Full Length Research Paper

ABSTRACT
A study was conducted among 108 students and pupils of four selected schools in Umukabia Community in Ehime Mbano local government area of Imo State, Nigeria using their activities at Efuru and Okparadibia streams. Structured questionnaire was used to elicit information on water contact frequency and aetiology of the disease. Schistosoma haematobium ova detection was achieved by the microscopy. Results revealed that there was no significant difference in prevalence of S. haematobium between the students and pupils of the schools but there was a significant difference in prevalence of the infection among the males and females. It is therefore recommended that boreholes should be sunk in the community, the streams be treated with mullucides to reduce the snail population, and recreational facilities be provided in schools to dissuade children from going to play in infected streams. Finally, health awareness seminar should be intensified to create awareness of the mode of transmission of the parasite.
Key words: Schistosomiasis, water contact, mullucides.
INTRODUCTION
Schistosomiasis is one of the neglected tropical diseases in Nigeria, which continues to plagues inhabitants of rural and peri- urban areas where there is inadequate sanitation and poverty. Over 600million people worldwide are exposed to the risk of infection, especially those who perform daily water- related activities in snail infested water bodies (Etim et al., 2012). Urinary schistosomiasis is a chronic disease caused by digenetic trematode, Schistosoma haematobium. (Akinboye et al., 2012). The snail intermediate host is an aquatic plunomate belonging to the family planorbidae (Ukoli, 1990).
S. haematobium was originally a disease of Africa which has spread to other continents with the advent of the massive exodus of slaves in the 17th and 18th centuries. S. haematobium is endemic in fifty-four countries of Africa and Middle East (WHO, 1993). The occupation of people predominantly affected by S.haematobium are farming and fishing. This is further compounded by the poor sanitary conditions allied to practices as urinating in ponds, rivers and streams, which are used as population’s water supply and water- related activities like swimming, sand digging, washing of house-hold chores, bathing amongst others (Iwuet al., 2006a).
The transmission of urinary schistosomiasis is contingent to the presence of the infected snail host in water or by direct contact with human population. The distribution is focal, and its effects are more felt in the rural areas of the tropics where the population lives in natural fresh water habitats using the water for domestic water supply and agriculture (Iwu et al., 2006b).
The disease is also associated with water resource developmental projects like irrigation schemes, slow- flowing or stagnant water where the inter mediate host breeds. These results in infection of people who use the traditional methods such as wading in the water, vegetable cultivation at river banks during dry season, plant and harvest rice or catching fish as a recreational activity. In the studies carried out independently by Ofoezie (2002), Hunter (2003) and Simon and Benhamou (2009) that there were increased rates of infection due to exposure patterns associated with bathing or washing, farming along rivers and canals harboring infected snail hosts. People become infected with S. haematobium when the cercaria, which is the infective form of the parasite, penetrates the skin and enters the circulatory system after becoming paired in the various vessels, reaches the veins of the bladder and are referred to as “copula”. Parasites can lay their eggs up to five years (Newport and Agbabian, 1990). The eggs are excreted in the urine of infected persons, into water bodies and develops into a ciliated miracidia, which swims in water and penetrates the snail, developing into cercaria form. This new form can emerge from snails and penetrate in the human’s skin starting a new cycle (Chessburgh, 1987).
Many school aged children often stop by streams to swim or “cool off”, fish or wash their dirty chores, thus the study aims at examining the effect of water contact frequency on the prevalence of urinary schistosomiasis and infectivity in streams in Umukabia Community of Ehime Mbano LGA. The target respondents in schools are located at varying distances from the streams which determine the frequency of contact, students had with the stream.
METHODOLOGY
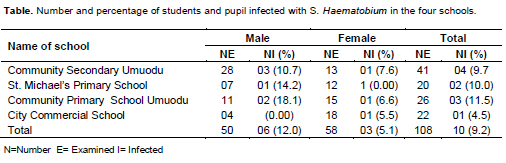
The study was conducted from January to November, 2012. Students from two secondary schools and two primary schools in Umukabia formed the study population. The Efuru stream is located along Mgboroko and Umualunwoke village while Okparadibia stream is in Umuobi both in Umukabia. The streams were selected due to their varying degree of accessibility to students and pupils of the four schools in the study. A total of 108 urine samples were collected from the students/pupils of the four schools as follows: 45 urine samples (28 males and 13 females) from Community Secondary school Umukabia, 19 urine samples from St. Michaels’ primary school Umuezeala( 7 males and 12 females), 26 urine samples from Community Primary school Umuodu (11 males and 15 females) and 22 urine samples from City Commercial Secondary School (4 males and 18 females).
Urine sampling
Urine samples were collected using 15 ml sterile sampling bottles covered with lids. This was done between 10.00 am and 1.00 pm a time reported to produce maximum egg output (Pugh and Gilles, 1978). Also, a structured questionnaire was administered to each subject to elicit information on the aetiology of the disease.
Schistosoma haematobium ova detection by microscopy
10 ml of each of the urine sample was centrifuged at 3000 r.p.m for 5 min. The supernatant was decanted, while the sediment was spread on a slide and covered with a cover slip, after which it was examined under the microscope, using the ×10 eye piece and ×40 objectives for the presence of S.haematobium ova. The quantity of eggs found were determined and expressed as number of eggs per 10 ml of urine (egg/10 ml). The infection was designated low, if the egg count was less than or equal to 50 eggs/10 ml (WHO, 1993).
RESULTS
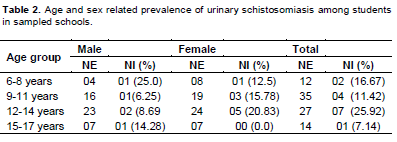
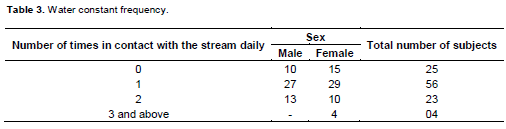
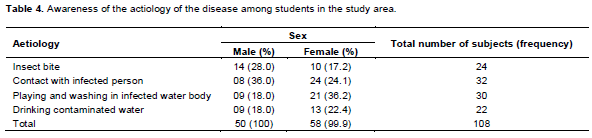
A total of 108 people were examined, comprising of 50 males and 58 females. Out of which 6 (12.0%) males and 3 (5.1%) females were found to be positive for ova of S. haematobium (Table 1). Prevalence of S. haematobium was higher among 6 to 8 years old in males and 12 to 14 years old in females (Table 2). Table 3 shows that females visit the streams more frequently than the males. The questionnaire analysis revealed that some females and males knew that playing and washing in infected water bodies was the cause of the infection depicting 36.2% and 18.0% respectively. Other sources of the infection suggested include insect bite, contact with infected person and/or drinking contaminated water meaning that the aetiology of the disease varied among the subjects (Table 4).
DISCUSSION
The overall prevalence rate of 9.2% of urinary schistosomiasis discovered in the study is low when compared to 91% prevalence observed by Gilles et al. (1965) in Ibadan, and 90 to 100% prevalence rate reported by Edungbola (1980) in Ilorin, Kwara State, Nigeria showing a variation in prevalence of schistosomiasis from one locale to another. Also, 37.82% prevalence rate was observed among primary school children in Ikwo, Ebonyi state (Iwu et al., 2006a, b), and 52.2% in Sokoto (Bello et al., 2003).
However, the current prevalence rate of 9.2% observed in the present study is higher than the 7% prevalence rate observed in Ibadan by Akinkugbe (1962), or 2.8 and 1.5% in Aguata and Imo state respectively by Ukpai and Ezeike (2002), Nnoruka (2000). The low prevalence rate might be related to continuous dredging of the streams, and improved knowledge and awareness about the disease.
Sex and age related prevalence showed that more of the males within the age range of 6 to 8 years play more often in streams than their female counterparts. Among the females age group, 12 to 14 year old was more infected than others, this is similar to the findings among secondary school students in Ibadan by Akinboye et al. (2012), and school children in Malumfanshi (Pugh and Gilles, 1978). The decline observed among the females within 15 to 17 years was previously observed by Lwanbo (1988), and was attributed to their knowledge of the aetiology of the infection and their ability to take appropriate precaution to avoid contamination. Also observed in this study, was that more females tend to visit water bodies once a day either to wash their body or chores thereby infecting themselves. This is in line with the previous reports in Ikwo, Ebonyi State where more females frequent streams to process breadfruit, fetching water for domestic use, wash cloths amongst others than their male counterparts as reported by Iwu et al. (2009), but differs from results obtained by Ukpai and Ezeike (2002), Dunah and Bristone (2000), Akogun and Akogun (1996) and Guyral and Vaz (2000) where frequency of water contact activities had been found to be positively associated with both prevalent and intensity of urinary schistosomiasis.
CONCLUSION AND RECOMMENDATION
The study revealed a low prevalence of urinary schistosomiasis, however there is need to enhance health education programs among school children, who are ignorant about the mode of transmission despite their knowledge of the disease. Also, most of the subjects encountered in the study did not know much about the life cycle, and how their activities in the environment enhance the life cycle of the parasite. There is an urgent need to treat Efuru and Okparadibia streams with effective mulluscide to reduce the snail population which is the intermediate host of the parasite. Finally, the primary schools located close to the stream should be provided with recreational facilities to dissuade children from going to play in infected streams.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
| Akinboye DO, Ajisebutu JU, Fawole O, Agbolade OM, Akinboye OO, Amosu AM, Atulomah NOS, Awodele O, Odula, O, Owodunni BM, Rebecca SN, Falade M, Emem O (2012). Urinary schistosomiasis; water contact frequency and infectivity among secondary school students in Ibadan, Nigeria. Nigerian J. Parasitol. 32(1):129-134. | ||||
| Akinkugbe OO (1962). Urinary schistosomiasis in Ibadan school children. West Afr. Med. J. 11:124-127. | ||||
| Akogun OB, Akogun MK (1996).Human Behavior, Water usages and Schistosomiasis Transmission in a small settlement near Yola. Nigerian. Ann. Trop. Med. Parasitol. 90(3):302–311. | ||||
| Bello YM, Adamu T, Abubakar U, Mohammed AA (2003). Urinary schistomiasis in some villages among the Goronyo Dam, Sokoto State, Nigeria. Nigerian J. Parasitol. 24:109-114. | ||||
| Chessburgh M (1987). Medical laboratory manual for tropical countries 2nd edition E.L.B.S. London 323-341. | ||||
| Dunah CS, Bristone B (2000). The prevalence of Schistosoma heamatobium among primary School pupils in Majo-belwe L.G.A of Anambra State Nigerian The J. Parasitol. 21:15-20. | ||||
| Edungbola D (1980). Water utilization and its health implication in Illorin, Kwara State, Nigeria. Acts Tropica 30:417-422. | ||||
| Etim SE, Okon OE, Oku EE, Ekpong GI, Ohioma ME, Uttah CE (2012). Urinary schistosomiasis in a rice farming community in Biase Area of cross River state for Nigeria. Nigerian J. Parasitol. 33(2):197-201 | ||||
|
Gilles HM, Lucas A, Adeniyi Jones C, Linder R, Avand A (1965). Schistosoma heamatobium infection in Nigeria II; infection of primary and secondary schools in ibadan. Ann. Trop. Med. Parasitol. 59(4):441-450. Pubmed |
||||
| Guyral, Vaz RG (2000). Prevalence, Risk Behavior and level of information on Urinary Schistosomiasis in primary school students from the Primeiro Yunho Health District, Maputo Mocanbique Cad. Sande Publican 16(1):43 -50. | ||||
|
Hunter JM (2003). Inherited burden of disease: Agricultural dams and the persistence of bloody urine (S. Haematobium) in the upper east region of Ghana. 1957-1997. Soc. Sci. Med. 56(2):219-234 crossref |
||||
| Iwu RU, Nwoke BEB, Anosike JC (2006). Prevalence of Urinary Schistosomiasis among Primary School children in Ikwo LGA,Ebonyi State, Nigeria. Interworld J. Sci. Technol. 3(1):80–85. | ||||
| Iwu RU, Anosike JC, Nwoke BEB (2006). Sociocultural and behavioral issues in the Prevention and Treatment of UrinarySchistosomiasis. Inter- World J. Sci. Technol. 3(2):97-101. | ||||
| Iwu RU, Nwoke BEB, Anosike JC (2009).Endemicity of Urinary Schistosomiasis in Ohaukwu Local Government Area of Ebonyi State, Nigeria. Interworld J. Sci. Technol. 3(1):400–407. | ||||
|
Lwanbo NJS (1988). Transmission of Urinary Schistosomiasis in Sukuma land Tanzania. J. Helminthol. 62(3):213-217. crossref |
||||
| Newport GR, Agbabian N (1990). Molecular biology of schistosomes and filariae in modern parasitic biology; cellular immunological and molecular aspects, Wyler D.J (ed) New York, freeman and company . 362. | ||||
| Nnoruka VO (2000). Epidemiological studies of urinary Schistosomiasis in Imo state I. Rapid Assessment. Nigerian The J. Parasitol. 21:21-32. | ||||
|
Ofoezie IE (2002). Human Health and sustainable water resource development in Nigeria; schistosomiasis in artificial lakes. Nat. resources forum 26:150-160. crossref |
||||
|
Pugh RNH, Gilles (1978). Malumfashi Endemic diseases research project, III urinary schistosomiasis; a congitudinal study. Ann. Trop. Med. Parasit. 72:471-482 Pubmed |
||||
| Simon D, Benhamou JF (2009). Rice farming in Guinea-forestiere; outcome of a development project. Field Active Science Report 2(1) | ||||
| WHO (1993). The control of schistosomiasis. Second report of a World Health organization expert committee, technical report series No 830, WHO Genera, Switzerland. 86. | ||||
| Ukoli FMA (1990). Introduction to parasitology in tropical Africa. Textflow ltd. 52-72. | ||||
| Ukpai OM, Ezeike AC (2002). The prevalence of urinary schistosomiasis among primary school children in Aguata L.G.A Anambra state, Nigeria. The J. Parasitol. 23:139-144. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


