Full Length Research Paper
ABSTRACT
Low iron status and Iron deficiency anemia are major prenatal complications predisposing pregnant women to preventable causes of premature delivery, intrauterine growth retardation and neonatal and prenatal death in Nigeria. Therefore, this study aims to evaluate and compare serum iron status in pregnant and non-pregnant women in Sapele, South-South Nigeria. A total of three hundred and sixty subjects were enrolled for this study comprising of 78 non-pregnant women and 282 pregnant women. 5 ml of venous blood were collected from participant into EDTA and plan containers respectively. The serum obtain from clotted sample was used for serum iron estimation using iron reduction method while EDTA blood was used for Packed Cell Volume (PCV) and hemoglobin estimation. Non-pregnant women had mean PCV value of 0.37±0.02 L/L with hemoglobin level of 12.3±0.9 g/dl and serum iron level of 132.6 ± 37.0 ug/dl. On the other hand, women with pregnancy had a mean PCV level of 0.32 ± 0.04 L/L, with hemoglobin and serum Iron level of 10.8 ± 1.5 g/dl and 96.4 ± 48.3 ug/dl respectively. Pregnant women had a significantly lower level of serum iron, PCV and hemoglobin when compare to non-pregnant women. This result points to the possibility of iron deficiency anemia among pregnant women in Sapele South-South Nigeria. It is believed that, information provided from this study will help in clinical care of pregnant women in this locality.
Key words: Iron status, pregnant women Sapele.
INTRODUCTION
Iron is a transitional metallic element essential for many developmental processes. Iron is vital for human growth because it is required for multiple metabolic processes, including DNA synthesis and erythropoiesis (Mark and Hoffbrand, 2005). Iron equilibrium in the body is regulated and diet is the main source of iron in human body, a normal western diet provides approximately 15 mg of Iron daily to the body (David, 2002). Poor diet and impaired dietary Iron absorption usually results in Iron deficiency which has been discovered to be the most common cause of anemia worldwide (Al-Farsi et al., 2011) and Iron deficiency anemia is the most frequent nutritional deficiency in pregnancy, with negative impact on maternal and fetal health, morbidity and mortality. Furthermore, Iron deficiency is regarded as the most important preventable causes of prenatal complications, such as premature delivery, intrauterine growth retardation and neonatal and perinatal death (Allen, 1997; Scholl, 2005).
Poverty and low economic status remain the major causes of low dietary Iron and poor nutritional quality among pregnant women in developing countries (United Nations, 2004; Gwatkin et al., 2004; Hong and Hong, 2007). Iron deficiency anemia, and malnutrition are major complications predisposing women to mortality. Many women in Nigeria, particularly among the poor have low nutritional status (World Bank/FMOH. Nigeria, 2005) and it has also been reported by World bank that there are worrisome levels of micronutrient deficiency among women in Nigeria and iron deficiency still remains a great challenge for women in antenatal care. Therefore, this study aims to evaluate iron status of pregnant women in central hospital, Sapele, south-south Nigeria.
Study design
This was a cross sectional and descriptive study carried out at Central Hospital, Sapele from June to August 2010. A total of three hundred and sixty subjects were enrolled for this study comprising of 78 non-pregnant women and 282 pregnant women. The first group being non-pregnant women was recruited from staff, youth corpers and other volunteers in central hospital Sapele. While the second group were pregnant women attending ante-natal clinic in same hospital Sapele. The second group were further divided into first trimester, second trimester and third trimester pregnancy according to ultrasonography reports. The sample was analyzed for full blood count and serum iron using Sysmex XN330 automated hematology analyzer and iron reduction method respectively.
Study site
Sapele is a city located in central part of Delta State, South-South Nigeria. It is positioned at a height of 9meters above sea level at latitude of 5.89° and a longitude of 5.68°. Sapele has a population of about 174,273 (Population census, 2006) and accommodates different tribes such as: Okpe, Urhobo, Itsekiri, Ibo, Ijaw, Isoko, Hausa, Edo, Yoruba, Ibibio, Nupe, Tiv, Fulani. The common diets in this locality are starch, yam, garri, rice, beans, plantain, palm oil, fish, meat, and periwinkle.
Exclusion criteria
Women without negative laboratory test results for pregnancy and those with complications of pregnancy were excluded from the study. Women who did not give consent for participation in this study were also excluded from this study.
Inclusion criteria
Women with positive laboratory test results for pregnancy and who gave consent for the study were included in this study.
Ethical approval
Approval for this study was obtained from the management of central hospital, Sapele, Delta Sate, Nigeria.
Sample collection
Five milliliters of venous blood was collected from participant by venipuncture into EDTA and plan containers respectively. EDTA blood was used for Packed Cell Volume (PCV) and hemoglobin estimation in automated analyzer while serum was obtained from clotted sample and used for serum iron estimation.
Sample analysis
The EDTA sample was placed in a position where the aperture is immersed in the blood and the aspirator button was pressed. A suspension of blood cell passes through a small orifice simultaneously with an electric current. After measurement, the result of the cell count, PCV and hemoglobin estimation were displayed on the screen and result recorded.
Serum Iron estimation
Using iron reduction method and TIBC reagent (obtained from TECO DIAGNOSTICS, Anaheim, USA). In this test, the iron in serum was dissociated from Fe (III) transferring complex by the addition of an acidic buffer containing hydroxylamine. This reduces the Fe (III) to Fe (II). The chromogenic agent, ferene, forms a highly coloured Fe (II)-complex that is measured photometrically at 560nm (Tietz, 1976; Henry, 1984).
Procedure for serum iron estimation
(1) Fresh, unhemolyzed serum was used in each case.
(2) Test tubes were labeled ‘Blank”, “Standard”, “Control”, and “Sample”
(3) 2.5 ml iron buffer reagent was added to all tubes.
(4) 0.5 ml sample was added to respective tubes and mixed, 0.5 ml iron free distill water was added to blank.
(6) Spectrometer was zeroed at 560 nm with the reagent blank
(7) The absorbance of all tubes (A1 reading) was read and mixed.
(8) 0.05 ml iron color reagent was added to all the tubes and mixed.
(9) All the tubes were placed in the heating bath at 37°C for minutes.
(10) The spectrophotometer was zeroed at 560 nm with the reagent blank (wavelength 520 – 560 nm).
(11) Absorbance of all the tubes were read (A2 reading and recorded).
Calculations of serum iron concentration
Using the formula: A2 test – A1 test x Conc, of Std = Total Iron (ug/dl)
A2 Std - A1 Std
Iron total = 60 - 150 ug/dl
A = Absorbance, Std = Standard
Conc = Concentration
Expected Values (Kit Reference Range)
Data analysis
The data from this study were collated, analyzed using SPSS version 20.0 and results were presented as mean ± Standard deviation.
RESULTS
Non-pregnant women had mean PCV value of 0.37±0.02 L/L with hemoglobin level of 12.3±0.9 g/dl and serum iron level of 132.6 ± 37.0 ug/dl. On the other hand, women with pregnancy had a mean PCV level of 0.32 ± 0.04 L/L, with hemoglobin and serum Iron level of 10.8 ± 1.5 g/dl and 96.4 ± 48.3 ug/dl respectively as shown in Table 2.
Table 1 shows the age distribution of study population in which 14 (3.89%) of pregnant women were between 10 and 19years of age while 144(40%) pregnant women were of the age range 20 to 29years. Pregnant women between the age 30 to 39 years made up 33.33% (120) of the study population and 4(1.11%) of pregnant women were of the age between 40-49years. Nevertheless, 72(20%) of pregnant women were in first trimester while 120(33.33%) were in second trimester of pregnancy and women in third trimester made up 25% of the pregnant women study population. Furthermore, age distribution among non-pregnant women reveals that, 1.39% (5) of non-pregnant women in this study were of age between 10 to 19years while those with age range 20 to 29years were 41(11.39%). On the other hands, 23(6.39%) and 9(2.5%) of non-pregnant women were of age range 30 to 39years and 40 to 49years respectively.
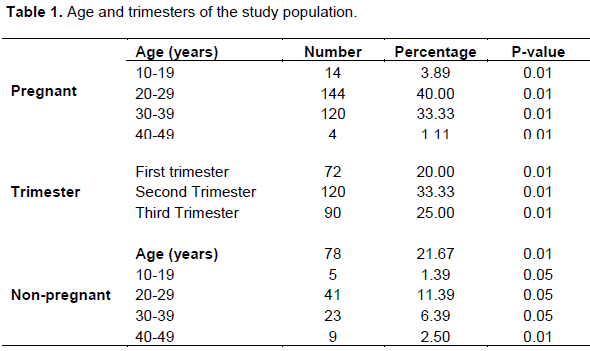
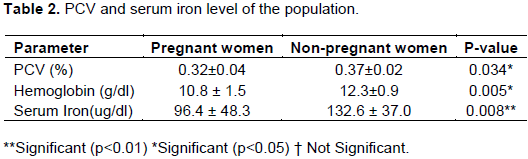
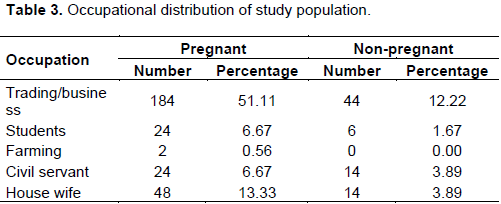
Table 3 shows occupational distribution among pregnant and non-pregnant women in the study population and 184(51.11%) pregnant and 44(12.22%) non-pregnant women were traders while, 24(6.67%) of pregnant and 6(1.67%) non-pregnant women were students. Nevertheless, 2(0.56%) pregnant women engage in farming while non-pregnant women who are farmers did not consent to participate in this study. Civil servant made up 24(6.67%) and 14(3.89%) of pregnant and non-pregnant women respectively. Pregnant women who were full time house wife were 48(13.33%) and non-pregnant house wife were 14(3.89%) of the population.
DISCUSSION
Serum iron status of pregnant and non-pregnant women in Sapele have been evaluated and it was discovered that pregnant women had a significantly lower level of serum iron than non-pregnant women this result points to the possibility of iron deficiency anemia among pregnant women in this locality. This result conforms with earlier report by Okafor et al. (2016) who stated that, iron deficiency was the commonest medical concern among women in Calabar rural community in south-south Nigeria. The prevalence of low iron status and iron deficiency anemia in pregnancy is still high in Nigeria (Ugwu and Uneke, 2020) and in several low income countries (Stevens et al., 2013). Lower iron level among pregnant women observed in this study may be due to poor nutritional and dietary quality as a result of less attention to food (Mekonnen et al., 2018) and low economic status of the studied population.
Furthermore, hemoglobin and PCV level was significantly lower in pregnant women than in non-pregnant women. This result is in tandem with earlier report by Percy and Mansour (2017) and this low hemoglobin level seen in this study is not unconnected with low serum iron because deficiency of iron causes a reduction in the rate of hemoglobin synthesis (Hassan et al., 2014). Age distribution of study population reveals that, women in age range 20-29years of age made up the highest percentage of pregnant participant in this locality while women of age range 40 to 49years were the least number of pregnant women seen in this study and this result is a pointer to the cultural and marriage pattern of women indicating predominancy of pregnancy among women in their twenties than those in forties years of age in Sapele.
Moreover, results obtained from this study indicates that women who were in their reproductive age were traders and business women while farmers made up the least number and this was another pointer to the occupational nature of reproductive women in this locality.
CONCLUSION
Pregnant women had a significantly lower level of hemoglobin, PCV and serum iron when compare to non-pregnant women. This result points to the presence of iron deficiency anemia among pregnant women and urgent need for dietary iron supplement for pregnant women in this locality.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The study was not sponsored, the equipment used was provided by the hospital in which this work was done.
REFERENCES
|
Al-Farsi YM, Brooks DR, Werler MM, Cabral HJ, Al-shafei MA, Wallenburg HC (2011): Effect of high parity on occurrence of anemia in pregnancy: A cohort study. BMC Pregnancy Childbirth 11:7. |
|
|
Allen LH (1997). Pregnancy and Iron deficiency unresolved issues. Journal of Nutrition and Review 55(4):91-101. |
|
|
David O (2002). Diet and Nutrition Environment: The savy vegetarian. Vegetarian 3(7):2-7. |
|
|
Gwatkin DR, Bhuiya A, Victoria CG (2004). Making health system more quitable. Lancet 364:1273-1280. |
|
|
Hassan AA, Mamman AI, Adaji S, Musa B, Kene S (2014). Anemia and iron deficiency in pregnant women in Zaria, Nigeria. Sub-Saharan African Journal of Medicine 1:36-39. |
|
|
Henry JB (1984). Clinical Diagnosis and Management by Laboratory Methods. WB Saunders, Philadelphia, p. 1434. |
|
|
Hong R, Hong R (2007). Economic inequality and undernutritional in women: multilevel analysis of individual, household, and community level in Cambodia. Food and Nutrition Bulletin 28(1):59-66. |
|
|
Mark W, Hoffbrand AV (2005). Iron metabolism, iron deficiency and disorders of haem synthesis," in Postgraduate Haematology, A. V. Hoffbrand, D. Catovsky, and E. G. D. Tuddenham, Eds., pp. 26-43, Blackwell, 5th edition. |
|
|
Mekonnen FA, Ambaw YA, Neri GT (2018) Socio-economic determination of anemia in pregnancy in North Shoa Zone, Ethiopia. PloS One 13:e0202734. |
|
|
Okafor IM, Okpokam DC, Antai AB, Usanga EA (2016): Iron Status of Pregnant Women in Rural and Urban Communities of Cross River State, South-South Nigeria. Nigerian Journal of Physiological Science 31(2):121-125. |
|
|
Percy L, Mansour D (2017): Iron Deficiency and iron deficiency anaemia in women's health. Obstetrics and Gynecology Journal 19:155-161. |
|
|
Scholl TO (2005): Iron status during pregnancy: Setting the stage for mother and Infant. American Journal of Clinical Nutrition 81(5):1218-1225. |
|
|
Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR (2013). Global, regional and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: A systematic analysis of population-representation data. Lancet Global Health 1:E16-25. |
|
|
Tietz NW (1976). Fundamentals of Clinical Chemistry. WB Sauders, pp. 923-929. |
|
|
Ugwu NI, Uneke CJ (2020). Iron deficiency anemia in pregnancy in Nigeria-A systematic review. Nigerian Journal of Clinical Practice 23(7):889-896. |
|
|
United Nations (2004). System standing Committee of Nutrition, 5th Report on the world nutrition situation. Nutrition for improved development outcomes. United Nations, New York 209:111-120. |
|
|
World Bank/FMOH. Nigeria (2005). Health, Nutrition and Population Country Status Report 2(Main Report) 17:3-9. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


