Review

ABSTRACT
Human African Trypanosomiasis (HAT) due to Trypanosoma brucei gambiense remains a major public health problem in South Sudan. It causes substantial socio-economic impacts on the livelihoods of poor rural inhabitants. This article throws lights on a review of historic and current trends for evolution of HAT in South Sudan. Data of HAT cases were obtained from several relevant sources including World Health Organization (WHO) disease reports as of 1956-2018. Hence, HAT episodes were divided into four historical periods: The First Civil War (1955-1972); the post-Addis Ababa Accord (1973-1982); the Second Civil War (1983-2004); and the post-Comprehensive Peace Agreement (CPA) as of 2005-2018. The highest HAT cases of 16,539 (52.3%) occurred during the Second Civil War, followed by 7,708(24.37%) in post Addis Ababa Accord; 5,164(16.33%) in post-CPA, and 2,215(7.0%) during the First Civil War totaling 31,626 cases. The lowest prevalence of HAT as of the 1950s through 1960s might be due to application of effective intervention and control measures. The highest prevalence rate during the Second Civil War could be ascribed to political upheavals, instability and civil unrest. Currently, no HAT cases were reported from Akobo and Pachalla foci in Jonglei State. All the historic foci of HAT in South Sudan are still active with exception of Raga in Western Bahr El-Ghazal State. Further studies on molecular parasitology and epidemiology are needed to re-establish the endemic status of Raga, Akobo and Pachalla HAT foci.
Key words: Human African Trypanosomiasis (HAT), past history, new foci, current trends, South Sudan.
INTRODUCTION
Human African Trypanosomiasis (HAT) or known as sleeping sickness is one of the neglected tsetse fly transmitted tropical diseases found in remote rural areas in Sub-Saharan Africa (Simarro et al., 2010). It is a deadly disease with fatality rate of 100% in untreated cases (WHO Fact Sheet No.259, 2012).
In 2000, WHO reported a total of 55 million people were at risk of the disease in 36 countries of sub-Saharan Africa with approximately 250 foci. However, only 3 to 4 million people were exposed to surveillance (Welburn and Maudlin,1999). Moreover, WHO reported that the actual annual number of cases might be in the range of 300,000 to 500,000. The disease was estimated to cause a loss of 2.1 million disability-adjusted life years in 1999. WHO has prioritized the elimination or eradication of African trypanosomiasis by 2020. Introduction of strengthened control and surveillance activities over the past twenty years succeeded in progressively reducing disease transmission (Franco et al., 2020).
Novel initiatives to combat Animal African Trypanosomiasis (AAT) and HAT were formulated into the Programme against African Trypanosomosis (PAAT) and the Pan African Tsetse and Trypanosomiasis Eradication Campaign (PATTEC). Consequently, HAT cases have halved in less than a decade in areas where it is still a public problem (Franco et al., 2017). Progress made in the control of HAT in many endemic countries had led to a reduction in the number of cases to 10,000 in 2009 for the first time in 50 years. This trend has been sustained in 2010 with 7,139 new cases (WHO, Fact sheet No 259, 2012). As of 2010, incidences of HAT were reported to decline to over 500 new cases in the DRC per annum compared to Angola, CAR, Chad, South Sudan and Uganda with a range of 100 and 500 new cases per annum. Furthermore, other HAT affected countries were reported to have fewer than 100 new cases per annum. However, current estimates indicated an annual incidence of 50,000 to 70,000 cases (WHO, Factsheet No 259, 2012).
HAT due to Trypanosoma brucei gambiense poses an important public health problem in South Sudan. The first case of sleeping sickness due T. b. gambiense in South Sudan was reported in 1908. Over 3,000 cases were documented between 1920 and 1925 (Ruiz-Postigo et al., 2012).
In South Sudan, the disease is confined only in the three Greater Equatoria States bordering Uganda, DRC and CAR. This is mainly due to the presence of the efficient tsetse vector Glossina fuscipes fuscipes (Mohammed et al., 2008). Among many other factors, devastating civil wars together with population displacement, poor health facilities and insecurity situation have culminated in massive HAT resurgence in the Greater Equatoria States (Moore et al., 1999). HAT could be diagnosed by direct microscopy and serology, and the control strategy is mainly based on chemotherapy. Apart from Lateral Flow Test (Enyaru et al., 2014), Indirect Fluorescent Antibody Test (Bailey et al., 1967), Enzyme-linked Immuno- sorbent Assay (ELISA), Card Agglutination Trypanosomes Test (CATT) and HAT rapid diagnostic tests (RDTs) have been employed for detection of trypanosomosis (Ruiz-Postigo et al., 2012; Sumbria et al., 2017).
Moreover, molecular techniques for detection of trypanosome parasites in wild tsetse flies were used in Cameroon (Morlais et al., 1998), Uganda (Alibu et al., 2015) and South Sudan (Lukaw et al., 2015). The Loop-mediated isothermal Amplification (LAMP) and PCR- based tests are crucial for surveillance and monitoring trypanosomosis (Malele et al., 2013; Parashar et al., 2018). Such tests could be employed for identification of infection not detected microscopically (Morlais et al., 1998; Diallo et al., 2018) and differentiation of trypanosomes which are morphologically indistinguishable, but with a very different economic impact (Duvallet et al., 1999). WHO has prioritized the elimination or eradication of African trypanosomiasis by 2020 (Franco et al., 2020).
South Sudan is a newly born country that is still at its building stage. Health infrastructure is still being built. Beside infrastructure, information on HAT cases and trends may be needed to justify carrying out HAT interventions and control strategy. Some of these strategies need to understand how HAT epidemiology developed in the course of years. The control strategy should also understand and be able to spot HAT Foci both the present and the past. Not only this, it should be able to underscore the reasons as to why new HAT Foci developed on the account of the already existing past foci.
The paper sheds lights on the distribution of HAT cases in 1955-2018, in South Sudan. Due to the epidemiological trends of HAT and in the context of elimination strategy, this approach of review adopted in this paper will provide a useful information that might be applied to analyze the present HAT cases and explain the factors that made most historic HAT foci active in the present day. There are four periods of time that the review considered in this study. Each one of these periods provides information on cumulative HAT cases and the problems associated with the emergence of HAT cases and outbreaks in the associating HAT foci. The purpose of this article was to reveal a review and analysis of historic and current trends of HAT and to highlight on the factors that led to outbreaks of HAT in the renowned HAT foci in South Sudan.
DATA SOURCES AND ANALYSIS
Extensive literature on the HAT Statistic by country in the WHO Reports was consulted. Statistic on the HAT cases in South Sudan as of 1955- 2018 was obtained from several WHO reports. The data obtained were divided into four periods. These include the First Civil War (1955-1972), the post Addis Ababa Accord (1973-1982), the Second Civil War (1983-2004) and the post-Comprehensive Peace Agreement (CPA) as of 2005-2018. Each period reflects an era of the political history of South Sudan. Data were managed and entered into Microsoft Excel sheet and used to generate a chart showing the total number of HAT cases in each period.
Shape file for the ten States of South Sudan was obtained from the South Sudan National Bureau of Statistics (SSNBS).The file and ArcGIS 3.5 software were used to create a map of the current and the past HAT foci in South Sudan.
HISTORIC AND CURRENT TRENDS OF HAT
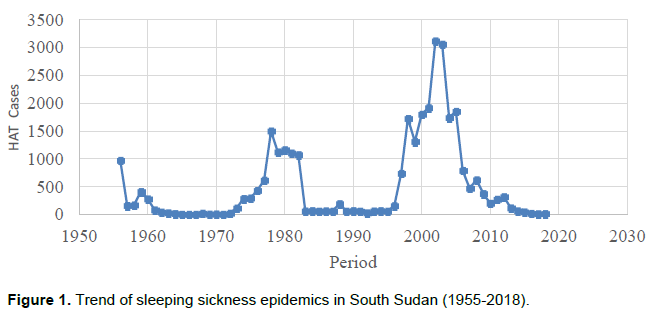
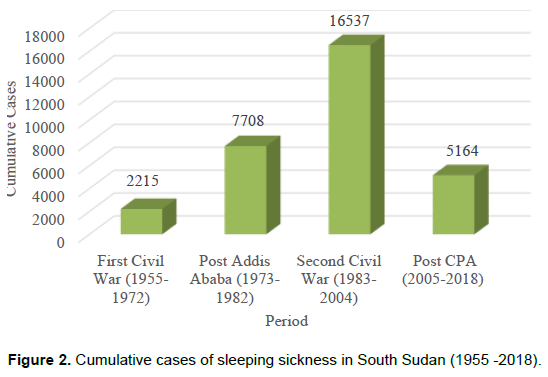
Figure 1 shows the trends of sleeping sickness cases for over six decades as of 1955-2018, of which three peaks of HAT outbreaks occurred in South Sudan. The eminent South Sudan’s HAT recent epidemic occurred during the Second Civil War period (1983-2004). Figure 2 shows the cumulative and total number of sleeping sickness cases in South Sudan for over six decades as of 1955-2018. The highest number of 16,537(52.3%) cases was revealed during the Second Civil War (1983-2004) compared to 7,708 (24.37%); 5,164 (16.33%); and 2,215(7.0%) cases during the Post Addis Ababa Accord (1973-1982); the CPA (2005-2018) and the First Civil War (1955-1972), respectively.
DISCUSSION
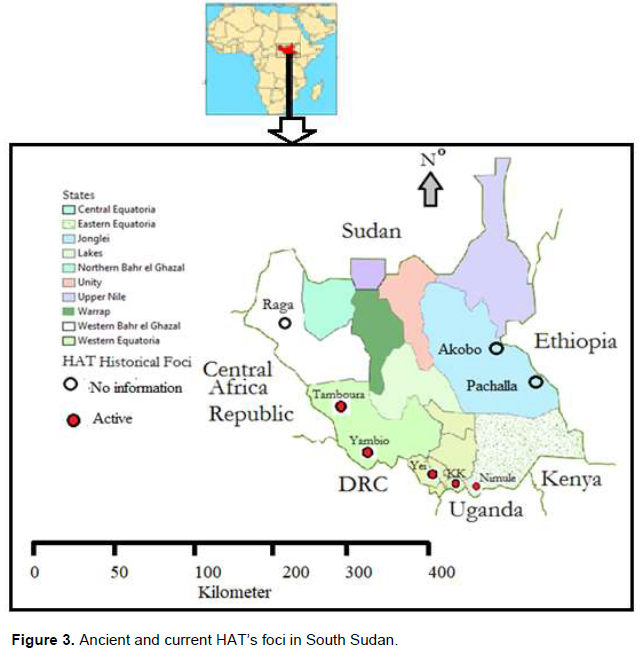
HAT outbreak in East African region is associated with specific foci (Hide, 1999). These foci are considered potential areas where the risk of infection with the disease and disease transmission may be high (Figure 3). Moreover, HAT foci expanded and contracted over time as tsetse fly distribution and human activities changed (Welburn and Maudlin, 1999). Human activities and the factors affecting vector distribution over time might give an insight into the characteristics of HAT foci. Therefore, disease outbreak at foci, necessitates a transmission cycle by efficient tsetse fly and suitable habitats that support the fly population and the presence of mammalian hosts. In South Sudan active HAT foci due to T. b. gambiense have been described in the Greater Equatoria region bordering the CAR, the DRC, and Uganda; whereas, the HAT caused by T. b. rhodesiense was reported from Akobo County of Jonglei State bordering Gambella in Ethiopia, although since 1984 no cases were reported (Ruiz-Postigo et al., 2012) despite the presence of G. f. fuscipes and G. tachinoides.
Repeated epidemics of HAT due to T. b. gambiense in South Sudan were observed periodically in foci found within a belt bordering the CAR, the DRC and Uganda (Moore and Richer, 2001). One of the most important episodes of HAT outbreaks in 1950s in the South Sudan occurred when Yambio in Western Equatoria State was designated as the centre of the New Zande Development Scheme (NZDS) in 1946. This event was one of the unique situations in Africa in which agricultural developments triggered massive population movement.
People moved and settled in high density in the Centre of the NZDS where many G. palpalis infested streams and HAT active foci present. The surrounding HAT-epidemic villages created conditions favorable for HAT in urban areas (Simo et al., 2006).
Following the signing of the Addis Ababa Peace Accord in 1972, the repatriation of South Sudanese refugees from endemic HAT areas of Uganda to South Sudan and the massive movements of the internally displaced Ugandan citizens to Nimule might be the cause of HAT outbreak in Nimule in 1970s (Palmer et al., 2014). Resurgence of HAT in 1970’s in the former Western and Eastern Equatoria Provinces had prompted an intervention for control programme by bilateral Belgian Sudanese Trypanosomiasis programme (BSTP). Between 1974 and 1978 HAT control activities were maintained through external assistance from WHO and BSTP. Hence, a reduction in the cases of HAT revealed in the mids-1980, both Li-Rangu and Juba Teaching Hospitals became reference centers for HAT, but later on it deteriorated due to eruption of the second civil war in 1983 (Ruiz-Postigo et al., 2012).
In the late 1980’sand 1990’s HAT control programmes and activities had collapsed. Consequently, by 1997 HAT re-emerged with prevalence rates as high as 19% in South-western Communities of South Sudan bordering DRC (Ford, 2007). By 1990, 4 out of 5 health facilities in the country were shut (Palmer et al., 2014).Consequently, HAT outbreaks occurred in the HAT already known foci in the South-western part of the county bordering CAR and DRC (Moore et al., 1999). Furthermore, HAT resurgence surfaced as renown epidemic in the Southern Sudan in 1997 (Hide, 1999).
Subsequent to the signing of the CPA in 2005, a relative peace and stability prevailed in South Sudan where HAT control activities carried out by the Ministry of Health (MoH) and Non-governmental Organizations (NGOs). The MoH and the NGOs planned control activities and as a result there was a significant decrease in number of reporting cases (Ruiz-Postigo et al., 2012).
In post-CPA era, the NGOs that were instrumental in HAT control programme withdrew leading to increasing HAT cases between the years 2000 and 2010. This was due to cessation of HAT control activities and reduction of health facilities after 2006 (Ruiz-Postigo et al., 2012).
Currently, the low HAT cases in South Sudan do not suggest that HAT foci do not exist. All the HAT ancient foci in Yambio and Tambura Counties in Western Equatoria State, Yei River and Morobo Counties in Central Equatoria State, Torit and Magwi Counties as well as Nimule Payam of Eastern Equatoria State may be active. No reported cases of HAT from the Raga historic foci in the Raga County of Western Bahr El Ghazal State were realized. This might be attributed to numerous factors including ecological factors and vegetation cover. HAT high risk correlates with areas of high infection, and so do areas of low risk with low infection. High risk also occurs in areas with low population densities, and low risk is also found in areas with high population densities (Ford et al., 2006). Disease risk is high in population with low density due to higher fly-host contact ratios; whereas the risk is low in dense population due to low fly-host contact ratios. There is a high disease risk when a new population moves into a population with high infection.
Social conflicts play a role in infectious diseases outbreaks and have long been recognized as determinants of infectious disease risk. The close association between the temporal occurrences of HAT outbreaks and civil conflicts is not a new scenario in South Sudan. There is an association between conflict and infectious disease, especially in the foci where civil conflicts still persist (Ford, 2007). The temporal occurrences of outbreaks for both T. b. rhodesiense and T. b. gambiense sub-species are associated with times of conflicts in south eastern Uganda (Ford, 2007). All of the HAT epidemics and outbreaks in South Sudan were observed during the era of political upheavals, instability and civil disturbance (Duku, 1979). With the eruption of the first civil war in the Sudan, enormous and unceasing population dislodgment across the country occurred. The movement of population to the regions where HAT foci prevailed and repatriated back to their homeland could explain HAT outbreaks and expansion of the local HAT reservoir. Proliferation of the HAT in Uganda was attributed to refugee movements and interaction with infected regions of the southern Sudan (Ford et al., 2006). Repatriation of the refugees had eventually increased HAT transmission potential in two ways: first the refugees from the endemic foci might pose the risk of infection to the few natives who did not leave their home land during the long years of conflict, secondly the vegetation and the new tsetse fly habitat that had grown during their absence became a potential risk since they might have made the environment suitable for tsetse fly (Ford, 2007). The later scenario increased HAT transmission potential by affecting directly a number of parameters in the HAT transmission leading to the increasing of HAT transmission potential (Ford, 2007); this might have contributed in the HAT cases in 1970’s.
CONCLUSION
The current review indicates that previously infected known Gambian HAT foci may still be active and can pose infection risk in South Sudan. Only Raga HAT historic foci remain without infection. No new cases of Rhodesian HAT are reported in South Sudan, though cattle are imported from Uganda which could warrant precautionary measures. Further studies on molecular parasitology and epidemiology are needed to confirm the elimination of infection or re-establish the endemic status of Raga, Akobo and Pachalla HAT foci in South Sudan.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Alibu VP, Enyaru JCK, Matovu E, Malele II, Chisi JE, Mbongo N, Mansinsa P, El-Rayah I, Yassir M, Abdelrahman M, Ochi EB, Lukaw YS(2015). Molecular xeno monitoring of trypanosomes in tsetse flies. Journal of Parasitology and Vector Biology 7(6):80-88. |
|
|
Bailey NM, Cunningham MP, Kimber CD (1967). The indirect fluorescent antibody technique applied to dried blood, for use as a screening test in the diagnosis of human trypanosomiasis in Africa. Transactions of the Royal Society of Tropical Medicine and Hygiene 61:696-700. |
|
|
Diallo T, Singla LD, Sumbria D, Kaur P, Bal MS (2018). Conventional and molecular diagnosis of haemo-protozoan infections in Cattle and equids from Republic of Guinea and India. Indian Journal of Animal Research 52(8):1206-1211. |
|
|
Duku MO (1979). Human trypanosomiasis in the Southern Sudan: Present situation and control measures in: International Scientific Council for Trypanosomiasis Research and Control 16th Meeting, Yaoundé Cameroon, pp. 139-145. |
|
|
Duvallet G, de La Rocque S, Reifenberg JM, Solano P, Lefrançois T, Michel JF, Bengaly Z, Sidibe I, Cuisance D,Cuny G (1999). Review on the molecular tools for the understanding of the epidemiology of animal trypanosomosis in West Africa. Mem Inst Oswaldo Cruz, Rio de Janeiro 94(2):245-248. |
|
|
Enyaru CKJ, James N, Pius AV, Enock M, Malele II, John CE, Nicolas M, Philemon M, El-Rayah I, Yassir M, Mubarak M, Ochi E, Vinand N (2014). Development and evaluation of lateral flow test for the detection of trypanosomes in tsetse flies. Journal of Parasitology and Vector Biology 6(12):181-188. |
|
|
Ford LB (2007). Civil conflict and sleeping sickness in Africa in general and Uganda in particular. Conflict and Health 1:6e. |
|
|
Ford LB, Odiit M, Maiso F, Waltner-Toews D, McDermott J(2006). Sleeping sickness in Uganda: revisiting current and historical distributions. African Health Sciences 6(4):223-231. |
|
|
Franco JR, Cecchi G, Priotto G, Paone M, Diarra A, Grout L, Simarro PP, Zhao W, Argaw D (2020). Monitoring the elimination of human African trypanosomiasis at continental and country level: Update to 2018. PLoS Neglected Tropical Diseases 14(5):e0008261 |
|
|
Franco JR, Cecchi G, Priotto G, Paone M, Diarra A, Grout L, Mattioli RC, Argaw D (2017). Monitoring the elimination of human African trypanosomiasis: Update to 2014. PLoS Neglected Tropical Diseases 11(5):e0005585. |
|
|
Hide G (1999). History of Sleeping Sickness in East Africa. Clinical Microbiology Reviews 12(1):112-125. |
|
|
Lukaw YS, Abdelrahman MM, Mohammed YO, Ochi EB, Suliman YR, El-Rayah IE (2015).Performance assessment of molecular and microscopy tests for detection of Trypanosoma species in Glossina fuscipes fuscipes (Diptera: Glossinidae) midguts in Kajo-keji County, South Sudan. International Journal of Bioassays 4(5):3910-3914. |
|
|
Malele I, Ouma J, Enyarau JCK, MatovuE, AlibuV, Auma JE, Onyoyo SG, Mukiria PW, Ndungu K, Kitonga PK, Mwaniki LM, Nyingili HS, Lyarau EA, Kapange LA, Kamau PK, Masiga DK(2013). Comparative diagnostic and analytical performance of PCR and LAMP-based trypanosome detection methods estimated using pooled whole tsetse flies midguts. Veterinary Parasitology 197:549-556. |
|
|
Mohammed YO, Mohammed- Ahmed MM, Malik KH, Rayah IE (2008). Distribution pattern of Glossina fuscipes fuscipes in Bahr el Jebel State, southern Sudan. International Journal of Tropical Insect Science 27:210-215. |
|
|
Moore A, Richer M (2001). Re-emergence of epidemic sleeping sickness in southern Sudan. Tropical Medicine and International Health. 6(5): 342-347. |
|
|
Moore A, Richer M, Enrile M, Losio E, Roberts J (1999). Resurgence of sleeping sickness in Tambura County, Sudan. American Journal of Tropical Medicine and Hygiene 61:315-318. |
|
|
Morlais I, Grebaut P, Bodo JM, Djoha S, Cuny G, Herder S (1998). Detection and identification of trypanosomes by polymerase chain reaction in wild tsetse flies in Cameroon. Acta Tropica 70:109-117. |
|
|
Palmer JJ, Kelly AH, Surur EI, Checchi F, Jones C (2014). Changing landscapes, changing practice: Negotiating access to sleeping sickness services in a post-conflict society. Social Science and Medicine 120:396-404. |
|
|
Parashar R, Singla LD, Batra K, Kumar R, Kashyap N, Kaur P and Bal MS (2018). Unraveling cryptic epizootiology of equid trypanosomosis in Punjab State of India by parasitological and sero-molecular techniques. Acta Tropica 185:18-26. |
|
|
Ruiz-Postigo JA, Franco JR, Lado M, Simarro PP (2012). Human african trypanosomiasis in South Sudan: How can we prevent a new epidemic? PLoS Neglected Tropical Diseases 6(5):e1541. |
|
|
Simarro PP, Cecci G, Poane M, Franco JR, Diarra A, Ruiz JA, Fèvre EM, Courtin F, Mattioli RC, Jannin JG (2010). The Atlas of human African trypanosomiasis: A contribution to global mapping of neglected tropical diseases. International Journal of Health Geographics 9:57. |
|
|
Simo G, Mansinsa PD, KandeV, Mesu BK, Manzambi EZ, Ollivier G, Asonganyi T, Cuny G, Grébaut P (2006). Trypanosomiasis transmission, Kinshasa, Democratic Republic of the Congo. Emerging Infectious Diseases. |
|
|
Sumbria D, Singla LD, Kumar R, Bal MS, Kaur P (2017). Comparative sero-prevalence and risk factor analysis of Trypanosoma evansi infection in equines from different agro-climatic zones of Punjab (India) by indirect enzyme linked immunosorbent assay and card agglutination test/T. evansi. Review of Scientific and Technical OIE 36(3):971-979. |
|
|
Welburn SC, Maudlin I (1999). Tsetse-trypanosome interactions: rites of passage. Parasitology Today 15:399-403. |
|
|
WHO (2012). World Health Organization (WHO) Fact Sheet No.259. Tryapanosomiasis, Human African (Sleeping Sickness). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


