Full Length Research Paper

ABSTRACT
Helminths and intestinal protozoa infections causes considerable human morbidity in low and middle-income countries. Determining the prevalence of intestinal parasites is necessary to define control strategies. In March and April 2019, we conducted a cross-sectional survey involving 350 schoolchildren living in urban area of the commune of Abobo, in Abidjan, in Côte d’Ivoire. Stool samples were obtained from the participants and were subjected to Kato-Katz technique and the formalin-ether concentration method for the detection of helminth eggs and intestinal protozoa cysts, respectively. Information on sociodemographic and socioeconomic characteristics concerning hygiene, sanitation and transmission of intestinal parasites were collected using a questionnaire administered to each selected pupil. Among schoolchildren, 71% (95% confidence interval [CI]: 66.1- 75.8%) were positive for one or more intestinal parasites. Schoolchildren were more infected with protozoan (69.7%, 95% CI: 64.6-74.5%) than helminths (6.9%, 95% CI: 4.4-10.0%). Prevalence of Schistosoma mansoni, Ascaris lumbricoides, hookworm and Trichuris trichiura were 0.9, 1.4, 2.0 and 2.9%, respectively. Prevalence for pathogenic protozoan namely, Giardia intestinalis and Entamoeba histolytica/dispar were 10.3 and 7.4%, respectively. Polyparasitism was found in 32,3% of the schoolchildren examined. The presence of cockroaches (Odds Ratio [OR] = 1.41, 95% CI: 1.30-1.53) and pets (OR =1.31, 95% CI: 1.15-1.60) were risk factors for Entamoeba histolytica/dispar infection in schoolchildren. This study confirms that protozoan infections are occurring among schoolchildren in Abidjan. Although, the prevalences of intestinal helminth infections are low; control efforts must continue in hope of interrupting the transmission of these parasitic infections in urban settings in Côte d’Ivoire.
Key words: Intestinal protozoa, Schistosomiasis, Soil-transmitted helminths, Schoolchildren, Côte d’Ivoire.
INTRODUCTION
Intestinal parasitic diseases due to infections with helminths (such as soil-transmitted helminthiasis (STH) and schistosomiasis) and intestinal protozoa (such as amoebiasis and giardiasis) are widespread in the world (Hotez et al., 2014; Utzinger et al., 2012). In tropical and subtropical regions, where climatic, ecological, socioeconomic and hygienic conditions are suitable for their transmission, STH and schistosomiasis are the most widespread parasitic neglected tropical diseases (NTDs) (Hotez et al., 2014; Utzinger et al., 2012). The roundworm (Ascaris lumbricoides), the whipworm (Trichuris trichiura) and the hookworms (Ancylostoma duodenale and Necator americanus) are the most common and accounted for 2.7 million disability-adjusted life years lost worldwide in 2019 (WHO, 2021). Globally, it’s estimated that 820 million people are infected with roundworms, 460 million with whipworms and 440 million with hookworms (WHO, 2018). For schistosomiasis, 230 million people are infected globally, with up to 700 million at risk of infection, and 200,000 deaths annually (WHO, 2022). The largest burden of schistosomiasis is in sub-Saharan Africa accounting for >90% of cases (WHO, 2021). The main species that cause schistosomiasis in humans in Africa are Schistosoma mansoni and S. haematobium (Hotez et al., 2014b). It is also estimated that 480 million people globally are infected by Amoebiasis, due to Entamoeba histolytica, with a high annual level of deaths ranging between 40 and over 100 thousand people (Espinosa Aranzales et al., 2018). Concerning giardiasis due to Giardia intestinalis, 280 million people worldwide are annually infected (Zajaczkowski et al., 2019). These infections lead to serious public health problem, as they cause anaemia, stunted growth in children and other physical and mental health problems (Alaofè et al., 2008; Bhat et al., 2013). Due to their association with poor sanitation and hygiene, it is observed a higher burden of disease among children of developing countries in sub-Saharan Africa, South-East Asia and Latin America (Errea et al., 2019; Jourdan et al., 2018). About 270 million preschool children and over 570 million school-age children live in these areas where there is the large-scale transmission of these parasites (WHO, 2016). Therefore, at the start of the new millennium, WHO endorsed preventive chemotherapy (PC) in school-age children for the control of STH and schistosomiasis. Later on, PC was further stipulated in the 2012 London Declaration on NCDs, with the ultimate goal of breaking the transmission of these parasitic diseases (WHO, 2016). In Côte d’Ivoire, a sub-Saharan African country, climatic, ecological and socio-economic conditions are suitable for transmission. Thus, STH, schistosomiasis, giardiasis and amoebiasis are endemic (Schmidlin et al., 2013)and are of a considerable public health relevance (Ouattara et al., 2010a; Yapi et al., 2016). Like all major sub-Saharan cities, Abidjan, the economic capital of Côte d’Ivoire, has undergone rapid urbanisation since independence, with an urbanisation rate of 95.8% in 1998 (INS, 1998). Abobo, the second most populated commune in Abidjan with a population of 1.031.658 people, that is 23.4% of Abidjan’s demographic weight, and an annual growth rate of 3.2% demographic weight, and an annual growth rate of 3.2% over an area of 9.000 ha is the full illustration of this uncontrolled urbanisation (INS, 2014). In Abobo, 53 under-equipped neighbourhoods occupy more than 70% of the municipal territory and offer precarious living conditions to the resident population. The spatial distribution of housing is 23% individual luxury housing, 7% grouped operations of companies and 66% courtyard housing (Diby, 2009). As a result, approximately 60% of the population of the commune lives in these precarious neighbourhoods (ONU-Habitat, 2012)where basic infrastructure is almost non-existent, making living conditions difficult and the environment polluted. These precarious living conditions favour the life cycle of many pathogens, including intestinal parasites. To control these intestinal parasites, Côte d’Ivoire has implemented the WHO recommendations by carrying out periodic deworming of school-age children. Hence, Preventive Chemotherapy is administered to school-age children with national coverage of more than 75% in 2018 (WHO, 2019), thus reaching the WHO target. With the achievement of this target, what is the current situation of intestinal parasitosis among school-age children in Côte d’Ivoire? In addition, studies have been carried out mostly in the rural settings in Côte d’Ivoire, but very few, are focalized on intestinal parasites in the urban environment. This study aims to determine the current prevalence and risk factors of intestinal parasites among schoolchildren in the commune of Abobo, in the district of Abidjan. The results might help health and school authorities to implement measures to improve schoolchildren’s health with regard to intestinal parasitic diseases.
MATERIALS AND METHODS
Ethical considerations
The protocol of this study obtained ethical approval from the “Comité National d’Éthique des Sciences de la Vie et de la Santé (CNESVS)” of Côte d’Ivoire (reference N°: 179-18/MSHP/CNESVS-kp). The health and education authorities (“Direction Régionale de l’Education Nationale et de l’Alphabétisation” [DRENA], school headmasters, teachers) of the city, parents/guardians and schoolchildren were informed about the objectives and procedures of the study. Written informed consent was obtained from parents/guardians and oral consent was obtained from the schoolchildren. Participation was voluntary and children could withdraw at any time without further obligation.
Study design and sample size calculation
A cross-sectional survey was conducted in Abobo (latitude 5° 20’56’ north and longitude 4° 00’ 42’ west), located in the district of Abidjan, in March and April 2019 to determine the prevalence and risk factors of intestinal infections among schoolchildren. In the afternoon before the class closes, consenting children were each given a plastic jar labelled with a unique identification number (ID) and asked to return the containers filled with a fresh morning stool sample (10-50 grams) the following day and collected between 8 and 10 am. The samples were transported the same day to the parasitology laboratory of the Department of Biology and Health of the Biosciences faculty at the University of Félix Houphouët-Boigny in Abidjan. A questionnaire was administrated to schoolchildren by sociologists to collect socio-demographic data (age, sex and residence) and environmental factors (presence of domestic animals, rats and cockroaches in the house; presence and type of toilets). The sample size (N) was determined based on the following formula:
N = (Z2 x p x (1-p) ) / e2 (Lwanga et al., 1991);
with “p” the expected prevalence of intestinal parasitic infections in the study area was set at 19.3% based on a previous study in Abidjan (Aka et al., 2016), the margin of error (e) was 5% and Z equal 1.96. The power of the study was set to 95%. Hence, the expected sample size was N = 264. Given 10% of loss to follow and the difficulty to get stool samples from the schoolchildren we finally calculate a sample size of 290 schoolchildren.
Laboratory procedures
The stool samples were examined by Kato-Katz technique (Katz et al., 1972)and ether-concentration method (Utzinger et al., 2010). On the day of collection, using the Kato-Katz method, two Thick smears of 41.7 mg were prepared for each stool sample for the diagnosis of S. mansoni and soil-transmitted helminths (T. trichiura, A. lumbricoides and hookworm) based on egg detection. About 1-2 grams of each stool sample was fixed in a Falcon tube filled with 15 ml of sodium acetate-acetic acid-formalin (SAF) (Garcia, 2016; WHO, 1994)and examined two months later using an ether-concentration method for the diagnosis of intestinal protozoa. The stool samples were examined by experienced laboratory technicians.
Statistical analysis
Statistical analyses were performed with STATA version 14.2 (Stata Corporation; College Station, TX, USA). Confidence Intervals (ICs) were used to compare the prevalence between parasitic infections. Chi-squared (X2) test of Pearson was used for comparison between groups (gender, age). Children were stratified into three age groups (5-8, 9-12, and 13-16 years).
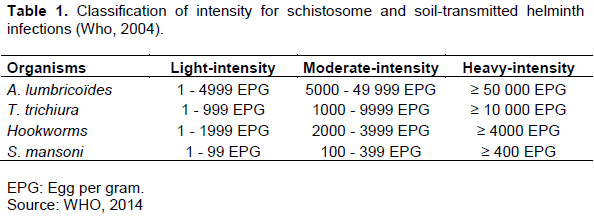
Associations between parasitic infections and risk factors were assessed by multivariable logistic regression. For each child, the arithmetic mean of species-specific helminth egg counts was calculated based on the duplicate Kato-Katz thick smear readings. At the commune level, the geometric mean egg counts were calculated. Helminth infection intensities were classified according to WHO guidelines into three categories (Table 1) (WHO, 2004). Concerning intestinal protozoa infection, intensities were recorded based on a semi-quantitative method distinguishing between light (1-5 cysts or trophozoites per slide); moderate (1 cyst or trophozoite per observation field at a magnification of ×400 or 500); and heavy (more than 1 cyst or trophozoite per observation field at a magnification of ×400 or 500) (Utzinger et al., 2010). A p-value below 0.05 was considered as significant for all statistical analyses.
RESULTS
Characteristics of the study population
The study involved 350 schoolchildren from two neighbourhoods in the commune of Abobo in Abidjan. There were 169 (48.3%) girls and 181 (51.7%) boys. The mean age was 10.8 years with extremes from 5 to 16 years. The most represented group was the 9-12 years old (73.1%). Most of the participants lived in Kennedy-Clouectcha (250) while 100 participants were from Habitat-Sogefiha.
Parasitic infections
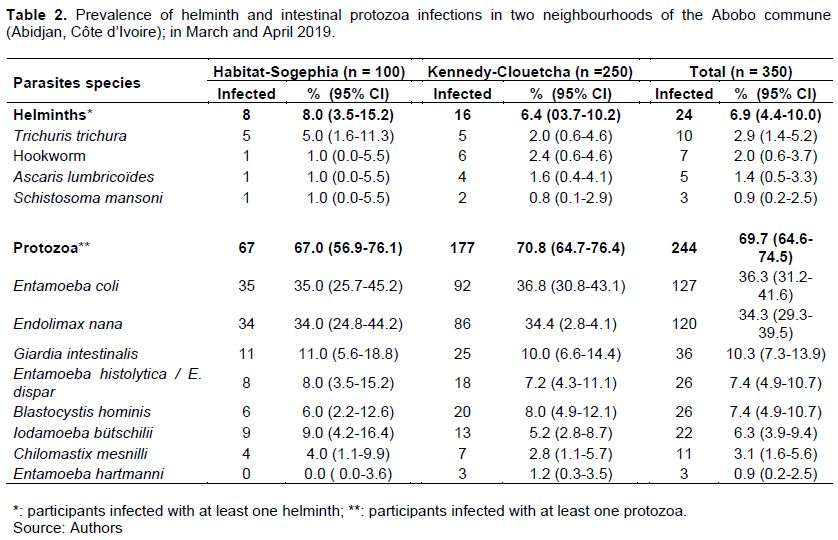
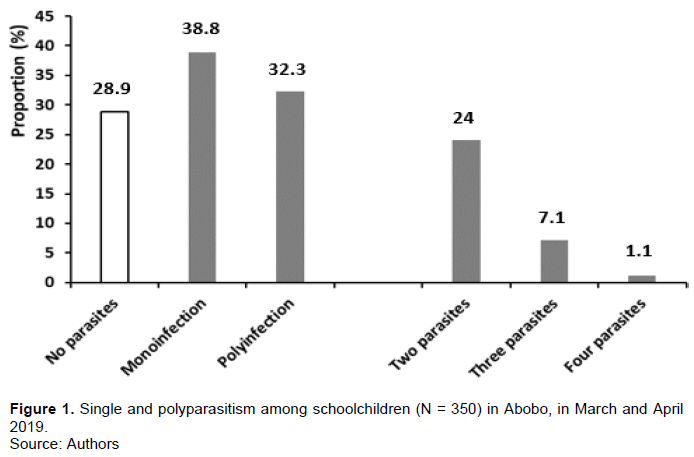
The prevalence of intestinal parasitic infections is shown in Table 2. Four species of helminths and eight species of protozoa were found in the stool samples. Of the 350 participant schoolchildren, 249 were positive for at least one intestinal parasite, resulting in an overall prevalence of 71.1%. Protozoan infections were most frequent with an overall prevalence of 69.7% (95% CI: 64.6-74.5%) compared to 6.9% (95% CI: 4.4-10.0%) for helminthiases. The species of helminths detected in the stool samples were Schistosoma mansoni (0.9%, 95% CI: 0.2-2.5%), Ascaris lumbricoides (1.4%, 95% CI: 0.5-3.3%), Ancylostoma spp. (2.0%, 95% CI: 0.6-3.7%) and Trichuris trichiura (2.9%, 95% CI :1.4-5.2%). From the eight species of protozoa, two pathogenic species were observed: Giardia intestinalis (10.3%, 95% CI: 7.3-13.9%) and Entamoeba histolytica/ dispar (7.4%, 95% CI: 4.9-10.7%). The other six non-pathogenic protozoan species observed were: Entamoeba coli (36.3%, 95% CI: 31.2-41.6%), Entamoeba hartmani (0.9%, 95% CI: 0.2-2.5%), Endolimax nana (34.3%, 95% CI: 29.3-39.5%), Iodamoeba butschili (6.3%, 95% CI: 3.9-9.4%), Blastocystis hominis (7.4%, 95% CI: 4.9-10.7%) and Chilomastix mesnili (3.1%, 95% CI: 1.6-5.6%). The most common species were Enatmoeba coli and Endolimax nana. Distribution of infections at the neighbourhood level shows a quite similar prevalence of helminths in the two habitats: 8.0% (95% CI: 3.5-15.2%) in Habitat-Sogefiha and 6.4% (95% CI: 3.7-10.2%) in Kennedy-Clouetcha. The distribution of protozoa was also comparable in Habitat-Sogefiha (67.0%, 95% CI: 56.9-76.1%) and Kennedy-Clouetcha (70.8%, 95% CI: 64.7-76.4%). Among the schoolchildren, 38.8% had single infection with 32.3% having multiple infection (Figure 1). Polyparasitism was stratified into those with two (24.0%), three (7.1%) and four (1.1%) parasites.
Intensity of infection
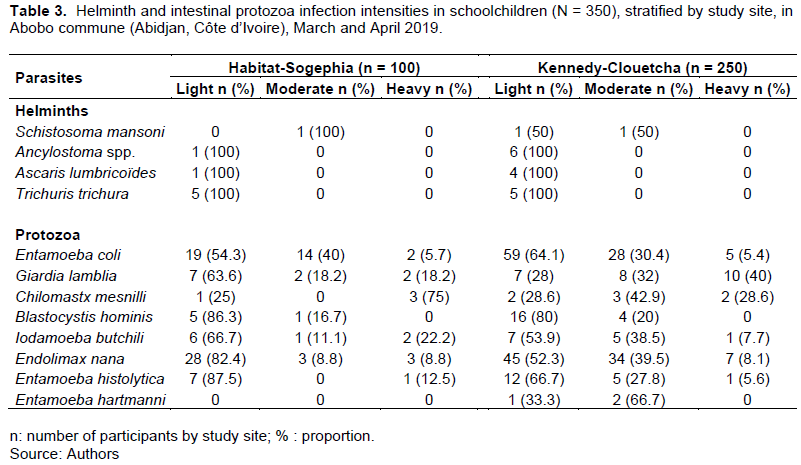
The intensities of the helminth infections were quite similar in the study area. However, the intensity of Ascaris lumbricoïdes (1024. 1 EPG, 95% CI: 159.4- 6579.5 EPG) was higher than the one of the other species:Ancylostoma spp. (38.7 EPG, 95% CI: 10.5-142.5 EPG) and Trichuris trichiura (55.2 EPG, 95% CI: 21.3-143.4 EPG). All helminth infections were light, but participants were moderately infected with S. mansoni in Habitat-Sogefiha and in Kennedy-Clouetcha (Table 3). Most of the participants infected with pathogenic intestinal protozoa were lightly infected with 63.6% (95% CI: 30.8-89.1%) and 87.5% (95% CI: 47.3-99.7%) for Giardia intestinalis and Entamoeba histolytica respectively in Habitat-Sogefiha. In Kennedy-Clouetcha, infected participants with Giardia intestinalis and Entamoeba histolytica were reported in the three categories of infection (Table 3).
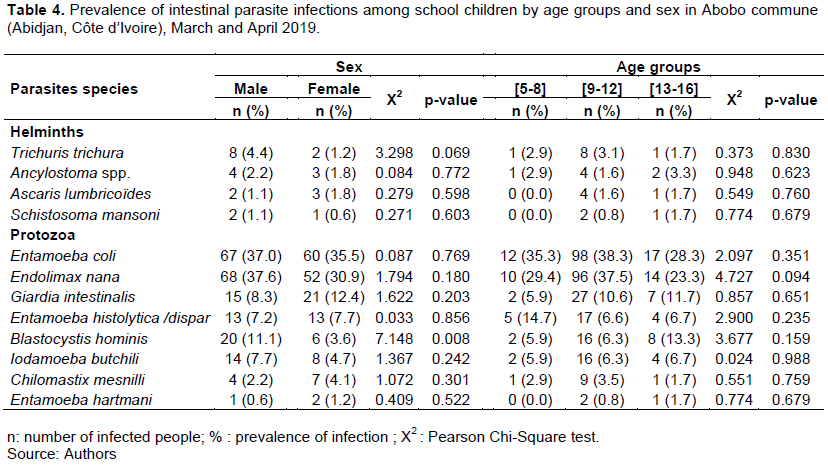
Parasite infection status stratified by age and sex
protozoa infections, stratified by sex and age groups in the study zone. Excepted Blastocystis hominis which had a significant difference (X2 = 7.148, p-value = 0.008) between males (11.1%) and females (3.6%), there was no statistically significant difference observed between gender, age and the status of the other intestinal parasites observed.
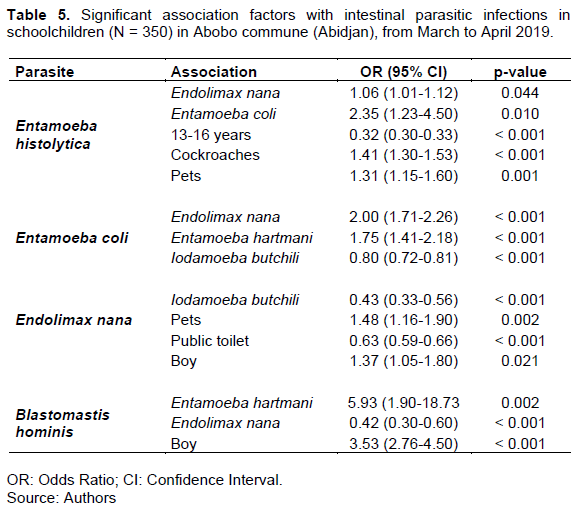
Associated factors with intestinal parasites infections
The significant associations between protozoan infections, sociodemographic factors determined based on logistic regression analyses are shown in Table 5. Being infected by Entamoeba histolytica was associated with Endolimax nana (Odds Ratio [OR]= 1.06, 95% CI: 1.23-4.50, p-value = 0.010). Children aged 13-16 years were less likely to be infected with Entamoeba histolytica compared to younger children (OR= 0.32, 95% CI: 0.30- Table 4 shows the prevalence of intestinal helminth and 0.33, p-value < 0.001). Cockroaches presence (OR = 1.41, 95% CI: 1.30-1.53, p-value < 0.001) and presence of pets (OR=1.31, 95% CI: 1.15-1.60, p-value = 0.001) were associated with Entamoeba histolytica infection and Endolimax nana was drived only by the presence of pets (OR = 1.48, 95% CI: 1.16-1.90, p-value = 0.002). Boys were more likely to be infected with Endolimax nana (OR=1.37, 95% CI: 1.05-1.80, p-value = 0,021) and Blastocystis hominis (OR=3.53, 95% CI : 2.76-4.50, p-value < 0.001) than girls.
DISCUSSION
Reliable estimates and updates on the status of intestinal parasites in vulnerable regions are important to guide control (Chege, 2020). Here, we assessed the prevalence and risk factors of intestinal parasitic infections among school children in the urban setting of the commune of Abobo (district of Abidjan) in Côte d’Ivoire. We found an overall prevalence of 71.1% for intestinal helminth and protozoa infection. This high prevalence of intestinal parasites would be due to poor hygienic conditions in Abobo, which would favour the maintaining and spreading of the parasites. Indeed, the commune of Abobo is known to be unhealthy, more than 40% of waste is not collected. Piles of waste in gutters, public squares and ravines are observed (N’Guessan and Alla, 2019). The accumulation of solid waste leads to the proliferation of insects and rodents carrying pathogens (Yonkeu et al., 2003). These animals with pathogens move into human habitats where they contaminate surfaces, objects and food (Graczyk et al., 2005). The prevalence of 71.1% observed in our study is consistent with what was observed in rural areas of Côte d’Ivoire (68%) (Yapi et al., 2005), in Jos township in north central Nigeria (69.9%) (Ikeh et al., 2007), and in Mecha district, Northwest Ethiopia (70.6%) (Feleke and Jember, 2018).
Some other studies have reported a higher prevalence of parasites than our results. Thus the prevalence of 84.8% has been reported in Côte d’Ivoire (Dancesco et al., 2005)and 86.2% in an archetypal African urban slum in Nigeria (Gyang et al., 2019). The prevalence of intestinal parasites, therefore, remains high in Africa and particularly in Côte d’Ivoire. This should challenge the authorities to take the necessary measures to increase the control of these parasites. The results showed that age or gender was not specifically associated with infections. This would mean that the participants were all exposed to these parasitic infections regardless of their age or sex. Studies conducted in urban areas in Ethiopia (Sitotaw and Shiferaw, 2020)and in Nigeria (Agbolade et al., 2007)also showed that gender and age were not risk factors for intestinal parasites. However in Côte d’Ivoire, in the city of Dabou, it was reported that boys had significantly higher prevalence of helminths and intestinal protozoa than girls (Traoré et al., 2011); while in Nepal (Rai et al., 2017)and Moroco (Tagajdid et al., 2012), girls were found more infected compared to boys.
Helminths were found at an overall prevalence of 6.9%. This prevalence is much lower than the prevalence of 59.5% (Kouame, 1995)and 45.0% (Menan et al., 1997)previously reported in Abobo (Abidjan). In our study, the prevalence of species-specific soil-transmitted helminths was considerably lower across all participants (A. lumbricoides [1.4%], T. trichiura [2.9%] and hookworm [2.0%]). Corroborating this finding, a study in Abobo found a low prevalence of Ascaris lumbrico?des (0,3%) and Trichuris trichiura (1,2%) (Coulibaly et al., 2017). These considerably lower rates might suggest that the various improvements due to education and socioeconomic development bring down the prevalence of intestinal parasites (Gabrielli et al., 2011; Levecke et al., 2014). In addition, the low prevalence of intestinal helminthiasis in school children in Abidjan could also be explained by the deworming campaigns with albendazole or mebendazole carried out periodically by the “Programme National de Lutte contre les Maladies Tropicales Négligées à Chimiothérapie Préventive” (PNLMTN-CP), and non-governmental organisations (NGOs); and the city’s sanitation efforts undertaken by local authorities. However, while helminth prevalence is not high in Abidjan, control efforts must continue to interrupt the transmission of these diseases. As with soil-borne helminths, the prevalence of Schistosoma mansoni was very low (0.9%). This indicates that S. mansoni is not common in Abidjan. This low prevalence of S. mansoni could be explained by urbanisation, which is reflected in the availability of drinking water, so the populations do not go to the existing waterways to drink, and the absence of agricultural practices in these waterways. Moreover, parents aware of the dangers linked to freshwater, do not allow their children to go swimming. There is therefore less risk of being infected by Schistosoma mansoni. Then, the few cases presented could be cases imported by children during their holiday stays in endemic areas. However, our survey did not allow us to specify the exact origin of these cases. Similarly, a low prevalence (2.7%) of S. mansoni was found in a previous study Abobo (Coulibaly et al., 2017). However, higher prevalences have been reported in bilharzia-endemic regions: 53.1% in urban Azaguie Gare (Coulibaly et al., 2012)and 9.5% in the western of Côte d’Ivoire (Assaré et al., 2020).
Overall, a high prevalence (69.7%) of intestinal protozoa was observed in the current study. The most common intestinal protozoa were non-pathogenic species, E. coli and E. nana, with an overall prevalence of 36.3 and 34.3%, respectively. Although these are non-pathogenic protozoa, this finding highlights the high level of faecal contamination around the community (Savichtcheva and Okabe, 2006). Indeed, the commune of Abobo is characterised by a lack of sanitation infrastructures.
Thus, 63.5% of households evacuate their wastewater directly into the street from washing, dishwashing and toilets (Tuo, 2019). In addition, 35.7% of households use manual pumpers for emptying septic tanks who, in their process, transfer the waste to a new hole dug in front of the houses, in the open air (Tuo, 2019). The consequence is faecal pollution of the environment exposing the population to a high risk of contamination. Similarly, high prevalences of protozoa (78.6%) were reported in a rural area in human populations in Taï National Park, Côte d’Ivoire (Roland et al., 2019). Although the prevalence of protozoa was high, the prevalence of the pathogenic protozoa G. intestinalis (10.3%) and E. histolytica (7.4%) was low. Entamoeba histolytica/dispar and Giardia intestinalis were also reported at low prevalences of 7 and 2.7%, respectively in 2017 in Abobo (Coulibaly et al., 2017). In contrast, slightly higher prevalences of 18.8% for E. histolytica/dispar and 13.9% for G. intestinalis were observed in the urban area of Agboville, in southern Côte d’Ivoire (Ouattara et al., 2010a). As described in tropical and subtropical countries, polyparasitism was observed in this study. This can be explained by the lack of hygiene in our study area. Several digestive parasites are thus found in the same environment and are also transmitted in the same way (Ouattara et al., 2010b). The presence of more than one parasite species in an individual is an alarming situation, as multiple species infection may increase susceptibility to other parasites (Zhang et al., 2016).
The current study shows that children who live in close proximity to pets were more susceptible to infection (OR=1.31, 95% CI: 1.15-1.60, p-value = 0.001). This may be since pets (dogs and cats) can serve as possible reservoirs for in-contact humans, especially those who handle shelter-resident and client-owned animals (Mohammadpour et al., 2020). Deworming of house hold pets is therefore recommended to help to reduce the prevalence of intestinal parasitic infections (Forson et al., 2017). This is in line with a study in urban areas of southern Algeria that found that the prevalence of intestinal parasites, particulary Giardia intestinalis was associated with pet ownership (Sebaa et al., 2021). Entamoeba histolytica/dispar was positively associated with the presence of cockroaches (OR = 1.41, 95% CI:1.30-1.53, p-value < 0.001). Indeed, because of the way they live in sewers and toilets, these insects are likely to host eggs and oocysts of intestinal parasites contained in the faeces of humans or animals. This was confirmed in a study carried out in Ethiopia which found that cockroaches serve as carriers of human intestinal parasites (Kinfu and Erko, 2008). The fact that boys were more likely to be infected with Blastocystis hominis and Endolimax nana than girls could be explained by some of the games they play, such as playing in run-off water where they can be infected with parasite eggs and cysts.
The current study has some limitations. Firstly, the relatively small number of schools participating in the study due to the refusal of some of the Habitat-Sogefia schools to participate and the single stool sample examined might influence the observed prevalence of parasitic infections. Additionally, data could not be compared between the two neighbourhoods Kennedy-Clouetcha and Habitat-Sogefia because of the difference in the number of schools (5 vs 2). Secondly, the diagnosis of intestinal parasites was based on Kato-Katz and formalin concentration, which are less sensitive. To increase the sensitivity and to have a more precise understanding of the diversity of pathogenic organisms, multiple stool samples and a suite of highly sensitive diagnostic approaches such as polymerase chain reaction (PCR) or a metagenomics approach should be considered (Becker et al., 2013; Schneeberger et al., 2016).
CONCLUSION
Our study confirms the presence of intestinal parasitic infections among schoolchildren in urban setting of Abobo (Abidjan) in Côte d’Ivoire, with a prevalence of 6.9% for helminth and 69.7% for protozoan infections. With similarly high prevalences in Sogefiha (69%) and Kennedy-Clouetcha (72%), those parasites presented no differences between age groups. In hope of effectively controling intestinal parasitic infections in schools in Côte d’Ivoire, regular mass deworming must be continuous and combined with health education and sanitation.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
REFERENCES
|
Agbolade OM, Agu NC, Adesanya OO, Odejayi AO, Adigun AA, Adesanlu EB, Ogunleye FG, Sodimu AO, Adeshina SA, Bisiriyu GO, Omotoso OI, Udia KM (2007). Intestinal helminthiases and schistosomiasis among school children in an urban center and some rural communities in southwest Nigeria. The Korean Journal of Parasitology (45):233-238. |
|
|
Aka N, Kouadio Y, Gisele C (2016). Prevalence of Intestinal Parasitic Infections among Maids in Abidjan, Cote D'ivoire. Journal of Bacteriology and Parasitology 7(263):2. |
|
|
Alaofè H, Zee J, Dossa R, O'Brien HT (2008). Intestinal parasitic infections in adolescent girls from two boarding schools in southern Benin. Transactions of the Royal Society of Tropical Medicine and Hygiene 102(7):653-661. |
|
|
Assaré RK, N'Tamon RN, Bellai LG, Koffi JA, Mathieu T-BI, Ouattara M, Hürlimann E, Coulibaly JT, Diabaté S, N'Goran EK, Utzinger J (2020). Characteristics of persistent hotspots of Schistosoma mansoni in western Côte d'Ivoire. Parasites and Vectors 13(1):1-16. |
|
|
Becker SL, Vogt J, Knopp S, Panning M, Warhurst DC, Polman K, Marti H, von Müller L, Yansouni CP, Jacobs J, Bottieau E, Sacko M, Rijal S, Meyanti F, Miles MA, Boelaert M, Lutumba P, van Lieshout L, N'Goran EK, Chappuis F, Utzinger J (2013). Persistent digestive disorders in the tropics: causative infectious pathogens and reference diagnostic tests. BMC Infectious Diseases (13):1-21. |
|
|
Bhat V, Vasaikar S, Nxasana N, Baba K (2013). Prevalence of intestinal parasites in primary school children of mthatha, Eastern Cape Province, South Africa. Annals of Medical and Health Sciences Research 3(4):511-516. |
|
|
Chege N (2020). The prevalence of intestinal parasites and associated risk factors in school-going children from informal settlements in Nakuru town, Kenya. Malawi Medical Journal 32(2):80-86. |
|
|
Coulibaly G, Yao KP, Koffi M, Ahouty BA, Louhourignon LK, N'Cho M, N'Goran EK (2017). Paludisme et parasitoses digestives chez la femme enceinte de la commune d'Abobo (Abidjan, Côte d'Ivoire). Bulletin de la Societe de Pathologie Exotique 110(2):85. |
|
|
Coulibaly JT, Fürst T, Silué KD, Knopp S, Hauri D, Ouattara M, Utzinger J, N'Goran EK (2012). Intestinal parasitic infections in schoolchildren in different settings of Côte d'Ivoire: effect of diagnostic approach and implications for control. Parasites and Vectors 5(1):1-11. |
|
|
Dancesco P, Akakpo C, Iamandi I, Abeu J, Tshipeta M, Kacou E (2005). [Intestinal parasitoses in a village of Côte d'Ivoire. II: Relationship between intestinal parasitoses, physical and physiological development and child nutrition]. Cahiers D'études et de Recherches francophones/Santé,15(1):11-16. |
|
|
DIBY KM (2009). Dynamique d'urbanisation de l'espace périphérique nord de la ville d'Abidjan?: le cas de la commune d'Abobo. Thèse unique de doctorat, Abidjan, Université de Cocody. Université de Cocody, Abidjan, Côte d'Ivoire. |
|
|
Errea R.A, Vasquez-Rios, G, Calderon ML, Siu D, Duque, KR, Juarez, LH, Gallegos R, Uriol C, Rondon CR, Baca KP, Fabian RJ, Canales M, Terashima A, Marcos LA, Samalvides F (2019). Soil-Transmitted Helminthiasis in Children from a Rural Community Taking Part in a Periodic Deworming Program in the Peruvian Amazon. The American Journal of Tropical Medicine and Hygiene (101):636-640. |
|
|
Espinosa Aranzales AF, Radon K, Froeschl G, Pinzón Rondón ÁM, Delius M (2018). Prevalence and risk factors for intestinal parasitic infections in pregnant women residing in three districts of Bogotá, Colombia. BMC Public Health (18):1071. |
|
|
Feleke BE, Jember TH (2018). Prevalence of helminthic infections and determinant factors among pregnant women in Mecha district, Northwest Ethiopia: a cross sectional study. BMC Infectious Diseases (18): 373. |
|
|
Forson AO, Arthur I, Olu-Taiwo M, Glover KK, Pappoe-Ashong PJ, Ayeh-Kumi PF (2017). Intestinal parasitic infections and risk factors: a cross-sectional survey of some school children in a suburb in Accra, Ghana. BMC Research Notes (10):1-5. |
|
|
Gabrielli A-F, Montresor A, Chitsulo L, Engels D, Savioli L (2011). Preventive chemotherapy in human helminthiasis: theoretical and operational aspects. Transactions of the Royal Society of Tropical Medicine and Hygiene 105(12):683-693. |
|
|
Garcia LS (2016). Diagnostic medical parasitology, 6th edition. ed. ASM Press, Washington, DC. |
|
|
Graczyk TK, Knight R, Tamang L (2005). Mechanical Transmission of Human Protozoan Parasites by Insects. Clinical Microbiology Reviews 18(1):128-132. |
|
|
Gyang VP, Chuang T-W, Liao C-W, Lee Y-L, Akinwale OP, Orok A, Ajibaye O, Babasola AJ, Cheng P-C, Chou C-M, Huang Y-C, Sonko P, Fan C-K (2019). Intestinal parasitic infections: Current status and associated risk factors among school aged children in an archetypal African urban slum in Nigeria. Journal of Microbiology, Immunology and Infection (52):106-113. |
|
|
Hotez PJ, Alvarado M, Basáñez MG, Bolliger I, Bourne R, Boussinesq, M, Naghavi M (2014). The global burden of disease study 2010: interpretation and implications for the neglected tropical diseases. PLoS Neglected Tropical Diseases 8(7):2865. |
|
|
Ikeh EI, Obadofin MO, Brindeiro B, Baugherb C, Frost F, Vanderjagt D, Glew RH (2007). Intestinal parasitism in Magama Gumau rural village and Jos township in north central Nigeria. The Nigerian Postgraduate Medical Journal 14(4):290-295. |
|
|
INS RGPH (1998). Recensement Général de la Population et de l'Habitation, Rapport, Abidjan. INS 1(1). |
|
|
INS RGPH (2014). Recensement général de la Population et de l'habitat, 2014. Ins. |
|
|
Jourdan PM, Lamberton PHL, Fenwick A, Addiss DG (2018). Soil-transmitted helminth infections. The Lancet (391):252-265. |
|
|
Katz N, Chaves A, Pellegrino J (1972). A simple device for quantitative stool thick-smear technique in Schistosomiasis mansoni. Revista do Instituto de Medicina Tropical de São Paulo 14(6):397-400. |
|
|
Kinfu A, Erko B (2008). Cockroaches as carriers of human intestinal parasites in two localities in Ethiopia. Transactions of the Royal Society of Tropical Medicine and Hygiene (102):1143-1147. |
|
|
Kouame BB (1995). Bilan des helminthiases intestinales chez les enfants d'âge scolaire dans les trois communes de la ville d'Abidjan (Abobo, Adjamé, Cocody) (Rapport). Université de Cocody, Faculté de Médecine, Abidjan, Côte d'Ivoire. |
|
|
Levecke B, Montresor A, Albonico M, Ame SM, Behnke JM, Bethony JM, Noumedem CD, Engels D, Guillard B, Kotze AC, Krolewiecki AJ, McCarthy JS, Mekonnen Z, Periago MV, Sopheak H, Tchuem-Tchuenté L-A, Duong TT, Huong NT, Zeynudin A, Vercruysse J (2014). Assessment of Anthelmintic Efficacy of Mebendazole in School Children in Six Countries Where Soil-Transmitted Helminths Are Endemic. PLoS Neglected Tropical Diseases 8(10):3204.. |
|
|
Lwanga SK, Lemeshow S and World Health Organization (1991). Détermination de la taille d'un échantillon dans les études sanométriques: manuel pratique. Organisation mondiale de la santé. |
|
|
Menan EI, Nebavi NG, Adjetey TA, Assavo NN, Kiki-Barro PC, Kone M (1997). [Profile of intestinal helminthiases in school aged children in the city of Abidjan]. Bulletin de la Societe de Pathologie Exotique 90(1):51-54. |
|
|
Mohammadpour I, Bozorg-Ghalati F, Gazzonis AL, Manfredi MT, Motazedian MH, Mohammadpour N (2020). First molecular subtyping and phylogeny of Blastocystis sp. isolated from domestic and synanthropic animals (dogs, cats and brown rats) in southern Iran. Parasites Vectors (13):365. |
|
|
N'Guessan LJ-B, Alla MDA (2019). Les risques sanitaires attribuables aux déchets solides et liquides dans la commune d'abobo à Abidjan (côte d'ivoire). RSS P 21. |
|
|
ONU-Habitat (2012). Côte d'Ivoire?: Profil urbain d'ABOBO. ONU-HABITAT, Nairobi, Kenya. |
|
|
Ouattara M, N'guéssan NA, Yapi A, N'goran EK (2010a). Prevalence and spatial distribution of Entamoeba histolytica/dispar and Giardia lamblia among schoolchildren in Agboville area (Côte d'Ivoire). PLoS Neglected Tropical Diseases 4:e574. |
|
|
Ouattara M, N'Guéssan NA, Yapi A, N'Goran EK (2010b). Prevalence and Spatial Distribution of Entamoeba histolytica/dispar and Giardia lamblia among Schoolchildren in Agboville Area (Côte d'Ivoire). PLoS Neglected Tropical Diseases 4:e574. |
|
|
Rai L, Saud B, Paudel G, Dhungana G (2017). Prevalence of Intestinal Parasitic Infection among Rural Area School Children of Lokhim VDC, Nepal. JMEN 4. |
|
|
Roland KWY, Sylvie P, Fidèle BK, Kouakou Hilaire B, Eliezer NK (2019). Parasites Gastro-Intestinaux des Populations Humaines du Parc National de Taï, Côte d'Ivoire. European Scientific Journal 15(36):27-44. |
|
|
Savichtcheva O, Okabe S (2006). Alternative indicators of fecal pollution: Relations with pathogens and conventional indicators, current methodologies for direct pathogen monitoring and future application perspectives. Water Research 40(13):2463-2476. |
|
|
Schmidlin T, Hürlimann E, Silué KD, Yapi RB, Houngbedji C, Kouadio BA, Acka-Douabélé CA, Kouassi D, Ouattara M, Zouzou F, Bonfoh B, N'Goran EK, Utzinger J, Raso G (2013). Effects of Hygiene and Defecation Behavior on Helminths and Intestinal Protozoa Infections in Taabo, Côte d'Ivoire. PLoS One 8(6):e65722. |
|
|
Schneeberger PHH, Becke, SL, Pothier JF, Duffy B, N'Goran EK, Beuret C, Frey JE, Utzinger J (2016). Metagenomic diagnostics for the simultaneous detection of multiple pathogens in human stool specimens from Côte d'Ivoire: a proof-of-concept study. Infection, Genetics and Evolution 40:389-397. |
|
|
Sebaa S, Behnke JM, Baroudi D, Hakem A, Abu-Madi MA (2021). Prevalence and risk factors of intestinal protozoan infection among symptomatic and asymptomatic populations in rural and urban areas of southern Algeria. BMC Infectious Diseases 21:888 |
|
|
Sitotaw B, Shiferaw W (2020). Prevalence of Intestinal Parasitic Infections and Associated Risk Factors among the First-Cycle Primary Schoolchildren in Sasiga District, Southwest Ethiopia. Journal of Parasitology Research pp. 1-13. |
|
|
Tagajdid R, Lemkhente Z, Errami M, El Mellouki W, Lmimouni B (2012). Portage parasitaire intestinal chez l'enfant scolarisé à Salé, Maroc. Bulletin de la Société de Pathologie Exotique 105:40-45. |
|
|
Traoré SG, Odermatt P, Bonfoh B, Utzinger J, Aka ND, Adoubryn KD, Assoumou A, Dreyfuss G, Koussémon M (2011). No Paragonimus in high-risk groups in Côte d'Ivoire, but considerable prevalence of helminths and intestinal protozoon infections. Parasites Vectors 4:96. |
|
|
Tuo P (2019). Gestion des eaux usées et nuisances sanitaires dans les cadres de vie des populations d'Abobo Kennedy Clouetcha (Abidjan, Côte d'Ivoire). Revue Africaine des Sciences Sociales et de la Santé Publique 1(1) :74-90. |
|
|
Utzinger J, Becker S, Knopp S, Blum J, Neumayr A, Keiser J, Hatz C (2012). Neglected tropical diseases: diagnosis, clinical management, treatment and control. Swiss Medical Weekly. |
|
|
Utzinger J, Botero-Kleiven S, Castelli F, Chiodini PL, Edwards H, Köhler N, Gulletta M, Lebbad M, Manser M, Matthys B, N'Goran EK, Tannich E, Vounatsou P, Marti H (2010). Microscopic diagnosis of sodium acetate-acetic acid-formalin-fixed stool samples for helminths and intestinal protozoa: a comparison among European reference laboratories. Clinical Microbiology and Infection 16(3):267-273. |
|
|
World Health Organization (WHO) (1994). Planches pour le diagnostic des parasites intestinaux. World Health Organization, Place of publication not identified. |
|
|
World Health Organization (WHO) (2022). WHO guideline on control and elimination of human schistosomiasis. World Health Organization, Geneva. |
|
|
World Health Organization (WHO) (2021). Schistosomiasis and soiltransmitted helminthiases: progress report, 2020. Weekly Epidemiological Record P 96. |
|
|
World Health Organization (WHO) (2019). Schistosomiasis and soil transmitted helminthiases: numbers of people treated in 2018. WER9450-eng pp. 601-612. |
|
|
World Health Organization (WHO) (2018). Lignes directrices?: la chimioprévention pour combattre les géohelminthiases dans les groupes de population à risque. Organisation mondiale de la Santé. |
|
|
World Health Organization (WHO) (2016). Summary of global update on preventive chemotherapy implementation in 2015. Weekly Epidemiological Record 91:456-459. |
|
|
World Health Organization (WHO) (2004). Prevention and control of schistosomiasis and soil-transmitted helminthiasis WHO/CDS/CPE/PVC/2004.9, OMS, série de rapports techniques. World Health Organization, Genève. |
|
|
Yapi HF, Ahiboh H, Monnet D, Yapo AE (2005). [Intestinal parasites, haematological profile and anthropometric status of schoolchildren in Cotê d'Ivoire]. Sante (Montrouge, France) 15(1):17-21. |
|
|
Yapi RB, Chammartin F, Hürlimann E, Houngbedji CA, N'Dri PB, Silué KD, Utzinger J, N'Goran EK., Vounatsou P, Raso G (2016). Bayesian risk profiling of soil-transmitted helminth infections and estimates of preventive chemotherapy for school-aged children in Côte d'Ivoire. Parasites Vectors 9:162. |
|
|
Yonkeu S, Maïga AH, Wethé J, Mampouya M, Maga GP (2003). Conditions socio-économiques des populations et risques de maladies?:Le bassin versant du barrage de Yitenga au Burkina Faso. Vertigo. |
|
|
Zajaczkowski P, Mazumdar S, Conaty S, Ellis JT, Fletcher-Lartey SM (2019). Epidemiology and associated risk factors of giardiasis in a peri-urban setting in New South Wales Australia. Epidemiology and Infection (147):e15. |
|
|
Zhang S-X, Zhou Y-M, Xu W, Tian L-G, Chen J-X, Chen S-H, Dang Z-S, Gu W-P, Yin J-W, Serrano E, Zhou X-N (2016). Impact of co-infections with enteric pathogens on children suffering from acute diarrhea in southwest China. Infectious Diseases of Poverty 5(1):1-13. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


