm that gave the higher reading was used.
RESULTS
The mean value of Packed Cell Volume (PCV) of obese and non-obese individual were 39.52±3.80% and 39.55±0.55% respectively and hemoglobin (HB) level of people with obesity was 125.39±1.26 g/dl while non-obese people had HB level of 127.27±1.75 g/dl. On the other hand, red blood cell (RBC) count of obese people was 4.55±0.05×1012/L when non-obese individuals had RBC count of 4.65±0.08×1012/l. Furthermore, obese and non-obese persons had total white blood cell (tWBC) count of 6.38±0.54 × 109/L and 5.94±0.28×109/L respectively. Nevertheless, Platelet (PLT) count and Neutrophil (Neut) count of obese people were 247.57±7.67×109/L and 3.01±0.33×109/L while PLT and NEUT count of non-obese individuals were 236.73±11.67×109/L and 3.01±0.26×109/L as shown in Table 1. In addition, lymphocyte (LYMPH) count of people with obesity was 2.59±0.19×109/L when non-obese people had LYMPH count of 2.38±0.10×109/L. The monocyte (MONO) count of obese and non-obese individuals was 6.40±0.23×109/L and 5.14±0.18×109/L respectively. Eosinophil (EOSINO) count and Basophil (BASO) count of people with obesity were 3.44±0.15×109/L and 0.35±0.03×109/L while EOSINO and BASO count of non-obese individuals were 3.81±0.15×109/L and 0.39±0.06×109/L.
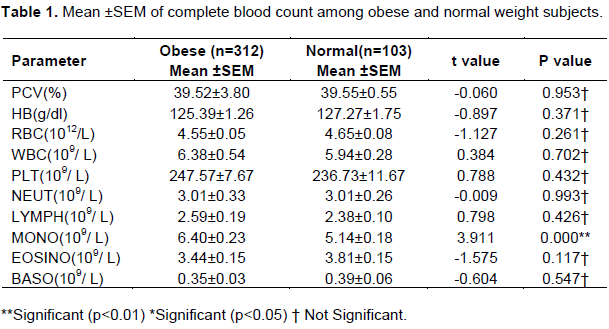
Comparison of hematological parameters shows that value of monocyte was significantly higher in people with obesity than in non-obese people while there was no significant difference in values of PCV, HB, RBC, tWBC, PLT, NEUT, LYMPH, EOSINO, and Basophil count among obese and non-obese people as shown in Table 1.
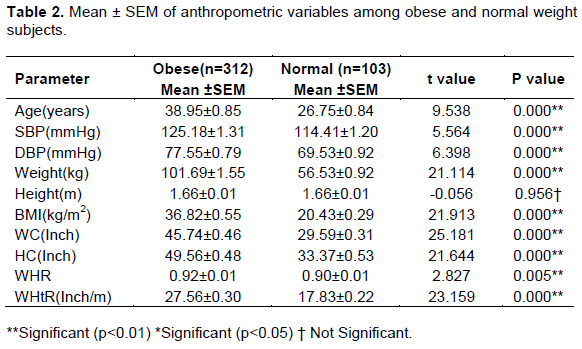
However, Table 2 shows the mean values of anthropometric variables of both obese and non-obese/normal subject and the mean waist height ratio (WHtR) of obese people was 27.56±0.30 inch/m while WHtR of non-obese/normal people was 17.83±0.22 inch/m. On the other hand, obese and non-obese people had Waist Hip Ratio (WHR) of 0.92±0.01 and 0.90±0.01 respectively. Hip circumference (HC) of obese subject was 49.56±0.48 inch and HC of non-obese people was 33.37±0.53 inch. Nevertheless, mean Body Mass Index (BMI) and mean Height of obese people were 36.82±0.55 kg/m2 and 1.66±0.01 m while BMI and height of non-obese people were 20.43±0.29 kg/m2 and 1.66±0.01 m. In addition, mean weight of people with obesity was 101.69±1.55 kg when non-obese people had mean weight of 56.53±0.92 kg. Systolic blood pressure (SBP) of obese and non-obese people was 125.18±1.31 mmHg and 114.41±1.20 mmHg and diastolic blood pressure (DBP) of people with obesity was 77.55±0.79 mmHg while non-obese people had DBP of 69.53±0.92 mmHg as shown in Table 2.
DISCUSSION
There was no significant difference in hematological parameters of obese and non-obese people and no difference in values of hemoglobin, packed cell volume and red blood cell count compared with normal weight subject, this implies that weight gains has no effect on hematopoietic processes and iron metabolism, this result is in agreement with an earlier report that overweight and obese subjects does not have lower hemoglobin and red blood cell count and obesity occur when excess energy intake exceeds energy usage, which does not considerably affect iron metabolism to cause anemia in adult obese subjects (Revelo et al., 2014). Nevertheless, people with obesity had significantly higher monocyte count when compared with non-obese people. This implies that obesity is characterized by chronic low grade systemic inflammatory state that triggers increase expression of monocytosis in obese individuals and there was significant univariate association between monocytosis and obesity, as well as subclinical arteriosclerosis in obese individuals (Kim and Park, 2008). Furthermore, obese subjects had significantly higher Neutrophil-Lymphocytes Ratio (NLR) value when compared with normal non-obese people and this implies that, obesity and excessive weight gain increases NLR due to inflammatory processes that is common in obesity.
Nevertheless, the result of this study shows that obese subjects had significantly higher blood pressure than normal weight subjects; this result is in agreement with the reports of Goh et al. (2014) and Afolabi et al. (2015). The higher blood pressure observed in obese subjects may be attributed to the positive energy balance which eventually leads to adipose tissue hypertrophy to a complex adaptive changes in the adipocytes and overtime these changes altered functionality of cell signaling proteins known as adipokines and increased production of inflammatory markers. Excessive weight gains lead to increased cardiac heart beats and blood output flow, which increases the arterial walls pressure coupled with stiffness of vascular walls due to inflammation eventually cumulate in hypertension overtime (Mathieu et al., 2009; Harwood, 2012).
Anthropometric variables such as: weight (Wt), height (Ht), waist (W), Hip circumference (HC), body mass index (BMI), waist to hip ratio (WHR), and waist to height ratio (WHtR) were higher in people with obesity than in non-obese subject this result in conformity with an earlier report by Sarry et al. (2014) and the higher values anthropometric variable in obese people is due to excessive body fat accumulation which results to negative alterations in body build configuration that characterizes obesity.
CONCLUSION
Of all hematological parameters measured, only monocyte and NLR values were higher in people with obesity than in non-obese people and the value of all measured anthropometric variables were higher in obese subject than in non-obese people.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Afolabi IS, Chinedu SN, Iweala EEJ, Ogunlana OO Azuh DE (2015). Body Mass Index and Blood Pressure in a Semi Urban Community in Ota, Nigeria. Food and Public Health 5(5):157-163. |
|
|
Bleich S, Cutler D, Murray C Adams A (2008). Why is the developed world obese? Annual Review Public Health (Research Support). 29(5):273-295. |
|
|
Dentali F, Squizzato A Ageno W (2009). The metabolic syndrome as a risk factor for venous and arterial thrombosis. Seminars of Thrombosis and Hemostasis 35(5):451-457. |
|
|
Goh LG, Dhaliwah SS, Welborn TA, Lee AH Della PR (2014). Anthropometric measurements of general and central obesity and the predictions of cardiovascular disease risk in women. Cross-section Study 4(2):e004138 |
|
|
Gray DS Fujioka K (1991). Use of relative weight and Body Mass Index for the determination of adiposity. Journal Clinical Epidemiology. 44(6):545-550 |
|
|
Harwood HJ (2012). The adipocyte as an endocrine organ in the regulation of metabolic homeostasis. Neuropharmacology 63(1):57-75. |
|
|
Haslam DW James WP (2005). Obesity. Lancet 13(3):435-436. |
|
|
Iloh GUP, Amadi AN, Njoku PU, Ofoedu JN Awa-Madu J (2012). The magnitude of abdominal adiposity and atherogenic dyslipidaemia among geriatric Nigerians with arterial hypertension in a rural hospital in sout-eastern Nigeria. Nigeria Journal Clinical Practice 15(4):462-468. |
|
|
Iloh GUP, Ikwudinma AO Obiegbu NP (2013). Obesity and its cardio-metabolic morbidities among adult Nigerians in a Primary Care Clinic of a tertiary hospital in South-eastern Nigeria.Journal Family Medicine Primary Care 2(1):20. |
|
|
Kim JA, Park HS (2008). White blood cell count and abdominal fat distribution in female obeseadolescents. Metabolism 57(5):1375-1379. |
|
|
Lau DC, Douketis JD, Morrison KM, Hramiak IM, Sharma AM Ur E (2007). Canadian clinical practice guidelines on the management and prevention of obesity in adults and children summary. Canadan Medical Annual Journal 176(8):S1-S13. |
|
|
LeFevre T Michael L (2014). Behavioral Counseling to Promote a Healthful Diet and Physical Activity for Cardiovascular Disease Prevention in Adults with Cardiovascular Risk Factors: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine 23(16):161-587. |
|
|
Mathieu P, Poirier P, Pibarot P, Lemieux I Despres JP (2009). Visceral obesity: the link among inflammation, hypertension, and cardiovascular disease. Hypertension 53(4):577-584. |
|
|
Mei Z, Grummer-Strawn LM, Pietrobelli A, Goulding A, Goran MI ,Dietz WH (2002). Validity of body mass index compared with other body composition screening indexes for the assessment of body fatness in children and adolescents. America Journal of Clinical Nutrition 75(6):978-985. |
|
|
Revelo XS, Luck H, Winer S Winer DA (2014). Morphological and inflammatory changes in visceral adipose tissue during obesity. Endocrine Pathology 25(1):93-101. |
|
|
Sarry El, Din AM, Zaki ME, Kandeel WA, Mohammed SK Wakeel KH (2014). Cut off values of Anthropometric Indices for the Prediction of Hypertension in a sample of Egyptian Adults. Macedonian Journal Medical Sciences 2(1):89-94. |
|
|
Siavash M, Sadeghi M, Salarifar F, Amini M Shojaee, Moradie F (2008). Comparison of Body Mass Index and waist /height ratio in predicting definite coronary artery disease. Annals Nutrition Metabolism 53(3-4):162-166. |
|
|
Sweeting HN (2007). Measurement and Definitions of Obesity In Childhood and Adolescence: A field guide for the uninitiated. Nutrition Journal 6(1):1-8. |
|
|
World Health Orgganization (WHO) (2015). Obesity: Preventing and Managing the global epidemic. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


