Full Length Research Paper
ABSTRACT
Ambulation is a common goal of stroke rehabilitation that is often linked to lower limb spasticity. This study was conducted to investigate the relationship between paretic lower limb spasticity and functional ambulation after stroke. Thirty stroke survivors (19 males) aged 57.77 ± 9.52 years participated in this correlational cross-sectional study. Spasticity of the paretic lower limb was assessed using the Modified Tardieu Scale. Functional ambulation performance was assessed using the Emory Functional Ambulation Profile (E-FAP). Data were analyzed using Pearson's product moment correlation and stepwise regression analysis at p = 0.05. Spasticity was highest in the ankle plantaflexors (253.20 ± 32.62°). There was a significant relationship between spasticity of the affected lower limb and functional ambulation performance (r=0.61; p<0.05). Stepwise regression analysis indicated that only spasticity of the ankle plantaflexors predicted functional ambulation. Spasticity of the paretic ankle plantaflexors has discriminative power for predicting functional ambulation. This underscores the need for focused rehabilitation aimed at reducing spasticity of ankle plantaflexors for improved functional ambulation among stroke survivors.
Key words: Stroke, spasticity, functional ambulation.
INTRODUCTION
Community ambulation, the ability of a person to walk independently and in the least possible time under various environmental circumstances (Lord et al., 2004), is a predictor of recovery. (Eng and Tang, 2007) and the most desired goals of rehabilitation among stroke survivors (Shim et al., 2012). It is required for successful community reintegration after stroke (Lord and Rochester, 2005). Yet, many stroke survivors who lost the ability to walk, rarely regain independent walking (Robinson et al., 2011; Hendrickson et al., 2014). Limitation in ambulation is associated with increased risks of fall, dependency, restriction in social participation, and poor quality of life (Jørgensen, 1996). Different post-stroke impairments have been shown to contribute to limitations in community ambulation after stroke. Lower extremity spasticity and poor balance are two common impairments that have been linked with difficulties with walking post stroke (Francisco and McGuire, 2012; Patterson et al., 2007).
Spasticity compounds motor impairments among stroke survivors, resulting in secondary complications (Francisco and Mcguire, 2012; Fayazi et al., 2014). Data on prevalence of PSS among stroke survivors in Nigeria are unavailable, reported prevalence from other region ranges between 19 and 47% (Urban et al., 2010; Thibaut et al., 2013; Zorowitz et al., 2013). PSS has significant negative consequences on functional recovery and quality of life (Gillard et al., 2015; Sunnerhagen et al., 2013; Francisco and McGuire, 2012) and is often associated with worse functional outcomes and muscle paresis (Bethoux, 2015). According to Belagaje et al. (2014), stroke survivors without spasticity have significantly better motor activity scores than stroke survivors with spasticity. It has also been posited that spasticity of the knee extensors, allows stroke survivors to support themselves during ambulation (Berger et al., 1984). The role of spasticity in balance control after stroke however, remains controversial (Phadke et al., 2014).
Studies have been conducted to investigate the relationship between community ambulation and different post-stroke impairments. Most of these studies focused on balance and motor impairments (Hamzat et al., 2006; Adegoke et al., 2012; Obembe et al., 2014). Data on the contribution of PSS to community ambulation is still emerging and there is no consensus on the actual relationship between spasticity and community or functional ambulation after stroke. For instance, Lundstrom et al. (2008) and Doan et al. (2012), reported higher disability in stroke survivors with spasticity than those without, while other researchers posited that PSS is a positive sign in the trajectory of stroke recovery (Thibaut et al., 2013; Fayazi et al., 2014; Li, 2017). To effectively manage spasticity for improved community ambulation, it is important to understand the actual relationship between post stroke spasticity and community ambulation. This study was therefore conducted to describe the pattern of PSS and investigate the relationship between paretic lower limb spasticity and community ambulation among stroke survivors in Ibadan, Nigeria.
MATERIALS AND METHODS
Consecutively recruited stroke survivors with first incident stroke resulting in spastic hemiparesis participated in this correlational cross-sectional study. Eligibility criteria were: a grade of 2-4 on the Modified Tardieu Scale and ability to walk a minimum of 10 m with or without walking aid. Participants who were able to comprehend instruction indicating minimal or no evidence of cognitive impairments participated in the study. Stroke survivors with pre-stroke history of difficulty with balance and/or walking and other neuro-musculoskeletal disorders of the lower limb were excluded. Ethical approval was obtained from appropriate institutional health research ethics committee and informed consents were obtained from eligible participants.
Measurements
Lower extremity spasticity was assessed in the participants. Specifically, spasticity of the hip extensors, knee extensors and ankle planterflexors of the paretic lower limb was assessed using the Modified Tardieu Scale (MTS). These muscles were selected because of the observed and reported extensor synergy in the muscle groups. The MTS provides a direct measure of spasticity by assessing the joint angle at the point of increased muscle tone (catch) at a high velocity (<1 s). Participants were positioned supine while the quality of muscle reaction and the angle of muscle reaction were measured. There are three speed definitions in taking the measurement: V1 = as slow as possible; V2 = limb falling under gravity; V3 = moving as fast as possible. Quality of muscle reaction was rated on a 6-point scale from 0 to 5 where 0 represents no resistance throughout the course of passive movement and 5 signifies an immobile joint. Angles of muscle reaction at V3 (R1) and at V1 (R2) were measured using a universal goniometer during hip flexion, knee flexion and ankle dorsiflexion. The dynamic tone component of the muscles was obtained by subtracting R1 from R2 (Boyd and Graham, 1999). The MTS has moderate to very good (K=0.52 – 0.87) test –retest reliability, construct validity (r) of 0.84 and Percentage of Exact Agreement (PEA) with laboratory measurement of spasticity is 100% for elbow flexors and ankle plantaflexors (Mehrhoiz et al., 2005). It also differentiates between spasticity and contracture.
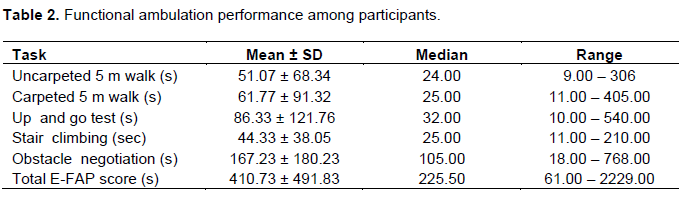
Community ambulation was assessed using the Emory Functional Ambulation Profile (E-FAP). The test includes five timed tasks involving walking under different environmental challenges namely: 5 m-walk on a hard surface, 5 m-walk on a carpeted surface, Up and Go task, negotiating obstacle course and ascending and descending stairs. Participants performed each of the tasks and the time taken to complete each of the task was noted. Each task was scored by multiplying the time taken to complete the task with an appropriate factor. The appropriate factor is based on whether or not the participant used an assistive device and the type of assistive device used. Appropriate factor 1 implies no assistive device was used. Factor 2 means an Ankle-Foot Orthosis (AFO) was used during ambulation performance. Factor 3 describes the use of a walking stick while factor 4 indicates the use of a walking frame. Factors 5 and 6 imply the participant used an AFO with a walking stick and an AFO with a walking frame respectively during task performance. Community ambulation performance was graded as summation of the scores for the five tasks on the E-FAP. High scores denote poor community ambulation performance (Wolf et al., 1999). All tests and measurements were carried out by one of the researchers (OSP) to eliminate bias resulting from measurements. Sociodemographic variables (age, sex and time since stroke onset) were elicited from participants via interview and documented in a form designed for that purpose.
Statistical analyses
Data were cleaned and analyzed using SPSS version 20.0. There were no missing data as measurements were performance-based and graded by one of the researchers (OSP). Pearson product moment correlation was used to test the relationships between community ambulation performance and spasticity. Stepwise regression analysis was conducted using community ambulation (total E-FAP score) as dependent variable while each of hip, knee and ankle spasticity were independent variables. The level of significance was set at 0.05.
RESULTS
Thirty stroke survivors with spastic hemiparesis aged 57.77 ±9.52 years were assessed in this study. Participants were majorly males (n=19; 63.3%). Eighteen (60.0%) of the participants had left hemiparesis.
Mean time since stroke onset was 19.07 ±17.96 months. Nine (30.0%) out of the stroke survivors had no spasticity of the hip extensor whereas knee extensors spasticity was present in almost all the participants (n=29; 96.67%). Spasticity was most severe in the ankle plantaflexors (mean = 253.20 ±132.62°; median = 235.00°) and least severe in the extensors of the hip (mean = 140.17 ±166.82°; median = 60.00°) (Table 1).

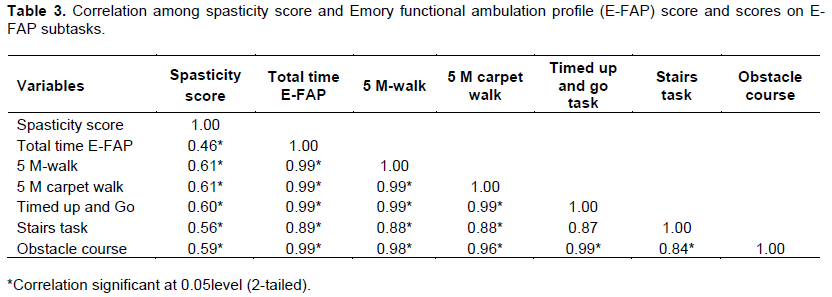
The mean functional ambulation performance score on the E-FAP was 410.73 ±491.83 s (median = 225.50 s). Participants’ scores on each of the five tasks of the Emory Functional Ambulatory Profile (E-FAP) are as presented in Table 2. Spasticity was significantly correlated with community ambulation performance and each of the task (P<0.05) in the E-FAP (Table 3). The predictive value for spasticity was from F≥0.05 to F≤0.10. Only ankle spasticity (β = 0.513; P = 0.004) predicted community ambulation.
DISCUSSION
Participants in this study had mostly spasticity of knee extensors and the majority also had spasticity of ankle plantaflexors. This is similar to an earlier report that extension of the knee with equinovarus foot is the commonest pattern of post-stroke spasticity of the lower limbs (Thibaut et al., 2013). Spasticity, a state of increased muscle tone with accompanying hyper-reflexia, is a common impairment after stroke. Despite the significant contribution of spasticity to motor disability (Urban et al., 2010); it occurrence is considered a positive sign and an important milestone in the trajectory of stroke recovery (Li, 2017).
The Functional ambulation score though higher, is comparable to that reported by Wolf et al. (1999). It is however, considerably higher compared to the values obtained by Adegoke et al. (2012) and Baer and Wolf (2001). The relatively high value obtained in this study may be attributable to the composition of the participants. Participants in the present study had spastic hemiparesis whereas Adegoke et al. (2012) did not indicate whether all their participants had spasticity. This could account for the difference in the functional ambulation score recorded in this study and that of Adegoke et al. (2012).
Co-contraction of agonist and antagonist muscles of the knee may limit normal limb movement which in turn interferes with walking. In addition, participant in this study used assistive devices where necessary whereas earlier studies excluded stroke survivors who ambulated with assistive devices (Adegoke et al., 2012; Fayazi et al., 2014). According to the E-FAP protocol, appropriate factor attached to each assistive device must be used to multiply the time taken to complete the task for which the device was used. This could also have contributed to the findings of this study. Performance on the obstacle negotiating task of the E-FAP was worst as indicated by the time taken by the participants to complete this task. This is in line with the submission that stair climbing and obstacles negotiating subtasks of the E-FAP are more challenging than over-ground walking for stroke survivors (Nadeau et al., 2003).
There was a significant positive correlation between spasticity score and functional ambulation performance. This suggests that higher lower limb spasticity was associated with poor functional ambulation performance. This is particularly so for spasticity of ankle plantaflexors. This is similar to findings from previous studies that a positive, though weak to moderate correlations exists between spasticity and functional ambulation (Belagaje et al., 2014; Welmer et al., 2006, 2010). This could be because spasticity impedes the propulsive force needed for ambulation performance. In addition, spasticity has been associated with muscle paresis among stroke survivors (Bethoux, 2015). Though, muscle strength was not assessed in this study, lower limb muscle strength has been associated with functional mobility (Hsu et al., 2003; Fayazi et al., 2014; Watanabe et al., 2015). Loss of motor units and decreased firing rate may reduce the efficiency of muscle contraction in stroke survivors with spasticity with consequent increased effort, fatigue and difficulty with voluntary force generation (Thibaut et al., 2013). Our finding is contrary to the findings of Fayazi et al. (2014) and Patterson et al. (2007). These authors found no significant correlation between spasticity and mobility. Our finding underscores the need to treat spasticity in stroke survivors for improved ambulatory performance.
LIMITATIONS OF THE STUDY
The findings from this study should however, be interpreted with caution because of the small sample size which makes generalization of results difficult. In addition, the careful selection of only participants with spasticity may also constitute a limitation to this study.
CONCLUSION
The results of this study showed that only spasticity of the ankle has discriminative power for predicting functional ambulation. This highlights the need to manage/treat spasticity especially of the ankle plantaflexors, for improved functional ambulation performance in stroke survivors with spastic hemiparesis.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adegoke BOA, Olaniyi O, Akosile CO (2012). Weight bearing asymmetry and functional ambulation performance in stroke survivors. Global Journal of Health Science 4(2):87-94. |
|
|
Baer HR, Wolf SL (2001). Modified emory functional ambulation profile: an outcome measure for the rehabilitation of post- stroke gait dysfunction. Stroke 32:973-979. |
|
|
Belagaje SR, Lindsell C, Moomaw CJ, Alwell K, Flaherty ML, Woo D (2014). The adverse effects of spasticity on 3- mouth post stroke outcome using a population-based model. Stroke Research and Treatment Volume 2014 Article ID 696089 |
|
|
Berger W, Horstmann G, Dietz V (1984). Tension development and muscle activation in the leg during gait in spastic hemiparesis: Independence of muscle hypertonia and exaggerated stretch reflexes. Journal of Neurology, Neurosurgery and Psychiatry 47(9):1029-1033. |
|
|
Bethoux F (2015). Spasticity management after stroke. Physical Medicine and Rehabilitation Clinics of North America 26(4):625-639. |
|
|
Boyd RN, Graham HK (1999). Objective Measurement of clinical findings in the use of botox type A for the management of children with cerebral palsy. European Journal of Neurology 6(S4):S23-S35. |
|
|
Doan QV, Brashear A, Gillard PJ, Varon SF, Vandenburgh AM, Turkel CC (2012). Relationship between disability and health-related quality of life and caregiver burden in patients with upper limb poststroke spasticity. PM & R 4(1):4-10. |
|
|
Eng JJ, Tang PF (2007). Gait training strategies to optimize walking ability in people with stroke: A synthesis of the evidence. Expert Review of Neurotherapeutics 7(10):1417-1436. |
|
|
Fayazi M, Dehkordi SN, Dadgoo M, Salehi M (2014). The Relationship between Spasticity and Lower Extremity Strength with Functional Mobility Following Chronic Stroke. International Journal of Physical Medicine and Rehabilitation 2(218)2. |
|
|
Francisco GE, McGuire JR (2012). Poststroke spasticity management. Stroke 43(11):3132-3136. https://doi/10.1161/STROKEAHA.111.639831 |
|
|
Gillard PJ, Sucharew H, Kleindorfer D, Belagaje S, Varon S, Alwell K (2015). The negative impact of spasticity on the health-related quality of life of stroke survivors: a longitudinal cohort study. Health and Quality of Life Outcomes 13(1):1-9. |
|
|
Hamzat TK, Olaleye OA, Adeniyi AF, Awolola OE (2006). Standing Asymmetry and Functional Ability in Relation to Gait Parameters in Hemiparetic Stroke Patients. Saudi Journal of Disability and Rehabilitation 12(3 & 4):59-63. |
|
|
Hendrickson J, Patterson KK, Inness EL, McIlroy WE, Mansfield A (2014). Relationship between asymmetry of quiet standing balance control and walking post-stroke. Gait and Posture 39(1):177-181. |
|
|
Hsu AL, Tang PF, Jan MH (2003). Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Archives of Physical Medicine and Rehabilitation 84(8):1185-1193. |
|
|
Jørgensen HS (1996). The Copenhagen Stroke Study experience. Journal of Stroke and Cerebrovascular Diseases 6(1):5-16. |
|
|
Li S (2017). Spasticity, Motor Recovery, and Neural Plasticity after Stroke. Frontiers in Neurology 8:120. |
|
|
Lord SE, McPherson K, McNaughton HK, Rochester L, Weatherall M (2004). Community ambulation after stroke: how important and obtainable is it and what measures appear predictive? Archives of Physical Medicine and Rehabilitation 85(2):234-239. |
|
|
Lord SE, Rochester L (2005). Measurement of community ambulation after stroke: current status and future developments. Stroke 36(7):1457-1461. |
|
|
Lundström E, Terént A, Borg J (2008). Prevalence of disabling spasticity 1 year after first-ever stroke. European Journal of Neurology 15(6):533-539. |
|
|
Mehrhoiz J, Wagner K, Meissner D, Grundmann K, Zange C, Koch R, Pohl M (2005). Reliability of the Modified Tardieu Scale and the Modified Ashworth Scale in adult patients with severe brain injury: A comparison study. Clinical Rehabilitation 19:751-759. |
|
|
Nadeau S, McFadyen BJ, Malouin F (2003). Frontal and sagittal plane analyses of the stair climbing task in healthy adults aged over 40 years: what are the challenges compared to level walking? Clinical Biomechanics (Bristol, Avon) 18(10):950-959. |
|
|
Obembe AO, Olaogun MO, Adedoyin R (2014). Gait and balance performance of stroke survivors in South-Western Nigeria--a cross-sectional study. The Pan African Medical Journal 17(Suppl 1):6. |
|
|
Patterson SL, Forrester LW, Rodgers MM, Ryan AS, Ivey FM, Sorkin JD (2007). Determinants of walking function after stroke: differences by deficit severity. Archives of Physical Medicine and Rehabilitation 88(1):115-119. |
|
|
Phadke CP, Ismail F, Boulias C, Gage W, Mochizuki G (2014). The impact of post-stroke spasticity and botulinum toxin on standing balance: a systematic review. Expert Review of Neurotherapeutics 14(3):319-227. |
|
|
Robinson CA, Shumway-Cook A, Matsuda PN, Ciol MA (2011) Understanding physical factors associated with participation in community ambulation following stroke. Disability and Rehabilitation 33:1033-1042. |
|
|
Shim S, Yu J, Jung J, Kang H, Cho K (2012). Effects of motor dual task training on spatiotemporal gait parameters of post-stroke patients. Journal of Physical Therapy Science 24:845-848. |
|
|
Sunnerhagen KS, Olver J, Francisco GE (2013). Assessing and treating functional impairment in poststroke spasticity. Neurology 80(3S2):S35-S44. |
|
|
Thibaut A, Chatelle C, Ziegler E, Bruno MA, Laureys S, Gosseries O (2013). Spasticity after stroke: Physiology, assessment and treatment. Brain Injury 27(10):1093-1105. |
|
|
Urban PP, Wolf T, Uebele M, Marx JJ, Vogt T, Stoeter P (2010). Occurrence and clinical predictors of spasticity after ischemic stroke. Stroke 41(19):2016-2020. |
|
|
Watanabe M, Suzuki M, Sugimura Y, Kawaguchi T, Watanabe A, Shibata K (2015). The relationship between bilateral knee muscle strength and gait performance after stroke: the predictive value for gait performance. Journal of Physical Therapy Science 27(10):3227-3232. |
|
|
Welmer AK, von Arbin M, Widén Holmqvist L, Sommerfeld DK (2006). Spasticity and its association with functioning and health-related quality of life 18 months after stroke. Cerebrovascular Diseases 21(4):247-253. |
|
|
Welmer AK, Widén Holmqvist L, Sommerfeld DK (2010). Location and severity of spasticity in the first 1-2 weeks and at 3 and 18 months after stroke. European Journal of Neurology 17(5):720-725. |
|
|
Wolf SL, Catlin PA, Gage K, Gurucharri K, Robertson R, Stephen K (1999). Establishing the reliability and validity of measurements of walking time using the Emory Functional Ambulation Profile. Physical Therapy 79(12):1122-1133. |
|
|
Zorowitz RD, Gillard PJ, Brainin M (2013). Poststroke spasticity: sequelae and burden on stroke survivors and caregivers. Neurology 80:S45-S52. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


