ABSTRACT
The American trypanosomiasis or Chagas disease, caused by the protozoan Trypanosomacruzi, affects the Paraíba hinterland region that is an endemic region by having multiple individuals being affected by it often, the main vector of transmission, is the triatomine, aka barber, they are considered to have very high dispersion. Teixeira-PB is a city that is located in that region, and a lot of people have found the vector in their homes, and also who having relatives who affected by the protozoan. The data that express this characteristic reflect the importance of applying preventive measures in this city, because the political authorities, according to information collected via questionnaire, in recent years seem to give much attention to fight the disease. Another contributing factor to describe the absence of measures that constrain the vector explains why individuals living in urban or rural areas, who had contact with the vector have been unwilling to carry out serological tests to diagnose Chagas disease, and were either sent by the health department to perform a procedure like. Therefore, the fact that this city is in need of prophylaxis, which cover up the residents to contract and spread an incurable and silent epidemic like this that can leave the carrier in clinical status of high risk of death.
Key words: Chagas disease, Trypanosomacruzi, Triatominesbugs, endemic area
The epidemiological cycles are responsible for infecting and decimate countless human beings in the environment, this fact requires a lot of attention because sometimes they may not realize the symptoms of an epidemic that can lead individuals to death. In this case, the Chagas disease fits unobtrusively and is gaining dispersal into the environment. One of the goals of this research is to describe different forms of contracting this disease, that is, emphasize the means of transmission of the epidemiological agent, the protozoan Trypanosoma cruzi, because the facility of infectability of the protozoan is a reason compromising the health of human beings. The T. cruzi belongs to the protozoa kingdom, phylum Sarcomastigophora, Zoomastigophorea class, Kinetoplastida order and trypanosomes family, genres: Trypanosoma and specie: T .cruzi. (Neves, 2005). According to Teixeira et al. (2011), the disease is considered by the World Health Organization (WHO) as a case of global and incurable health, moreover, it is also influenced by the rural exodus and the migration that took evolution in the XIX and XX,but also leaves its victims in the XXI century. The First National Survey conducted in 1975 to 1980 period recorded a prevalence of 4.2% positivity for Brazil (SILVA; GOLDENBERG, 2008). "The disease was named after the discovery of the parasite by the researcher Carlos Chagas, in 1909, in the region of Lassance, Minas Gerais." (LIMA, 2010). Since the discovery is considered a very important epidemiological disease.
The most comprehensive form of transmission of Chagas disease occurs by its vector, the Triatomine, according to Souza (2007), correspond to 80% of cases of transmission. The triatomines when feeding defecate and their feces infected with T. cruzi comes in contact with the skin of the host. Through the bite plus the act of scratching, the mucosa of the human being infects, concluding the infection stage. "Mucous even when intact, do not prevent the penetration of T. cruzi in the body. The conjunctival mucosa is the most affected" (DIAS, 2009).
According to Mangueira (2013), "The Northeast region, the epidemiological scenario of Chagas disease has always been important; this is due to high concentration of vector species". In Paraiba, Chagas disease has been maintaining high levels, especially in the hinterland region, an area considered endemic (Souza, 2007), the city studied here is located in the hinterland of Paraiba.
The relentless fight against the insect vector and the search for decent housing for individuals exposed to this endemic disease, all depend on a firm political will, based on human dignity and the duties and responsibilities of the State (Chagas, 1911), cited by (Dias,1997).
Nowadays, preventive measures remain the same as indicated by Chagas in 1911. Prophylaxis of Chagas disease is closely linked to improving the living conditions of the peasant and the modification of the secular habit of destruction of fauna and flora (Neves, 2005). Consequently, for the ultimate control of Chagas disease, should social reforms in endemic regions should be put in place.
Objective of study
This study, in general, was conducted to determine the prevalence of American trypanosomiasis rate among the population in the city of Teixeira-PB. The survey data helped to determine the prevalence of infectious population by T. cruzi, between female and male, age and educational level in different parts of the city contributing to upgrade the status of Chagas disease in the region, and to promote an alert to the implementation of public policies to control the disease.
Time and location of study
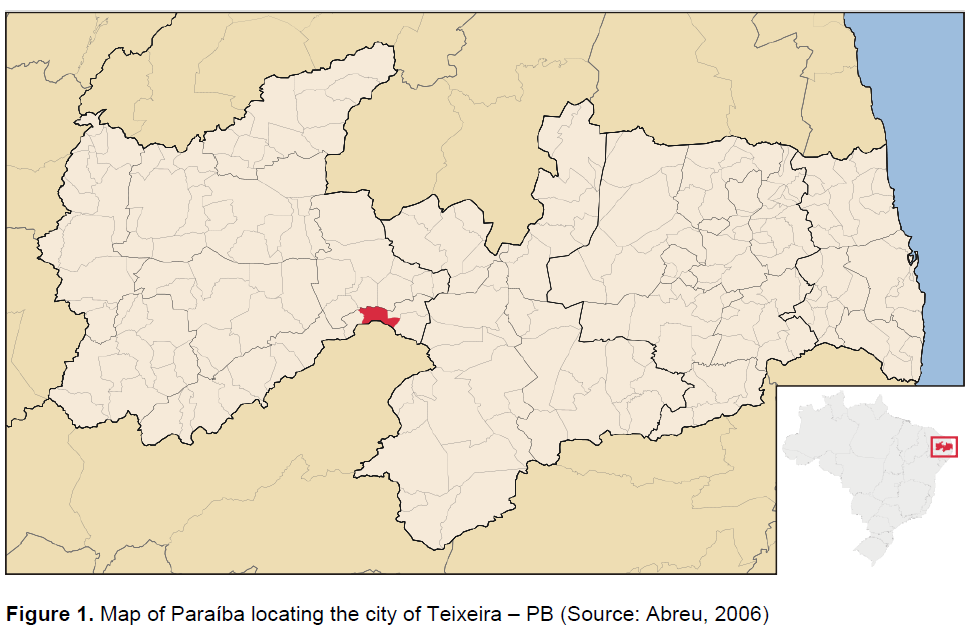
The study was conducted for ten months, from August 2013 to March 2014. The basic information was provided by the Department of Sanitary Surveillance and IBGE (Brazilian Institute of Geography and Statistics). The study was conducted in the municipality of Teixeira- PB, located in the middle region of Paraiba hinterland and micro region of Teixeira Hill. According to the IBGE (2010), its population was estimated at 14,153 people. Land area of 160.9 km², the geographical position is determined by the parallel of latitude 07°13'22 south at its intersection with the meridian of longitude 37°15'15 west longitude, with a distance of 308 km from João Pessoa, via Taperoá (Figure 1).
The collected data were analyzed at the Federal University of Campina Grande (UFCG) on the campus of Patos-PB, local processing of data from the questionnaires, analysis of laboratory tests records, statistical calculations and research of endemic framework of Chagas Disease in cities in the Paraiba hinterlands (Olhod'Água, Coremas, Piancó, PedraBranca, São José de Caiana and Igaracy) close to Teixeira was also carried out.
The study was conducted through research of laboratory tests of diagnostic of Chagas disease, negative and positive, and the questionnaire for updating and comparing data on knowledge of the local population about American trypanosomiasis.
The survey data of the exams was collected at the Municipal Laboratory of Public Health Dr. Maria Dilva Carlos Diniz in the city Patos-PB, which serves as the city of Teixeira. We collected the data registered by the descriptive type with a quantitative approach to people who have undergone laboratory tests, from 2004 to 2014. The data were analyzed according to gender, age and year. The exams researched and used for diagnosis of cases were Enzyme-Linked Immunosorbent Assay (ELISA), Indirect Hemagglutination (HAI), Immunofluorescence Indirect (RIFI) and Polymerase Chain Reaction (PCR), they were separated into positive results (25) and negative (119), totaling 144 tests recorded in the laboratory during this period of 10 years.
Another metric used was the application of a questionnaire on a set of characteristics of Chagas disease and the transmitting agent in a sample of 100 people. The questionnaire was prepared for the occasion and was composed of questions regarding the triatomine insect, place of birth, place of residence and personal characteristics. In addition, the identification of structural types of households and their occupants were also included (Silveira et al., 2009).
The choice of the participants was randomly selected in regions of urban and rural areas, different points of locations in the city of Teixeira, whose inhabitants were considered able to participate. The study included the people who were present in the home at the time of the visit of the interviewers. Undergraduate students also applied to the questionnaires. The households were visited only once. During the interviews, the questionnaires were filled, with answers provided by the respondent. The protocols of the ethics committee were respected.
The statistical analyzes of the data were performed in Microsoft computers, Windows 10, with statistical processing features of Epi Info ™ software system, version 7.1.5 (CDC, Atlanta, USA), Microsoft Excel and Microsoft Word for the production of tables and graphics.
The data presented in the course of this topic corresponds to the number of analyzes carried out in the city of Teixeira-PB, located in Paraiba hinterland. This area has similar geographical features such as climate-semiarid (hot and dry), with average high temperatures between 25°C and 30°C, climatic conditions favorable for the development of the insect vector, the triatomine.
The main objective of the numbers in which it will be presented below is to translate the percentage of all people affected by the protozoan Trypanosoma cruzi, which causes Chagas disease, and compare them with previous studies in nearby cities.
The positive and negative cases analyzed in this study had no record of the way in which the infection occurred , but it can produce an infection curve in a ten year period (Figure 3). However, it is known that the major forms of protozoa in human blood contact is through the vector, the triatomine, which is common in Teixeira region. Figure 2, are images of the insects commonly found in the study area.
Figure 2A displays images of two species of triatomine the Trypanosoma brasiliensis and Trypanosoma pseudomaculata. Figure 2B displays the species of Trypanosssoma petrochii and while Figure 2C displays the species of Panstrongilus lutzi and Panstrongilus megistus these species mentioned earlier are commonly found in the region studied.
Another factor that influences the proliferation of the T. cruzi in the population is explained by the fact that it has dozens of residences named as mud houses or brick houses that are located within the forest of caatinga and common in rural area of Teixeira.
The Ministry of Health (2009) recommends the realization of two serological tests for the diagnosis of Chagas disease, the recommended tests are the ELISA, HAI and RIFI. In the period between 2009 to 2012, the Entomology Laboratory of the city of Patos-PB performed examinations for HAI and the RIFI. From 2013, a new test for ELISA was implemented, which is used nowadays.
The data shown in Figure 3 reflect the number of cases in which it detected the T. cruzi in the blood of people who have undergone the serological examinations, between 2005 and 2014, carried out by entomological laboratory in the city of Patos-PB.
In the city of Teixeira, during the 2005 examinations, a person who has been subjected to the tests had positive result. In 2006, no case was positive in 2007, 32 people had their blood analyzed in which 15.6% of people carried the T. cruzi, while in 2008 no diagnosis of the disease was recorded. Two cases was in 2009, four cases in 2010, four in 2011, three cases in 2012, five in 2013 and just one in 2014. The rise of Chagas disease started since 2009, and a decline in 2014, because only eleven people had submitted to the examination.
The results of serological tests for Chagas disease in the cities of Paraiba hinterland, between the years 2005 to 2014 revealed that the age groups with the highest incidence of positive cases for T. cruzi are 50'58 years (Cristiany, 2015). A total of 144 people were examined in the last ten years in Teixeira, 17% (25 individuals) of those who were subjected to laboratory tests had infected blood.
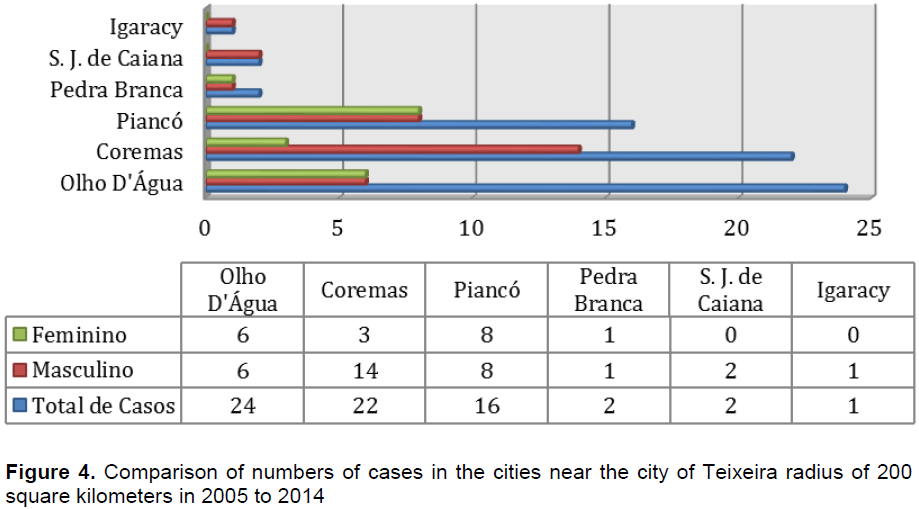
Figure 4 shows the comparison of people infected by T. cruzi in an 200 km² radius. In comparison between genders, people who had the diseases were confirmed to be 17% (16 female and 9 male). In Teixeira municipality, women showed higher rate. A feasible explanation is that women are more time exposed to vectors, since they spend more time in their homes than men or have the near wall sleep habit (Borges-pereira, 2006). Unlike other cities, it was observed that males had higher positive cases (Figure 4).
In terms of age (17%), there were no records of individuals within the age of 30 years in Teixeira city who were infected, indicating that young people had no contact with the vector or are not infected. Table 1 aims to demonstrate the level of knowledge of the people about Chagas disease. They interviewed 100 people (59 male and 41 female) with 73% of respondents living in urban areas and 27% in the countryside. Regarding the level of education, it was noted that 16% are illiterate, 77% have basic education and 7% have graduation. People were interviewed with an age range of 13 to 89 years.
A key question to extract from this research is to detect as much knowledge as possible from the population on Chagas disease. Among the respondents, 97% have heard about the disease, and 37% are aware that the disease is acquired by the bite of Triatomine contaminated by T. cruzi. This information is important because it is the population that can implement a method to prevent Chagas disease, for it is necessary that some educational and awareness practices should be put in place.
A comparison with the results of the questionnaires of Teixeira on the knowledge of the disease and the vector insect, other survey data, the population of Bambuí region in the state of Minas Gerais, revealed that both adults and children showed good knowledge about the triatomasp with accuracy rates quite satisfactory for the recognition of the insects (89.1% for adults and 66.7% for school) (Villela et al., 2009). These findings revealed that Teixeira population has very good knowledge (97%). Reason potentially explained by the high number of positive cases in the region, featuring endemic risk of T. cruzi.
Analyzing the interviews (Table 1), it was observed that 44% of respondents have found the triatomine in his residence reaching an average of three triatomine per individual. These data are highly relevant as the direct contact with the vector of the disease corresponds to the means, which transmits more Chagas disease, the triatomasp when feeding, defecates and their feces infected with T. cruzi comes in contact with the body of man (Borges-pereira, 2006). Regarding animal husbandry, 53% say they keep animals at home, 50% breeds dogs which is considered the main domestic reservoir of T. cruzi (Montenegro et al., 2002).
The Chagas disease is a disease that affects between 16 and 18 million individuals, and exposing another 90 million at risk of contracting it (Sousa et al., 2007). In the questionnaires, it was ascertained that 25% of respondents are infected with T. cruzi or someone in the family is been infected (Table 1). The data reflect that the city of Teixeira and its adjacent regions are considered as endemic areas for Chagas disease, part of the regions most at risk of vectorial transmission of Brazil.
Based on the questionnaires, it was verified that 67% of respondents did not undergo serologic tests, even those people who were infected with triatomine. Question on whether the respondents already had seen any campaign or awareness in the city of Teixeira on Chagas disease, 67% said they never witnessed campaign in the city showing the lack of knowledge of the population (Table 1).
In this study, we observed high rates of T. Cruzi in the city studied, warning of the need for effective public policies aimed at public awareness of disease transmission, improvement in living conditions in rural communities and developing effective actions to combat vector with greater attention to the most affected groups, females and people over 30 years. So arises the idea that the infection rate may increase in both sexes and affect other age groups, or continue on the rise in the region studied. Therefore, based on the data presented, it appears that there is need for more information and attention of Health Surveillance in the study area, which is essential to conduct further research to become current epidemiological data of Chagas disease, and arrangements can be made appropriate for prophylactic to combat Trypanosomacruzi.
The authors have not declared any conflict of interests.
REFERENCES
|
Abreu RL (2006). GNU Free Documentation Licesne, Mapa da Paraíba.
|
|
|
|
Borges PJ, Castro JAF, Silva AR, Zauza PL, Bulhões TP, Gonçalves ME, Almeida ES,Salmito MA, Pereira LRM, Alves Filho FI, Correia-Lima FG, Coura JR (2006). Soroprevalência da infecção chagásica no Estado do Piauí. Rev. Soc. Bras. Med. Trop. 39:530-539.
Crossref
|
|
|
|
|
Dias JCP, Coura JR (1997). Epidemiologia. In: Dias JCP, Coura JR (ed.), Clínica e Terapêutica da Doença de Chagas: Uma Abordagem Prática para o Clínico Geral. Editora Fiocruz, Rio de Janeiro. pp. 33-66.
|
|
|
|
|
Dias ELF (2009). Qualidade de Vida de Adultos e Idosos Portadores da Doença de Chagas.74 fls. Dissertação(Gerontologia). Universidade Estadual de Campinas (UNICAMP).
|
|
|
|
|
Lima AFR (2010). Análise sócio-ambiental da dinâmica da doença de chagas no estado de Sergipe/Brasil. Dissertação de mestrado (saúde e ambiente). Universidade Tiradentes.
|
|
|
|
|
Mangueira VM (2013). Avaliação Soroepidemiológica da Doença de Chagas no Cariri Paraibano. 40 fls. Monografia (Farmácia). Universidade Federal da Paraíba (UFPB).
|
|
|
|
|
Montenegro VM, Jiménez M, Dias JCP, Zeledón R (2002). Chagas disease in dogs from endemic áreas of Costa Rica. Mem. Inst. Oswaldo Cruz 97(4):491-494.
Crossref
|
|
|
|
|
Neves PD (2005). Parasitologia Humana. 11. Ed. São Paulo: Atheneu.
|
|
|
|
|
Rodrigues CA (2015). Prevalência da Doença de Chagas na Microrregião do Vale do Piancó, Paraíba, Brasil. Monografia (Ciências Biológicas). Universidade Federal da Paraíba (UFCG).
|
|
|
|
|
Silveira AC, Rezende DF, Nogales AM, Cortez-Escalante JJ, Castro C, Macêdo V (2009). Assessment of an Entomological Surveillance System for Chagas Disease with Community Participation in Mambaí and Buritinópolis, State of Goiás. Goiás.
|
|
|
|
|
Sousa JO, Nogueira RBS, Silva LGS, Costa DL, Amorim FDB, Marinho AH, Barbosa TM, Onofre LB, Alencar VMPD, Lima CMBL (2007). Análise dos Casos Confirmados de Doença de Chagas na Paraíba em 2007. XI Encontro de Iniciação à Docência. View
|
|
|
|
|
Villela MM, Pimenta DN, Lamounier PA, Dias JC (2009). Evaluation of Knowledge and Practices Related to Chagas Disease and its Vectors Among Adults and Children in an Endemic Region in Minas Gerais State, Brazil. Cad. Saude Publica 25(8):1701-1710.
|
|
|
|
|
Teixeira A, Viinaud M, Castro AM (2011). Emerging Chagas Disease. Brasília, Bentham Science Publishers.
View
|
|








