Full Length Research Paper

ABSTRACT
Loa loa and Mansonella perstans are two filarial species commonly found in Gabon loiasis has gained attention because of severe adverse events occurring in individuals harboring very high L. loa microfilarial loads after treatment with ivermectin. However, most studies were carried out in rural areas. This work aimed at the study of the prevalence of filarial infections in different urban areas of southeast Gabon. The cross-sectional survey was conducted between May and December 2018 in Franceville, Moanda, and Mvengue. Participants provided written informed consent, a questionnaire to collect data on demographics and related clinical signs (ocular passage of the worm, Calabar swelling, and pruritus). Blood was collected to search for filarial infections. Plasma and blood pellets were separated after centrifugation. The plasma was used for detection of specific IgG4 by ELISA. In total, 545 were samples collected, the overall prevalence of filarial infection in the three cities was 4.77% (95% CI: 3.06–7.97). The prevalence of L. loa infection was 4.59% (95% CI: 3.05–6.79), and 0.18% (95% CI: 0.01–1.18) for M. perstans. The prevalence of ocular passage of the worm, Calabar swelling and pruritus was 27.71% (95% CI: 24.03–31.07), 17.98% (95% CI: 17.90–24.52) and 48.99% (95% CI: 44.72–53.27), respectively. The overall prevalence of specific IgG4 producers was 15.60% (95% CI: 12.71–19.98). There was no correlation between the density of microfilaremia and ocular passage of the worm (p=0.074), but there was a correlation with Calabar swelling (p=0.0005) and between the level of IgG4 subclass and microfilaremic status (p=0.001). This study reveal that the prevalence of L. loa and Mansonella perstans was low in these urban areas, compared with that in rural areas of the same region which was 20.4% for L. loa and 10.2% for M. perstans. These results suggest a different pattern of filarial infection between rural and urban areas.
Keywords: Prevalence, Loa loa, M. perstans, urban area, specific IgG4
INTRODUCTION
Gabon is located in an area in which filariasis is endemic. Loa loa, Onchocerca volvulus, Mansonella perstans, Mansonella streptocerca, and Mansonella rodhaini have endemic foci in Gabon (Zouré et al., 2011). The most prevalent filarial worms in Gabon are L. loa and M. perstans (Akue et al., 2011). Loiasis is endemic in heavily forested areas of Central Africa, including Cameroon, the Democratic Republic of the Congo (DRC), Gabon, and Nigeria (Richardson et al., 2012). In Gabon, the prevalence of L. loa infection is greater than 20% (Zouré et al., 2011). The parasite is transmitted to humans by tabanids belonging to the genus Chrysops: Chrysops dimidiata and Chrysops silacea. Weather transformission has great effect on vectors and vector borne diseases having potential effect (Sumbria and Singla, 2017). They are blood sucking flies mainly found in high trees of rainy forests (Ratmanov and Mediannikov, 2013). Loiasis causes a variety of disease symptoms such as Calabar swelling, the migration of the adult worm under the bulbar conjunctiva, and pruritus. It is estimated that more than 10 million people in Africa have loiasis (Saito et al., 2015). L. loa infection has attracted considerable attention in the context of onchocerciasis control programs (Mischlinger et al., 2018)owing to the serious side effects associated with the use of ivermectin and/or diethylcarbamazine as a mass treatment to eliminate onchocerciasis and lymphatic filariasis in endemic areas (Boussinesq and Gardon, 1997). Because of the co-endemicity, administration of anthelmintic drugs requires great caution especially in patients with loiasis and particularly in individuals with a high load of L. loa microfilaria. It is now accepted that the most effective drugs for L. loa infection are not safe for heavily infected individuals (>30,000 microfilariae per milliliter of blood), and the safer ones are not completely effective (Mogoung-Wafo et al., 2019). A study conducted (Akue et al., 2011)on the epidemiology of concomitant infection due to L. loa and M. perstans in Gabon showed that there is a spatial relationship between the prevalence and intensity of parasitemia in populations living in rural areas. In fact, rural environments in Gabon, are characterized by low levels of urbanization: There are no hospitals but only dispensaries, no road, and houses are surrounded by forest and/ or savannah. The principal activities are field work for women and fishing and hunting for men, food is cooked with fire wood. All these conditions, are favorable for the development of infectious diseases. In 2017, a study carried outin rural department of Tsamba-Magotsi, located in the central part of Gabon, found that the environment is afflicted by the burden of infectious diseases, in particular malaria and neglected tropical diseases (Manego et al., 2017). Microfilaria of L. loa and M. perstans were the most prevalent parasitic infections affecting the local population (Manego et al., 2017). Furthermore, the prevalence of L. loa microfilaremia varies from country to country (Boussinesq and Gardon, 1997)as well as within a country and even within a given geographic area (Boussinesq, 2006). In contrast to L.loa, which seems to be found only in central Africa and in some west African countries, M. perstans is widely spread in many countries and is endemic in a large part of sub-Saharan Africa as well as in South America (Simonsen et al., 2011). However, few studies have been carried out on M. perstans filaria. Although very prevalent, the potential consequences of the infection by this filarial parasite are not well known. Attenuated anemia and a proinflammatory response were shown to be associated with M. perstans infection (Housseini et al. 2012) . Hyper-eosinophilia caused by M. perstans (Fux et al., 2006)and the intraocular localization of M. perstans have also been reported (Bregani et al., 2002). In a study in Uganda the pattern of microfilaremia M. perstans and clinical manifestations were analyzed (Asio et al., 2009). This study suggested that the host's regulatory responses are downregulated in M. perstans infections. Furthermore, most of the reports on both filariae are based on rural populations, with no study performed on the pattern of the filarial transmissions in urban areas. In this era of mass control of parasitic diseases, information on the prevalence and the distribution of filarial parasites is necessary for an appropriate planning strategy. The objective of the present research was to study the prevalence of Loa loa and M. perstans in different cities of the southeast of Gabon.
MATERIALS AND METHODS
Study area
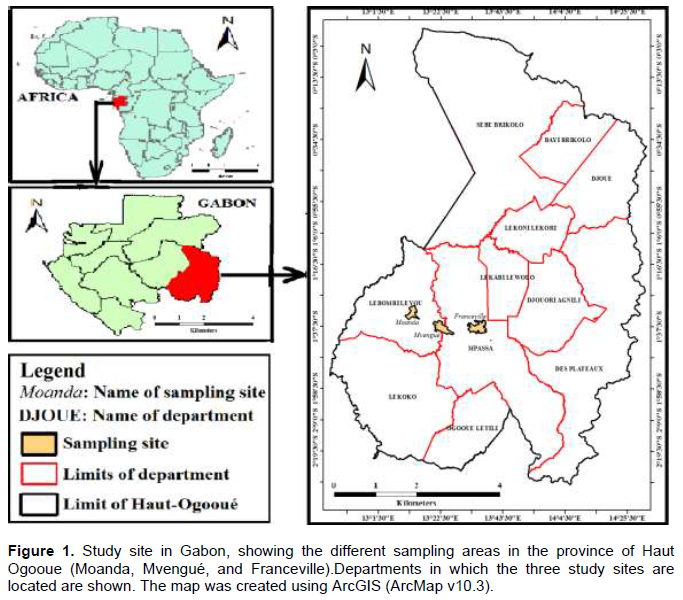
Sampling was carried out in three different urban areas of Haut-Ogooué province: Mvengue, Franceville, and Moanda (Figure 1). Haut-Ogooué is in the southeast of Gabon. The geographic region of the three cities is characterized by isolated areas of savannah and forest.
Study population
The study was conducted from May to July 2018 and October to December 2018 depending on the availability of individual (Holiday, etc.). Blood was collected during day time between 10 a.m. to 2 p.m. A cross-sectional survey was carried out among citizens of Franceville, Moanda, and Mvengue. In order to determine the period prevalence of L. loa and M. perstans, a probability sampling technique using a stratified sampling method was carried out among civil servant from the three cities. The size of the sample was determined according to the formula n=P(100p) Z2/E2.. With P as the percentage of occurrence of the L. loa and M. perstans microfilaria determined during a previous survey in the area (Akue et al., 2011); E is the percentage maximum error required and Z the value corresponding to the level of confidence. Each person who agreed to participate was assigned a code number and was interviewed. All volunteers, including the guardians of all children, provided written, individual informed consent. The National Ethics Committee of Gabon (PROT N00001/20/6/3/SG/CNE) approved the project for this research. The rationale and objective of the study were explained and a one-page questionnaire was administered to all participants. The reliability of the questionnaire was assumed following the procedure developed for the RAPLOA method (Zouré et al., 2011). The question on a history of eye worm was: ‘‘Have you ever experienced or noticed worms moving in your eye or under the eyelid?” The questions on Calabar swellings and pruritus were: ‘‘Have you ever experienced swellings under the skin, or in any other part of your body (hand, chest, face, etc.)”. The questions on pruritus were: “Have you ever experienced itching? Was it over your whole body or only a part? For how long it was?” During the interview, we collected demographic data (age, sex) and the medical history (ocular passage of the worm [eye worm], Calabar swelling, pruritus, etc.).
Blood collection
Field laboratory facilities were set up in healthcare centers in each area of the study site. Intravenous blood was collected in 4 ml tubes containing EDTA (VWR International, France) between 9 a.m. to 2p.m. A 10-µl sample of the collected blood was used for direct parasitological diagnostics. The rest of the blood was centrifuged at 17,000 g for 3 min to separate the plasma and the blood pellet. Each sample was stored at -200C for immunological analysis.
Parasitological analyses
A systematic analysis was initiated by direct examination of a 10-µl sample of blood under an optical microscope, followed by a concentration technique. Parasites were identified and counted directly in 10 µl of blood using a wet mount slide under an optical microscope with a ×10 objective (Gupta and Singla 2012). Parasitemia was expressed in microfilariae per milliliter (mf/ml) of blood. A modified Knott’s concentration technique (Goldsmid, 1970)was applied routinely to each sample, as follows: 1 ml blood was diluted with 9 ml PBS in a conical tube and 200 µl of saponin (2%) was added to lyse red blood cells. The tubes were centrifuged (10 min, 500 g) and the supernatants discarded. The entire pellet was then examined under the microscope (×10 objective) and microfilariae were identified and counted. Parasite species were identified by their size and motility, and by the absence or presence of a sheath.
Extraction of Loa loa antigen
The adult L.loa worm extracted during ocular passage was washed three times in pure water. The worm was homogenized. The homogenization was carried out in solution containing protease inhibitors (2 mM PMSF, 2mMTPCK, 2MmTLCK) and the detergent sodium deoxycholate was added to a final concentration of 1%. The mixture was left on ice for 1 h. The extract was centrifuged at 33,000 g for 30 min and the supernatant was used as antigen. The protein content was measured according to the Bradford method (Bradford, 1976).
Specific IgG4 enzyme linked-immunosorbent assay (ELISA)
A 96-well plate (immunolon II) was coated overnight with 50 ng/ml of adult L. loa extract in 100 μl per well of carbonate buffer pH 9.6 at 4°C. The next day, 200 μl of a saturation solution (TBS-Tween/BSA 3%) was added and incubated for 2 h at room temperature. Plates were washed with washing buffer (TBS-T). Individual sera were collected and added into each well and subsequently incubated at room temperature for 1 h. The plates were then washed again and an anti-IgG4 monoclonal coupled to peroxidase (1/4000) (HP-6025, Sigma) was added to each well and incubated at room temperature for 1 h. The reaction was stopped with stop solution (KPL TMB). The optical densities (OD) were read at wavelength between 450 nm and 620 nm as reference. To differentiate between positive and negative samples for specific IgG4, a cut-off was defined by using the mean of IgG4 in a sample of Turkish (Caucasian) individuals who have never been exposed to L.loa. Therefore, the OD mean level plus one standard deviation of the Caucasian sample was considered as positive for specific IgG4 (OD=0.309). Samples with OD greater than or equal to 0.309 were considered as positive for specific IgG4.
Data analysis
The software Excel was used to create a database, whichwas exported into Epi Info 7 software version 7.1.3.3 (Centers for Disease Control and Prevention, Atlanta, GA) for statistical analysis. Statistical significance was defined as p< 0.05. R-studio version 3.3.2 was used to plot the graphs.
RESULTS
Characteristics of the study population
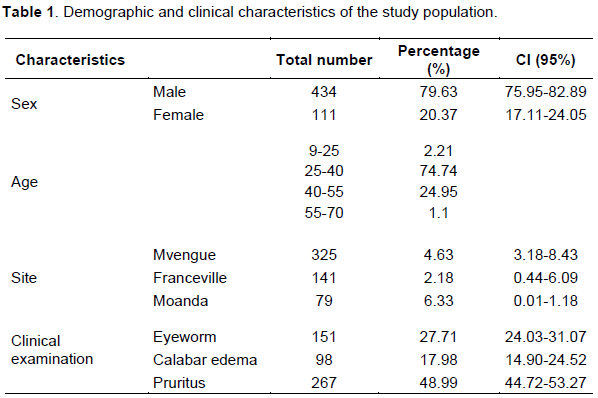
A total of 545 individuals, 10–70 years of age, were enrolled in all the study sites. In our study there were more males (79.63%) than females (20.37%). The average age of our population was 35.76 ±8.38 years. Most of the participants were civil servants (Table 1).
Parasitological analysis
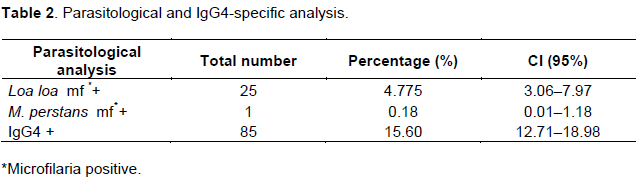
A survey was carried out with all 545 individuals enrolled in the study and their blood was examined for the presence of microfilaria via light microscopic analysis. The general prevalence of microfilaria in the whole population was 4.77%. The prevalence of L. loa was 4.59% and of M. Perstans it was 0.18% (Table 2). When looking at the locations, the prevalence of parasite infection in Mvengue was 4.63%, in Franceville, 2.13%, and in Moanda, 6.33%. For M. perstans, however, only one case of M. perstans microfilaremia was found in Mvengue, 0.31%.
Prevalence of major clinical symptoms of filariae and relationship with parasitological status
Filarial infections are characterized by clinical symptoms such as ocular passage of the worm, edema, and pruritus. The existence of these symptoms among the patients was investigated. The results showed that the prevalence of reported eye worm history was 27.71%. The prevalence of Calabar swelling was 17.98% and that of pruritus was 48.99% (Table 1). When these symptoms were related to microfilaremia, we found that only 48% of microfilaremia carriers reported ocular passage, compared with 52% in this group; this difference was statistically significant (p=0.0217), but there was no relationship between the number of microfilariae and this symptom (p=0.074). Furthermore, 44% of microfilariae carriers reported Calabar swelling compared with 56% without this symptom. The difference between the two groups was statistically significant (p=0.0018), and there was a significant correlation between the density of microfilaria and Calabar swelling (p=0.0005).
Specific IgG4 responses to Loa loa, association with parasitological status, and major clinical symptoms
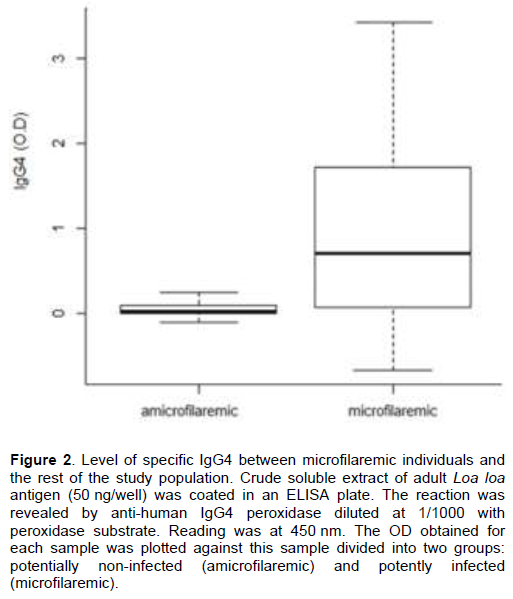
The level of the specific IgG4 subclass in response to the L. loa adult worm antigen was analyzed. The overall prevalence of specific IgG4 producers was 15.60% in our study population. Among microfilariae carriers, 66.67% were specific IgG4 producers and 33.33% were IgG4 non-producers; this difference was not statistically significant (p=1). When comparing the level of specific IgG4 between microfilariae carriers and all other patients enrolled in the study, the difference was more pronounced in the former (1.179±.012 vs.0.2507±37.67). However, this difference between the two groups was not statistically significant (p=0.4624). Besides, there was a correlation between the production of specific IgG4 subclass and microfilaremic status (p=0.001) (Figure 2). Regarding the main clinical symptoms, we found that there was no significant difference or association between ocular passage (36.47% vs. 63.53%, p=0.122) or Calabar swelling (22.35% vs. 77.65%, p=0.471) and the prevalence of specific IgG4 producers.
DISCUSSION
This study was carried out to investigate the prevalence of filarial infection in three different urban areas of the southeast of Gabon. The prevalence of L .loa infection (4.59%) and that of M. perstans (0.18%) is very low compared with the overall prevalence rates of 22.4% reported for L. loa infection in a rural population of Gabon in 2011 and of 10.2% for M. perstans ( Akue et al., 2011). To our acknowledge there is no previous report concerning urban areas in this country. The prevalence of infection in this province was 18.1% for L. loa infection and 13.02% for M. perstans (Akue et al., 2011). The prevalence rate obtained here are very low compared with those obtained in 2011 in the same provinces probably due to differences in the environment. Studies were conducted in two different types of environment. In 2011, the prevalences was determined in a rural population, while in the present study it was determined in urban populations. Our results are also different from those reported in three rural communities of Cameroun where the overall infection rate of L. loa was 27.3% (Mogoung-Wafo et al., 2019). In rural Senegal, the prevalence of M. perstans was 14.5% (Bassene et al., 2015). The difference between our study and the others lie in the type of areas in which the study performed. The low rate of L. loa and M. perstans infections reported in the present study can be explained by the fact that the study was carried out in urban areas, characterized by low forest or savanna, which reduces the presence of L. loa and M. perstans vectors. The urban environment is not favorable to the vector of both L. loa and M. perstans, as these pathogens are vector-borne. In fact, the natural breeding site of Chrysops (the vector of L. loa) is the rainforest canopy (Badia-Rius et al., 2019); Culicoides (the vector of M. perstans) bite early in the morning and in the evening probably at a cooler time (Kelly-Hope et al., 2012). These ecosystems and geoclimatic conditions are not common in urban areas (Badia-Rius et al., 2019). In addition, the access to hospitals in urban areas results in improved health care in the population.Therefore, our results suggest that the prevalence of both parasites may be affected by the environment (Akue et al., 2011). However, this is not seen in all parasitic infections. In a study conducted in 1993 on intestinal parasitic infections in children from urban and rural areas on Pemba Island, all the participants were found to be infected with helminths and there were no significant differences between the urban groups and rural groups (Albonico et al., 1993).
Clinical symptoms have been used to predict the risk of side effects during mass chemotherapy (Gardon et al., 1997). In this study, only microfilaremia, Calabar swelling, and eye worm were taken into consideration since pruritus is a common symptoms of multiple infections in humans and it is often an allergic reaction. Generally, there are two characteristics (calabar swelling and eye worm) and well-known clinical features that are commonly associated with L. loa infection (Antinori et al., 2012). We studied symptoms associated with the infection. The prevalence of eye worm history and Calabar swelling was 27.71 and 17.98%, respectively. These results are not different from those obtained in three rural areas of the center of Cameroun, where the prevalence of Calabar swelling was 22.5% and the prevalence of eye worm was 26.0% (Mogoung-Wafo et al., 2019). The relationship between these symptoms was analyzed and results showed that there was a difference between microfilaremic individuals with ocular passage (48%) and those without ocular passage (52%) (p=0.04642). There was no correlation between the number of microfilariae and eyeworm (p=0.074). However, 44% vs. 56% of microfilariae carriers reported Calabar swelling, and the difference between the two groups was significant (p=0.00382). Furthermore, it was found that the density of microfilariae correlated significantly with Calabar swelling (p=0.0005). This is similar to the results obtained in Gabon (Akue et al., 2011), where the prevalence of eye worm did not correlate with the prevalence of microfilaremia. However, different results were obtained in Cameroun in (Mogoung-Wafo et al., 2019), where a correlation was found between the prevalence of loiasis (evaluated by microfilaremia) and history of eye worm (OR: 5.250; 95% CI: 2.545–10.829; p<0.0001).
Moreover, we found a correlation between the density of L. loa infection and the appearance of Calabar swelling (p=0.0005). Calabar swelling is presumed to reflect hypersensitivity reactions to allergens released by migrating adult worms (Fortunata et al., 2017). In filarial infections, the level of IgG4 can be used as a biomarker of L. loa infection (Akue et al., 1994). The overall prevalence of specific IgG4 producers was 15.60% (95% CI: 12.71–18.98) in our study population. Although this percentage is low compared with the general picture of loiasis infection, which is between 60% and 75%, the ratio remains the same: one third for microfilaremic and two thirds for amicrofilaremic individuals with defined ocular passage (Dupont and Zue-Ndong, 1988). Specific IgG4 levels have been shown to be elevated in both cases, in microfilaria carriers and adult worm carriers without microfilaria (Akue et al., 1994). The fact that in this study some participants without microfilaria had elevated specific IgG4 levels suggests that they had adult worms or an active infection, as was the case for those who were microfilaremic. It was noticed that individuals with microfilariae had high levels of specific IgG4 compared with those without microfilariae, suggesting the specificity of this marker. A total of 33.33% of microfilaremic individuals were not specific IgG4 producers. This might be explained by the fact that some individuals have genetic deficiencies in IgG4 synthesis (Pieringer et al., 2014). No relationship was found between the two characteristic symptoms (eye worm and Calabar swelling) of L. loa infection and IgG4 production (p=0.1223 and p=0.4711, respectively). It is interesting to note that only one case of M. perstans was found among the 545 individuals examined. In addition, only IgG4 against Loa loa were examined. This test has a high specificity of over 95% (Akue et al., 1994). Previous studies on others parasitic infections more often helminths, have shown increased levels of IgG4 during the course of infection (McSorley and Maizels, 2012). This pattern also includes M. perstans despite reduced systemic innate and adaptive immune responses (Ritter et al., 2018). Different clinical expression of filarial infection was tested including adult worm swelling, calabar oedema or pruritus. None of these symptoms were associated with M. perstans. One plausible explanation for this is the number of M. perstans positive cases (n= 1) is that in general, this species is considered asymptomatic although some clinical signs were associated with this parasite in Uganda for example with bunge eye (Asio et al., 2009). Furtheremore, in Gabon a species designated as Mansonella sp”DEUX” was linked to febrile children (Mourembou et al., 2015). Finally, this study was limited by the sampling method which relied on volunteers due to ethical constraints.
CONCLUSION
This study suggests a large difference between the distribution of filariae between urban areas and rural areas within the same geographic region. The implication of this observation should be taken into account for the definition of an appropriate strategic plan to control filarial infection.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
Centre Interdisciplinaire de RechercheMedicales (CIRMF) is sponsored by the State of Gabon and Total Gabon. The authors would like to thank the all participants of this study.
REFERENCES
|
Akue JP, Nkoghe D, Padilla C, Moussavou G, Moukana H, Mbou RA, Ollomo B, Leroy EM (2011). Epidemiology of concomitant infection due to Loa loa and mansonella perstans in Gabon. PLoS Neglected Tropical Diseases 5(10). |
|
|
Albonico M, De Carneri I, Di Matteo L, Ghiglietti R, Toscano P, Uledi MK, Savioli L (1993). Intestinal parasitic infections of urban and rural children on Pemba Island: implications for control. Annals of Tropical Medicine and Parasitology 87(6): 579-583. |
|
|
Antinori S, Schifanella L, Million M, Galimberti L, Ferraris L, Mandia L, Giuseppe T, Cacioppo Monaco V, Tosoni G, Brouqui A, Gismondo P, Giuliani MR, Corbellino G (2012). Imported Loa Loa Filariasis: Three Cases and a Review of Cases Reported in Non-Endemic Countries in the Past 25 Years. International Journal of Infectious Diseases : IJID : Official Publication of the International Society for Infectious Diseases 16 (9):e649-62. |
|
|
Asio SM, Simonsen PE, Onapa AW (2009). Mansonella perstans filariasis in Uganda: patterns of microfilaraemia and clinical manifestations in two endemic communities. Transactions of The Royal Society of Tropical Medicine and Hygiene 103(3):266-273. |
|
|
Badia-Rius X, Betts H, Molyneux DH, Kelly-Hope LA (2019). Environmental factors associated with the distribution of Loa loa vectors Chrysops spp. In Central and West Africa: Seeing the forest for the trees. Parasites and Vectors 12(1):1-11. |
|
|
Bassene, Hubert, Masse Sambou, Florence Fenollar, Siân Clarke, Sawdiatou Djiba, Gaël Mourembou, L. Y. Alioune Badara, Didier Raoult, and Oleg Mediannikov (2015). High Prevalence of Mansonella perstans Filariasis in Rural Senegal. American Journal of Tropical Medicine and Hygiene 93(3):601-6. |
|
|
Boussinesq M (2006). Loiasis. Annals of Tropical Medicine & Parasitology 100(8):715-731. |
|
|
Boussinesq M, Gardon J (1997). Prevalences of Loa loa microfilaraemia throughout the area endemic for the infection. Annals of Tropical Medicine and Parasitology 91(6):573-589. |
|
|
Bradford MM (1976). A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Analytical Biochemistry 72(1):248-254. |
|
|
Bregani ER, Ceraldi T, Rovellini AGC (2002). Case report: intraocular localization of Mansonella perstans in a patient from south Chad. Transactions of the Royal Society of Tropical Medicine and Hygiene 96(6):654. |
|
|
Dupont A, Zue-Ndong JPM (1988). Common occurrence of amicrofilaremic Loa loa filariasis within the endemic region. Transactions of the Royal Society of Tropical Medicine and Hygiene 8(5):730. |
|
|
Fortunata G, Putri S, Jember U, Nurdian Y, Jember U (2017). Calabar Swelling Reflect Hypersensitivity Reactions to Allergens Released by Migrating Adult Loa loa as a Specific Sign for Loiasis(December):5-8. |
|
|
Fux CA, Chappuis B, Holzer B, Aebi C, Bordmann G, Marti H, Hatz C (2006). Mansonella perstans causing symptomatic hypereosinophilia in a missionary family. Travel Medicine and Infectious Disease 4(5):275-280. |
|
|
Gardon J, Gardon-Wendel N, Demanga-Ngangue, Kamgno J, Chippaux JP, Boussinesq M (1997). Serious reactions after mass treatment of onchocerciasis with ivermectin in an area endemic for Loa loa infection. The Lancet 350(9070):18-22. |
|
|
Goldsmid JM (1970). Studies on the laboratory diagnosis of human filariasis: preliminary communication. Journal of Clinical Pathology 23(7):632-635. |
|
|
Gupta SK, Singla LD (2012). Diagnostic trends in parasitic diseases of animals. In: Veterinary Diagnostics: Current Trends. Gupta RP, Garg SR, Nehra V and Lather D (Eds), Satish Serial Publishing House, Delhi pp. 81-112. |
|
|
Housseini D, Yaya IC, Benoit D, Siaka K, Siaka YC, Salif SD, Abdallah AD, Lamine S, Michel EC, Seidina ASD, Aldiouma G, Michael PF, Simon M, Thomas BN, Amy DK (2012). Filariasis attenuates anemia and proinflammatory responses associated with clinical malaria: a matched prospective study in children and young adults. PLoS Neglected Tropical Diseases 6(11):e1890. |
|
|
Kelly-Hope LA, Bockarie MJ, Molyneux DH (2012). Loa loa ecology in central africa: Role of the congo river system. PLoS Neglected Tropical Diseases 6(6):1-4. |
|
|
Manego RZ, Mombo-Ngoma G, Witte M, Held J, Gmeiner M, Gebru T, Tazemda B, Mischlinger J, Groger M, Lell B, Adegnika AA, Agnandji ST, Kremsner PG, Mordmüller B, Ramharter M, Matsiegui PB (2017). Demography, Maternal Health and the Epidemiology of Malaria and Other Major Infectious Diseases in the Rural Department Tsamba-Magotsi, Ngounie Province, in Central African Gabon. BMC Public Health 17 (1):1-7. |
|
|
McSorley HJ, Maizels RM (2012). Helminth infections and host immune regulation. Clinical Microbiology Reviews 25(4):585-608. |
|
|
Mischlinger J, Luzia V, Gildas BT, Paul P, Pierre BM, Markus G, Heimo L, Gebru H, Held T, Jana M, Ramharter B, Michael R (2018). Behavioural and Clinical Predictors for Loiasis. Journal of Global Health 8(1):1-9. |
|
|
Mogoung-Wafo AE, Nana-Djeunga HC, Domche A, Fossuo-Thotchum F, Bopda J, Mbickmen-Tchana S, Djomo-Kamga H, Kamgno J (2019). Prevalence and Intensity of Loa Loa Infection over Twenty-Three Years in Three Communities of the Mbalmayo Health District (Central Cameroon). BMC Infectious Diseases 19(1):1-7. |
|
|
Mourembou G, Fenollar F, Lekana-Douki JB, Ndjoyi Mbiguino A, Maghendji Nzondo S, Matsiegui PB, et Bile B, FadiRaoult D, Mediannikov Oleg (2015). Mansonella, including a Potential New Species, as Common Parasites in Children in Gabon. PLoS Neglected Tropical Diseases 9(10):1-12. |
|
|
Pieringer H, Parzer I, Wöhrer A, Reis P, Oppl B, Zwerina J (2014). IgG4- related disease : an orphan disease with many faces. Orphanet Journal of Rare Diseases 9(110):1-14. |
|
|
Ratmanov P, Mediannikov O (2013). Vectorborne diseases in West Africa : Geographic distribution and geospatial characteristics Vectorborne diseases in West Africa : geographic distribution and geospatial characteristics. Transactions of the Royal Society of Tropical Medicine and Hygiene (June 2014). |
|
|
Richardson ET, Luo R, Fink DL, Nutman TB, Geisse JK, Barry M (2012). Transient facial swellings in a patient with a remote African travel history. Journal of Travel Medicine 19(3):183-185. |
|
|
Ritter M, Ndongmo WPC, Njouendou AJ, Nghochuzie NN, Nchang LC, Tayong DB, Abdel Jelil, Nghochuzie, Nora NN, Lucy CT, Dizzle BA, Kathrin N, NormanJ, Marc W, Samuel L, Laura E, Hoerauf, Achim (2018). Mansonella perstans microfilaremic individuals are characterized by enhanced type 2 helper T and regulatory T and B cell subsets and dampened systemic innate and adaptive immune responses. PLoS Neglected Tropical Diseases 12(1):1-21. |
|
|
Saito M, Armstrong M, Boadi S, Lowe P, Chiodini PL, Doherty T (2015). Clinical features of imported loiasis: A case series from the hospital for tropical diseases, London. American Journal of Tropical Medicine and Hygiene 93(3):607-611. |
|
|
Simonsen PE, Onapa AW, Asio SM (2011). Mansonella perstans filariasis in Africa. Acta Tropica 120(SUPPL. 1). |
|
|
Sumbria D, Singla LD (2017). Thwack of Worldwide Weather Transformation on Vector and Vector-Borne Parasitic Infections. ARC Journal of Animal and Veterinary Sciences 3(2):1-10. |
|
|
Zouré HGM, Wanji S, Noma M, Amazigo UV, Diggle PJ, Tekle AH, Remme JHF (2011). The geographic distribution of Loa loa in Africa: Results of large-scale implementation of the rapid assessment procedure for Loiasis (RAPLOA). PLoS Neglected Tropical Diseases 5(6). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


