Full Length Research Paper

ABSTRACT
Plasmodium falciparum Pfmdr1-86 gene polymorphisms were investigated in blood samples of patients > 6 months of age treated with Amodiaquine-Artesunate (ASAQ) and Artemether-Lumefantrine (AL) in Nanoro, Burkina Faso. Treatments outcome was determined with a 28-day follow-up. The prevalence of Pfmdr-1 N86Y alleles was determined before and after treatment. The PCR-adjusted Adequate Clinical and Parasitological Response (ACPR) was higher in the ASAQ arm (100%) than in the AL arm (87.5%) [Risk difference = -12.50; 95% CI: -20.13; - 4.86 (p=0.001)]. The prevalence of Pfmdr-1 Y86 mutation in the ASAQ arm was significantly higher among patients who had a recurrent parasitaemia (54.54%) than those classified as ACPR (12.70%) (p = 0.007). Similarly, the prevalence of the mutant allele Pfmdr-1 Y86 before treatment (20.00%) was significantly lower than that found in post-treatment (55.56%) in the ASAQ arm (p = 0.01). However, we did not see such difference in the AL arm either for post-treatment samples versus pre-treatment samples (p = 0.88), nor for patients with recurrent parasiteamia compared to those classified as ACPR (p = 0.65). In conclusion, our study showed that ASAQ is selected for parasites carrying the Pfmdr-1 Y86 mutation; however we were not able to demonstrate the reverse relationship between Pfmdr-1 86N and AL treatment as previously reported in Africa.
Key words: Malaria, Plasmodium falciparum, Amodiaquine-Artesunate, Artemether-Lumefantrine, Efficacy, Pfmdr-1, Burkina Faso.
INTRODUCTION
Worldwide use of Artemisinin-based combination therapies (ACT) combined with other control measures (vector control, seasonal malaria chemoprophylaxis, intermittent preventive treatment in pregnant women, etc) has led to significant decreases in malaria transmission and thus subsequent malaria-related morbidity and mortality over the past decade in many endemic countries (Maude et al., 2009; WHO, 2006). Nevertheless, malaria still kills approximately 584,000 people a year worldwide and causes illness in hundreds of millions more, most of them children living in sub-Saharan Africa (World Malaria report 2013).
ACTs, mostly artemether–lumefantrine (AL) and artesunate–amodiaquine (ASAQ), are deployed worldwide, including Burkina Faso where a new treatment policy was adopted in 2005 recommending the use of ASAQ or alternatively AL for the treatment of uncomplicated falciparum malaria (Gansané et al., 2009; Zwang et al., 2009). However, following the reports on the decreasing susceptibility of P. falciparum to artemisinin derivatives along the Thailand and Myanmar border (Dondorp et al., 2009; Lim et al., 2009; Noedl et al., 2010; Rogers et al., 2009), several studies have reported a decline of adequate parasitological response rate to treatment with ACTs in African patients, possibly due to the emergence of parasites with reduced drug sensitivity (Beshir et al., 2013; Borrmann et al., 2011). In such context, the regular monitoring of P. falciparum sensitivity against artemisinin derivatives and its partner drugs in Africa is needed. Several studies have identified the polymorphisms of Pfmdr-1 N86Y gene as one of the main molecular markers involved in the development of tolerance / resistance to Lumefantrine and Amodiaquine; the two partner drug of AL and ASAQ respectively (Baliraine and Rosenthal, 2011; Baraka et al., 2015; Dokomajilar et al., 2006; Eyase et al., 2013; Holmgren et al., 2006, 2007; Sisowath et al., 2005, 2007; Somé et al., 2010). Here we report the results of a pilot study investigating the relationship between the polymorphism of the Pfmdr-1 N86Y alleles and the treatment outcome of ASAQ and AL in Burkina Faso.
MATERIAL AND METHODS
The study was carried out between October and December 2012 in Nanoro, Burkina Faso where malaria is hyper-endemic with a seasonal transmission from July to December. Plasmodium falciparum is the predominant malaria parasite and the commonest vectors are Anopheles gambiae ss, An. funestus and An. Arabiensis (Tinto et al., 2002). This was part of a pilot study that investigated the therapeutic efficacy of AL and ASAQ in patients ≥ 6 months of age with a molecular markers study nested into it. The study methodology has been described in detail elsewhere (ClinicalTrials.gov Identifier: NCT01697787). Briefly, patients with fever (axillary temperature of 37.5°C) or history of fever with a suspicion of malaria were screened after informed consent. Then, patients meeting the inclusion criteria were treated and followed up according to the WHO 28-day in vivo test (WHO, 2003). Outcomes were defined according to the WHO guidelines for monitoring antimalarial drug resistance (WHO, 2003).
Blood samples for the molecular analysis were collected on filter paper (Whatman 3, Maidstone, England) at day 0 before treatment and at the time of recurrent parasitaemia. DNA was extracted from dried blood spots using QIamp DNA miniKit (Qiagen, Germany) following the manufacturers procedures. Detection of Pfmdr1 N86Y polymorphisms was performed using nested PCR method followed by a restriction fragment length polymorphism (RFLP) (Dokomajilar et al., 2006): Briefly, the first round was done by using primers MDR1 5'-ATGGGTAAAGAGCAGAAAGA-3' and MDR2 5'-AACGCAAGTAATACATAAAGTCA-3' and then nested PCR was done by using primers MDR3 5'-TGGTAACCTCAGTATCAAAGAA-3' and MDR4 5'-A TAAACCTAAAAAGGAACTGG-3'. The second round (nested PCR) product was subjected to enzyme digestion with AflIII (New England Biolabs), which cuts only the mutant gene into 226 bp and 295 bp fragments. For each series of samples, water was used as a negative control, 3D7-clone DNA was used as the wild-type control and Dd2- DNA was used as the mutant control. Nested PCR was performed as well for the analysis of Msp-1 and Msp-2 to distinguish between recrudescence and new infection (Ranford-Cartwright et al., 1997). Data were double entered in an Excel database. Statistical analysis was performed using STATA (IC), version 8.0 software. Pfmdr-1 N86Y genotype was determined by the presence or absence of wild/mutant alleles. Differences between groups were assessed using the Chi-square test for proportions and a P-value < 0.05 was considered as statistically significant.
RESULTS
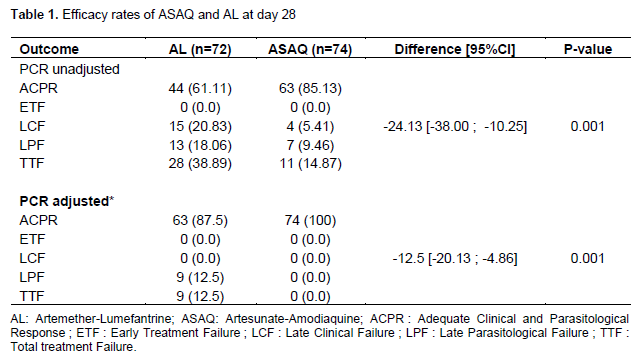
Out of 246 patients screened, 78.45% (193 patients) had a microscopically confirmed malaria infection. Out of them, 150 were randomized to receive either ASAQ (n=75) or AL (n=75). The two treatments’ outcomes are summarized in Table 1. At day 28, 74 patients completed their follow-up in the ASAQ arm against 72 patients in the AL arm. Unadjusted Adequate Clinical and Parasitological Response (ACPR) at day 28 was significantly higher in the ASAQ (85.13%) than in the AL arm (61.11%) [Risk difference = -24.13; 95% CI: -38.00; - 10.25 (p=0.001)]. Similarly, The PCR-adjusted ACPR was significantly higher in the ASAQ (100%) than in the AL arm (87.5%) [Risk difference = -12.50; 95% CI: -20.13; - 4.86 (p=0.001)]. The Pfmdr-1 N86Y gene was successfully genotyped in the blood samples of the 150 patients randomized at day 0. The overall prevalence of the mutant allele Pfmdr-1 Y86 was 18.67% [CI 95% (12.78 to 25.84)].
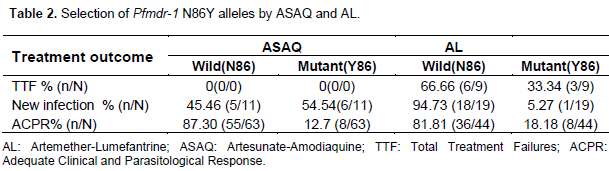
The prevalence of the two alleles before treatment in relation with treatments outcomes is summarized in Table 2. The prevalence of Pfmdr-1 Y86 mutation in the ASAQ arm was significantly higher among patients who had a recurrent parasitaemia (54.54%) than those classified as ACPR (12.70%) (p = 0.007). However, we did not see such difference in the AL arm (p = 0.65). Similarly, the prevalence of the mutant allele Pfmdr-1 Y86 before treatment (20.00%) was significantly lower than that found in post-treatment (55.56%) in the ASAQ arm (p = 0.01). However, we did not see such difference in the AL arm (p = 0.88).
DISCUSSION
Good efficacy of an ACT is reported when the partner drug is also efficacious (The Four Artemisinine-Based Combinations (4ABC) Study Group, 2011). The high rate of 100% ACPR reported in the ASAQ arm is an indicationof a good efficacy of Amodiaquine and confirm the results of previous studies conducted in Burkina Faso and comparing the two ACTs (Siribié, Diarra, Tiono, Soulama, & Sirima, 2012; Sirima et al., 2009; The Four Artemisinine-Based Combinations (4ABC) Study Group, 2011; Tinto et al., 2008, 2014; Zongo et al., 2007). The overall prevalence of the mutant allele Pfmdr-1 Y86 regardless of the treatment arm was surprisingly low when compared with that reported by previous studies; indicating a decrease of this mutation in Burkina Faso (Baraka et al., 2015; Somé et al., 2010; Tinto et al., 2003, 2008).
The Pfmdr-1 Y86 and Pfcrt T76 mutations have been identified as the main determinants for 4-aminoquinolines resistance including Amodiaquine (Tinto et al. 2003; Djimdé et al. 2015; Sondo et al. 2015). The decrease of the Pfmdr-1 Y86 mutation observed in our study may follow the same trend observed with Pfcrt T76 mutation after the malaria treatment policy change in endemic countries. Indeed, a decrease of the prevalence of Pfcrt T76 mutation was reported following the withdrawal of chloroquine from the treatment policy in many Africa endemic countries (Kublin et al., 2003; Laufer et al., 2010; Mwai et al., 2009; Sondo et al., 2015). These findings suggest that Amodiaquine resistance may be decreasing following the implementation of the new anti-malarial drug policy based on ACT in Burkina Faso.
An association between the polymorphism in Pfmdr-1 gene and the parasite response to arylaminoalcohols including lumefantrine has been reported with a significant increase of Pfmdr-1 86N wild type allele after exposure to the drug; suggesting that Lumefantrine exerts the opposite effect of amodiaquine on this locus (Duraisingh and Cowman, 2005; Sisowath et al., 2005). In addition, Pfmdr1 86N–carrying parasites have been associated with decreased sensitivity to lumefantrine in vitro, suggesting this allele as a potential marker of lumefantrine resistance (Baliraine and Rosenthal, 2011). We noticed in our study an overall high prevalence of Pfmdr-1 86N allele. However we did not observed an increase in the prevalence of the Pfmdr-1 86N in patients who had a recurrent parasitaemia samples than those classified as ACPR. Similarly, we did not observe an increase of the prevalence in the post-treatment samples than in pre-treatment samples. Therefore there was no significant selection of the Pfmdr1 86N allele after AL treatment in our study as reported previously in Africa (Baliraine and Rosenthal, 2011; Sisowath et al., 2005, 2007).
Overall, we did not see any linear association between the Pfmdr1-N86Y alleles and both AL and ASAQ treatments outcome. This lack of relationship confirms the difficulty to predict the individual treatment outcome by looking at molecular markers alleles in pre-treatment samples (Holmgren et al., 2006). This can be explained by the effect of the host immunity which could modify the relation between molecular markers and resistance; a phenomenon similar to what has been reported previously for CQ resistance (Djimdé et al., 2015; Tinto et al., 2003, 2008). Indeed, in our study, patients of all age groups including adults were enrolled when in most of studies where this relationship was established, study participants were mostly children (Baliraine and Rosenthal, 2011; Sisowath et al., 2005, 2007). However, further studies should be carried out exclusively in children to confirm this assumption in our study area.
In conclusion, our study showed a decrease of the Pfmdr-1 Y86 mutation in parasites strains circulating in Burkina Faso. ASAQ selected for parasites carrying the Pfmdr-1 Y86 mutation, however we were note able to demonstrate the reverse relationship between Pfmdr-1 86N allele and AL treatment as reported previously.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
We thank the study participants and the staff of the Nanoro Health District for their support. We are grateful to the Institute of Tropical Medicine, Belgium (FA3 – DGCD program) for the financial support of the laboratory work. We are also grateful to Kamala Ley-Thriemer, Maaike De Kroop and Raffaella Ravinetto for their contributions to the field study supervision.
REFERENCES
|
Baliraine FN, Rosenthal PJ (2011). Prolonged Selection of pfmdr1 Polymorphisms After Treatment of Falciparum Malaria With Artemether-Lumefantrine in Uganda. J. Infect. Dis. 204(7):1120-1124. |
|
|
Baraka V, Tinto H, Valea I, Fitzhenry R, Delgado-Ratto C, Mbonye MK, Erhart A (2015). In vivo selection of Plasmodium falciparum Pfcrt and Pfmdr1 variants by artemether-lumefantrine and dihydroartemisinin-piperaquine in Burkina Faso. Antimicrob. Agents Chemother. 59(1):734-7. |
|
|
Beshir KB, Sutherland CJ, Sawa P, Drakeley CJ, Okell L, Mweresa CK, Bousema T (2013). Residual Plasmodium falciparum parasitemia in Kenyan children after artemisinin-combination therapy is associated with increased transmission to mosquitoes and parasite recurrence. J. Infect. Dis. 208(12):2017-2024. |
|
|
Borrmann S, Sasi P, Mwai L, Bashraheil M, Abdallah A, Muriithi S, Marsh K (2011). Declining responsiveness of Plasmodium falciparum infections to artemisinin-based combination treatments on the Kenyan coast. PLoS ONE 6(11):e26005. |
|
|
Djimdé A, Doumbo OK, Steketee RW, Plowe CV (2015). Application of a molecular marker for surveillance of chloroquine-resistant falciparum malaria. Lancet 358(9285):890-891. |
|
|
Dokomajilar C, Nsobya SL, Greenhouse B, Rosenthal PJ, Dorsey G (2006). Selection of Plasmodium falciparum pfmdr1 alleles following therapy with artemether-lumefantrine in an area of Uganda where malaria is highly endemic. Antimicrob. Agents Chemother. 50(5):1893-1895. |
|
|
Dondorp AM, Nosten F, Yi P, Das D, Phyo AP, Tarning J, White NJ (2009). Artemisinin resistance in Plasmodium falciparum malaria. N. Engl. J. Med. 361(5):455-467. |
|
|
Duraisingh MT, Cowman AF (2005). Contribution of the pfmdr1 gene to antimalarial drug-resistance. Acta Trop. 94(3):181-90. |
|
|
Eyase FL, Akala HM, Ingasia L, Cheruiyot A, Omondi A, Okudo C, Johnson JD (2013). The Role of Pfmdr1 and Pfcrt in Changing Chloroquine, Amodiaquine, Mefloquine and Lumefantrine Susceptibility in Western-Kenya P. falciparum Samples during 2008-2011. PLoS ONE 8(5):e64299. |
|
|
Gansané A, Nébié I, Soulama I, Tiono A, Diarra A, Konaté AT, Sirima BS (2009). Change of antimalarial first-line treatment in Burkina Faso in 2005. Bull. Soc. Pathol. Exot. 102(1):31-35. |
|
|
Holmgren G, Gil JP, Ferreira PM, Veiga MI, Obonyo CO, Björkman A (2006). Amodiaquine resistant Plasmodium falciparum malaria in vivo is associated with selection of pfcrt 76T and pfmdr1 86Y. Infect. Genet. Evol. 6(4):309-14. |
|
|
Holmgren G, Hamrin J, Svärd J, Mårtensson A, Gil JP, Björkman A (2007). Selection of pfmdr1 mutations after amodiaquine monotherapy and amodiaquine plus artemisinin combination therapy in East Africa. Infect. Genet. Evol. 7(5):562-9. |
|
|
Kublin JG, Cortese JF, Njunju EM, Mukadam RAG, Wirima JJ, Kazembe PN, Plowe CV (2003). Reemergence of chloroquine-sensitive Plasmodium falciparum malaria after cessation of chloroquine use in Malawi. J. Infect. Dis. 187(12):1870-5. |
|
|
Laufer MK, Takala-Harrison S, Dzinjalamala FK, Stine OC, Taylor TE, Plowe CV (2010). Return of chloroquine-susceptible falciparum malaria in Malawi was a re-expansion of diverse susceptible parasites. J. Infect. Dis. 202(5):801-808. |
|
|
Lim P, Alker AP, Khim N, Shah NK, Incardona S, Doung S, Ariey F (2009). Pfmdr1 copy number and arteminisin derivatives combination therapy failure in falciparum malaria in Cambodia. Malar. J. 8:11. |
|
|
Maude RJ, Pontavornpinyo W, Saralamba S, Aguas R, Yeung S, Dondorp AM, White LJ (2009). The last man standing is the most resistant: eliminating artemisinin-resistant malaria in Cambodia. Malar. J. 8:31. |
|
|
Mwai L, Ochong E, Abdirahman A, Kiara SM, Ward S, Kokwaro G, Nzila A (2009). Chloroquine resistance before and after its withdrawal in Kenya. Malar. J. 8(1):106. |
|
|
Noedl H, Se Y, Sriwichai S, Schaecher K., Teja-Isavadharm P, Smith B, Chan Thap L (2010). Artemisinin resistance in Cambodia: a clinical trial designed to address an emerging problem in Southeast Asia. Clin. Infect. Dis. 51(11):e82-e89. |
|
|
Ranford-Cartwright LC, Taylor J, Umasunthar T, Taylor LH, Babiker HA, Lell B, Kremsner PG (1997). Molecular analysis of recrudescent parasites in a Plasmodium falciparum drug efficacy trial in Gabon. Trans. R. Soc. Trop. Med. Hyg. 91(6):719-724. |
|
|
Rogers WO, Sem R, Tero T, Chim P, Lim P, Muth S, Wongsrichanalai C (2009). Failure of artesunate-mefloquine combination therapy for uncomplicated Plasmodium falciparum malaria in southern Cambodia. Malar. J. 8(1):10. |
|
|
Siribié M, Diarra A, Tiono AB, Soulama I, Sirima SB (2012). Efficacité de l'artéméther-luméfantrine dans le traitement du paludisme simple de l'enfant en milieu rural au Burkina Faso en 2009. Bull. Soc. Pathol. Exot. 105(3):202-7. |
|
|
Sirima SB, Tiono AB, Gansané A, Diarra A, Ouédraogo A, Konaté AT, Taylor WR (2009). The efficacy and safety of a new fixed-dose combination of amodiaquine and artesunate in young African children with acute uncomplicated Plasmodium falciparum. Malar. J. 8(1):48. |
|
|
Sisowath C, Ferreira PE, Bustamante LY, Dahlström S, Mårtensson A, Björkman A, Gil JP (2007). The role of pfmdr1 in Plasmodium falciparum tolerance to artemether-lumefantrine in Africa. Trop. Med. Int. Health 12(6):736-42. |
|
|
Sisowath C, Strömberg J, Mårtensson A, Msellem M, Obondo C, Björkman A, Gil JP (2005). In vivo selection of Plasmodium falciparum pfmdr1 86N coding alleles by artemether-lumefantrine (Coartem). J. Infect. Dis. 191(6):10141017. |
|
|
Somé AF, Séré YY, Dokomajilar C, Zongo I, Rouamba N, Greenhouse B, Rosenthal PJ (2010). Selection of Known Plasmodium falciparum Resistance-Mediating Polymorphisms by Artemether-Lumefantrine and Amodiaquine- Sulfadoxine-Pyrimethamine but Not Dihydroartemisinin- Piperaquine in Burkina Faso. Antimicrob. Agents Chemother. 54(5):1949-1954. |
|
|
Sondo P, Derra K, Tarnagda Z, Nakanabo SD, Zampa O, Kazienga A, Tinto H (2015). Dynamic of plasmodium falciparum chloroquine resistance transporter gene Pfcrt K76T mutation five years after withdrawal of chloroquine in Burkina Faso. Pan Afr. Med. J. 21:1-4. |
|
|
The Four Artemisinine-Based Combinations (4ABC) Study Group (2011). A head-to-head comparison of four artemisinin-based combinations for treating uncomplicated malaria in African children: a randomized trial. PLoS Medicine 8(11):e1001119. |
|
|
Tinto H, Diallo S, Zongo I, Guiraud I, Valea I, Kazienga A, D'Alessandro U (2014). Effectiveness of artesunate-amodiaquine vs. artemether-lumefantrine for the treatment of uncomplicated falciparum malaria in Nanoro, Burkina Faso: a non-inferiority randomised trial. Trop. Med. Int. Health. 19(4):469-75. |
|
|
Tinto H, Guekoun L, Zongo I, Guiguemdé RT, D'Alessandro U, Ouédraogo JB (2008). Chloroquine-resistance molecular markers (Pfcrt T76 and Pfmdr-1 Y86) and amodiaquine resistance in Burkina Faso. Trop. Med. Int. Health 13(2):238-40. |
|
|
Tinto H, Ouédraogo JB, Erhart A, Van Overmeir C, Dujardin J-C, Van Marck E, D'Alessandro U (2003). Relationship between the Pfcrt T76 and the Pfmdr-1 Y86 mutations in Plasmodium falciparum and in vitro/in vivo chloroquine resistance in Burkina Faso, West Africa. Infect. Genet. Evol. 3(4):287-292. |
|
|
Tinto H, Zoungrana EB, Coulibaly SO, Ouedraogo JB, Traoré M, Guiguemde TR, D'Alessandro U (2002). Chloroquine and sulphadoxine-pyrimethamine efficacy for uncomplicated malaria treatment and haematological recovery in children in Bobo-Dioulasso, Burkina Faso during a 3-year period 1998-2000. Trop. Med. Int. Health 7(11): 925-930. |
|
|
World Health Organization (WHO) (2003). Assessment and monitoring of antimalarial drug efficacy for the treatment of uncomplicated falciparum malaria. Geneva. |
|
|
World Health Organization (WHO) (2006). Guidelines for the Treatment of Malaria 2006 Geneva: WHO. |
|
|
Zongo I, Dorsey G, Rouamba N, Tinto H, Dokomajilar C, Guiguemde RT, Ouedraogo JB (2007). Artemether-lumefantrine versus amodiaquine plus sulfadoxine-pyrimethamine for uncomplicated falciparum malaria in Burkina Faso: a randomised non-inferiority trial. Lancet 369:491-498. |
|
|
Zwang J, Olliaro P, Barennes H, Bonnet M, Brasseur P, Bukirwa H, Randrianarivelojosia M (2009). Efficacy of artesunate-amodiaquine for treating uncomplicated falciparum malaria in sub-Saharan Africa: A multi-centre analysis. Malar. J. 8(1):203. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


