Short Communication
ABSTRACT
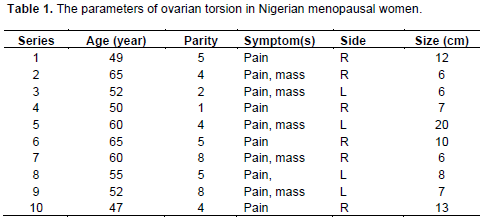
This study aimed at determining the prevalence of ovarian torsion in postmenopausal women in Nigeria. For this purpose, a histopathology data pool was maintained for 30 years among the Igbos, a large ethnic group in Nigeria from where postmenopausal women diagnosed with ovarian torsion were extracted for classification. The data concerned 69 cases. All were presented with acute abdominal pain. None was malignant. The patients were aged between 47 and 65 years (mean 55.5 years); their parity ranged from 1 to 8 (average 5); the size of the specimens ranged from 6 to 20 cm (average 9.5 cm); and the right/left involvement was in the ratio of 3:2. It was concluded that there are well-acknowledged risk factors for ovarian torsion even in postmenopausal women presenting with acute abdominal pain. Consequently, even in a developing country, there is need for clinical awareness of this important entity.
Key words: Ovary, torsion, menopause, Nigeria.
INTRODUCTION
MATERIALS AND METHODS
RESULTS AND DISCUSSION
CONFLICT OF INTEREST
REFERENCES
|
Baker TE, Copas PR (1995). Adnexal torsion: A clinical dilemma. J. Reprod. Med. 40(6):447-449. |
|
|
Balci O, Icen MS, Mahmoud AS, Capar M, Colakoglu MC (2011). Management and outcomes of adnexal torsion: A 5-year experience. Arch. Gynecol. Obstet. 284(3):643-646. |
|
|
Basden GT (1966) (First ed. 1938) Niger Igbos, London Frank Cass |
|
|
Bayer AI, Wiskind AK (1994). Adnexal torsion: Can the adnexa be saved. Am. J. Obstet. Gynecol. 171(6):1506-1510. |
|
|
Bider D, Mashiach S, Dulitzky M, Kokia E, Lipitz S, Ben-Rafael Z (1991). Clinical, surgical and pathologic findings of adnexal torsion in pregnant and nonpregnant women. Surg. Gynecol. Obstet. 173(5):363-366. |
|
|
Bouguizane S, Bibi H, Farhat Y, Dhifallah S, Darraji F, Hidar S, Lassoued L, Chaieb A, Khairi H (2003). Adnexal torsion: A report of 135 cases. English Abstract. J. Gynecol. Obstet. Biol. Reprod. 32(6):535-540. |
|
|
Descargues G, Tinlot-Mauger F, Gravier A, Lemoine JP, Marpeau L (2001). Adnexal torsion: A report on forty-five cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 98(1):91-96. |
|
|
Eitan R, Galoyan N, Zuckerman B, Shaya M, Shen O, Beller U (2007). The risk of malignancy in post-menopausal women presenting with adnexal torsion. Gynecol. Oncol. 106(1):211-214. |
|
|
Gordon A, Rosenshein N, Parmley T, Bhagavan B (1980). Benign cystic teratomas in postmenopausal women. Am. J. Obstet. Gynecol. 138(8):1120-1123. |
|
|
Houry D, Abbott JT (2001). Ovarian torsion: A fifteen-year review. Ann. Emerg. Med. 38(2):156-159. |
|
|
Huchon C, Fauconnier A (2010). Adnexal torsion: A literature review. Eur. J. Obstet. Gynecol. Reprod. Biol. 150(1):8-12. |
|
|
Husain AR (2002). Life expectancy in developing countries: A cross-section analysis. Bangledesh Inst. Dev. Stud. 28:161-178. |
|
|
Koonings PP, Grimes DA (1989). Adnexal torsion in postmenopausal women. Obstet. Gynecol. 73(1):11-12. |
|
|
Lomano JM, Trelford JD, Ullery JC (1970). Torsion of the uterine adnexa causing an acute abdomen. Obstet. Gynecol. 35(2):221-225. |
|
|
Macartney JC, Rollason TP, Codling BW (1980). Use of a histopathology data pool for epidemiological analysis. J. Clin. Pathol. 33(4):351-355. |
|
|
McGovern PG, Noah R, Koenigsberg R, Little AB (1999). Adnexal torsion and pulmonary embolism: Case report and review of the literature. Obstet. Gynecol. 54(9):601-608. |
|
|
Nichols DH, Julian PJ (1985). Torsion of the adnexa. Clin. Obstet. Gynecol. 28(2):375-380 |
|
|
Oelsner G, Shashar D (2006). Adnexal torsion. Clin. Obstet. Gynecol. 49:459-463. |
|
|
Peng YY, Chen CH, Chien SC, Chen JR (2008). Torsion of a huge ovarian cyst in a 90 year-old woman. Taiwan J. Obstet. Gynecol. 47(2):224-225. |
|
|
Perez-Lopez FR, Chedraui P, Troyano-Luque JM (2010). Peri-and post-menopausal incidental adnexal masses and the risk of sporadic ovarian malignancy: New insights and clinical management. Gynecol. Endocrinol. 26(9):631-643. |
|
|
Rosai J (1996). Ackerman's Surgical Pathology. 8th ed. St Louis: Mosby-Year Book Inc, 1996:1450. |
|
|
Shih S, Vetto JT, Berek JS, Heaps JM, Hiatt JR (1991). Adnexal torsion. An unusual cause of abdominal pain in postmenopausal women. Am. Surg. 57(5):327-329. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


