Full Length Research Paper

ABSTRACT
This research effort seeks to use doses of thioridaxine to enhance antibiotic sensitivity in a multidrug resistant (MDR) Staphylococcus aureus strain. Five axenic (pure) strains of S. aureus coded SA1 to SA5 were obtained from five infected midstream urine samples, inoculated on sterile cystine lactose electrolyte deficient (CLED) agar and stocked on sterile nutrient agar slants at 4°C in a refrigerator. Bacteria strains were sub-cultured on fresh sterile CLED agar and mannitol salt agar plates to confirm S. aureus strains. Gram staining, catalase test and coagulase test were done on the resulting colonies to further confirm the strains as S. aureus. Antibiotic susceptibility test was done by agar disc diffusion method using sterile Mueller- Hinton agar plates before and after treatment with laboratory dilutions of thioridaxine. S. aureus strains 1, 3 and 5 were multidrug resistant as they resisted 3 (37.5%), 3 (37.5%) and 4 (50.0%) of the antibiotics used. The highest (11.8±1.4 mm) and least (0.8±10.0 mm) zones of inhibition by all five strains were recorded for streptomycin and augmentin, respectively whereas, all five uropathogen strains resisted cloxacillin, they were sensitive to gentamycin, cotrimoxazole, chloramphenicol and streptomycin. After treatment with 2000 to 2240 ug/ml laboratory dilutions of thioridaxine, ≤50.0% loss of resistance was recorded for each of all seven dilutions but only 2240 ug/ml dilution recorded mean±S.E. loss of 56.2±17.8% for gentamycin, cotrimoxazole and streptomycin after treatment of SA5 uropathogen. This was followed by resistance losses of 41.4±10.8 and 42.7±8.3% induced by 2080 and 2200 ug/ml dilutions, respectively. Cumulative effect of all dilutions resulted in 40.0±8.2 and 40.5±17.1% borderline resistance losses to cotrimoxazole and chloramphenicol, respectively. Minimum inhibitory concentration of chloramphenicol was lowered by 2080, 2160 and 2240 ug/ml dilutions of thioridazine by four-fold (7.5 ug), four-fold (7.5 ug) and two-fold (15 ug), respectively. Upon this, the medical/chemotherapeutic implications of these findings are discussed.
Key words: In vitro, dilutions, thioridaxine, enhance, antibiotic, sensitivity, multidrug resistant Staphylococcus aureus.
Abbreviation: MDR, Multidrug resistant; CLED, cystine lactose electrolyte deficient; SDS, sodium dodecyl sulphate.INTRODUCTION
Antibiotics resistance is not a new phenomenon. However, the current magnitude and speed with which it is developing is a cause for global concern (Namita et al., 2012). According to WHO (2012), antimicrobial resistance is on the rise in Europe and all over the world with gradual loss of first line antimicrobials. Epidemiological studies have suggested that antibiotic resistance genes emerge in microbial populations within five years of the therapeutic introduction of an antibiotic (Chakrabarty et al., 1990). Hence, numerous classes of antimicrobial agents have become less effective as a result of the emergence of antimicrobial resistance often as a result of the selective pressure of their daily usage (Oskay et al., 2009). This selective pressure has been attributed to indiscriminate use of antibiotics, complex socio-economic behavioral antecedents and dissemination of drugs resistant pathogens in human medicine (Okeke et al., 1999). Moreover, the disappointing lack of new antimicrobial agents has led to overuse of existing ones thus leading to the emergence of multi-resistant pathogens (McGowan, 2006). Therefore, as the proliferation of multidrug resistant pathogens continue unavoidably within and around us, it is important that their resistance trend be put under check through intensive research and antibiotic surveillance (Akortha and Filgona, 2009). The primary causes of antibiotic resistance in bacteria are mobile elements called plasmids and conjugative transposons. Plasmids are extra chromosomal DNA elements that have the capacity to replicate independently of the chromosome of the bacterial cell (Madigan et al., 2003). Resistance plasmids or R plasmids code for enzymes that can inactivate antibiotics, prevent the uptake of an antibiotic or pump out the particular antibiotic (Neu, 1989). Other causes of antibiotic resistance are efflux pumps, mutation, under dosage or use of drugs without prescription (Amaral et al., 2013). Plasmids carry genes some of which code for beta-lactamase or extended spectrum beta lactamase which can inactivate or degrade drugs thus rendering them ineffective (Amaral et al., 2013).
Curing is the process of removing plasmids from a bacterial cell (Trevors, 1986). The resulting bacteria then become sensitive to the selective agent and it was initially thought that this phenomenon would proffer solution in controlling the development of antibiotic resistance in formerly antibiotic susceptible bacteria. DNA intercalating dyes (ethidium bromide), sodium dodecyl sulphate (SDS), antibiotics, thymine starvation and elevated tem-peratures have been used as curing agents (Chakrabarty et al., 1984; Gupta et al., 1980; Obaseki-Ebor, 1984; Reddy et al., 1986). Novobiocin, ethidium bromide, acriflavine, acridine orange, ascorbic acid and elevated temperatures have been used as curing agents (Ramesh et al., 2000). Physical treatments, chemical compounds and growth conditions may increase the frequency of elimination of drug resistant R-plasmids, resulting in sensitive cells that were previously resistant to antibiotics (Lakshmi et al., 1981). It has been reported that phenothiazines have the ability to control overexpression of efflux pump systems and thus are able to remove or reduce antibiotic resistance (Viveiros et al., 2010; Amaral et al., 2013). Mukherjee et al. (2012) reported the use of 1000 to 3000 ug/ml dilutions of a type of phenothiazine and an anti-psychotic drug called thioridaxine to cure a multidrug resistant strain of Pseudomonas aeruginosa. Multidrug resistance is now common among familiar pathogens such as Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, P. aeruginosa to mention but a few (Nabeela et al., 2004). The enormous genetic plasticity of the organism assists it to endlessly evolve resistance mechanisms against existing antimicrobial agents thus necessitating the need to control the spread of resistant Staphylococcal isolates in hospitals and health care settings (Gomber and Saxena, 2007).
Seventy percent to 90% of S. aureus strains demonstrate resistance to the penicillins and amino-penicillins and hence, infections are often difficult to treat because of widespread cross-resistance to amino-glycosides, macrolides, lincosamides, tetracyclines, cephalosporins, carbapenems, beta-lactamase inhibitor combinations, trimethoprim and sulphonamides (Nichols, 1999). While, vancomycin is often regarded as the last line of defense against nosocomial and community based S. aureus infections (Bhalakia, 2008), resistance has been reported and there is a major concern that total antibiotic resistant strains may emerge in the immediate future (Diekema et al., 2001). Soonafter, the use of penicillin, S. aureus was found to produce penicillinase (beta-lactamase).
To overcome this situation, the antibiotic-methicillin was used to replace penicillin and S. aureus strains resistant to methicillin emerged very quickly (Woo et al., 2003). This same pattern was also seen following the use of vancomycin. Treatments that increase frequency of elimination of plasmids will certainly enhance sensitivity (effectiveness) of antibiotics in situ. There is no published current work on use of laboratory dilutions of thioridaxine in the treatment (curing) of a multidrug resistant S. aureus uropathogen.
The focus of this work therefore, was the use of laboratory dilutions of thioridaxine to enhance the antibiotic sensitivity of multidrug resistant S. aureus uropathogen with the following objectives: 1) Determine the antibiograms of five selected S. aureus pure culture strains obtained from cultures of midstream urine samples after 37°C incubation for 24 h with the aim of selecting a multi-antibiotic resistant strain; 2) determine the antibiotic susceptibility profiles of a selected MDR S aureus strain in terms of ≤50% resistance loss after treatment with laboratory dilutions of thioridaxine (that is, 2000 to 2240 ug/ml); 3) show a summary of data of ≤50% resistance loss by thioridaxine dilutions after treatment on the MDR S. aureus strain; 4) determine thioridaxine dilutions’ effect(s) on the minimum inhibitory concentration (MIC) of a selected antibiotic that recorded borderline loss of resistance (that is, between 45 to 49% as borderline to ≤ 50%).
MATERIALS AND METHODS
Sampling
Five pure (axenic) isolates (strains) of S. aureus were obtained from 24 h CLED agar plate cultures with appropriate labeling. The agar plate medium used was one of several agar plates which had been inoculated with freshly voided midstream urine samples by a graduating student working on urinary tract infection in the Microbiology and Biotechnology laboratory of Western Delta University, Oghara. The status of the S. aureus isolates (strains) was re-confirmed by aseptically inoculating representative colonies on sterile Mannitol Salt agar plates. Inoculated plates were incubated aerobically at 37°C for 24 h. Gram reaction, biochemical and sugar fermentation tests by standard methods were then carried out to identify the resulting colonies (Cowan and Steel, 1993). Catalase positive, coagulase positive, bright yellow smooth gram positive cocci in clusters which were confirmatory of S. aureus were then stocked on sterile nutrient agar slants and kept at 4°C in the refrigerator after appropriate labeling for further use. The five bacterial uropathogens were then subjected to antibiotic sensitivity testing before treatment with laboratory dilutions of thioridaxine.
Antibiotic sensitivity testing
Antibiotic sensitivity testing was carried out on the pure culture colonies of the five S. aureus strains using the agar disc diffusion method on sterile Mueller-Hinton agar (MHA) plates (Bauer et al., 1966). A loopful of each colony of the uropathogens was picked aseptically using a flamed wire loop and placed in the centre of the sterile MHA plates. This was then spread all over the plates applying the caution of not touching the edges of the plates. The seeded plates were allowed to stand for about 2 min to allow the agar surface to dry. A pair of forceps was flamed and cooled and used to pick an antibiotic multidisc (Abitek, Liverpool) containing augmentin (30 ug), gentamicin (10 ug), erythromycin (5 ug), tetracycline (25 ug), cotrimoxazole (25 ug), cloxacillin (5 ug), chloramphenicol (30 ug) and streptomycin (10 ug). The discs were placed at least 22.0 mm from each other and 14.0 mm from the edge of the plates (Ochei and Kolkhatkar, 2008). Antibiotic discs were selected on the basis of their clinical importance and efficacy on various pathogenic strains of S. aureus. The seeded plates were allowed to stand for 10 min before incubation (Mbata, 2007). At the end of incubation, the diameters of the zones of inhibition from one edge to the opposite were measured to the nearest millimeter using a transparent ruler (Byron et al., 2003). Strains that showed resistance against three antibiotics and above were termed multiple drug resistant strains (Jan et al., 2004) and were noted and used further.
Preparation of laboratory dilutions of thioridaxine
Thioridaxine (a phenothiazine also known as 2-methylmercapto-10-(2-N-methyl-2-piperidyl-ethyl phenothiazine) dilutions of 2000 to 2240 ug/ml were chosen based on the lethal Dose-50 (LD50) of 956 to 1034 mg/kg administered orally on rats as reported by Barth et al. (2006) and in line with a similar study carried out by Mukherjee et al. (2011). Laboratory thioridaxine dilutions of 2000, 2040, 2080, 2120, 2160, 2200 and 2240 ug/ml were therefore prepared using RV/O where stock or original concentration of thioridaxine used was 50 mg tablet (Southwood Pharmaceuticals, UK). The 50 mg tablet was originally dissolved in 10 ml sterile water to give 5 mg/ml which is equivalent to 5000 ug/ml. To obtain 2000 ug/ml dilution, 2 ml of stock or original drug (5000 ug/ml thioridaxine) was mixed or diluted with 3 ml sterile water. To obtain 2040 ug/ml dilution, 5.1 ml of stock was mixed with 7.4 ml of sterile water. A mixture of 5.2 ml of stock drug solution with 7.3 ml of sterile diluent resulted in a dilution of 2080 and 2120 ug/ml dilution was obtained by mixing 5.3 ml of original drug solution with 7.2 ml of diluent (sterile water). To obtain 2160 ug/ml dilution, 5.4 ml stock drug solution was mixed with 7.1 ml of diluent, while a mixture of 1.1 ml of stock with 1.4 ml of diluent gave a dilution of 2200 ug/ml. Lastly, 2240 ug/ml was obtained by mixing 5.6 ml of stock with 6.9 ml of diluent.
Growing broth culture of MDR Staphylococcus aureus (SA5)
The stock culture of SA5 was selected from among the initial five stocked strains. An inoculum of SA5 was aseptically picked from its slant stock culture using flamed and cooled wire loop and inoculated into 10 ml sterile Nutrient broth (LabM, UK). The inoculated broth was incubated at 37°C for 18 h. The resulting turbid broth culture was then diluted according to a modified method of Shirtliff et al. (2006). Using a sterile pipette, 0.1 ml of broth culture was mixed with 19.9 ml (1:200 dilution) of sterile Nutrient broth. This was properly mixed and was used as working inoculum and should contain 105 to 106 organisms and used within 30 min (Ochei and Kolhatkar, 2008).
Treatment of SA5 uropathogen with prepared thioridaxine dilutions
The treatment of MDR S. aureus strain 5 with the prepared thioridaxine dilutions was done according to a modified method by Byron et al. (2003). Using a sterile pasteur pipette, 0.5 ml aliquot of the diluted overnight broth culture of SA5 uropathogen was added to 4.5 ml sterile molten Nutrient agar (LabM, UK) and mixed. The various prepared dilutions (one at a time) of thioridaxine were then added in 0.5 ml volume. The set up for each dilution was then poured on top of sterile hardened or set 2% Nutrient agar plates and left to set. The same antibiotic multidiscs used before treatment were then picked (using flamed and cooled pair of forceps) and impregnated on the set agar overlay plates. Plates were incubated at 37°C for 24 h. Measurement of diameter of zones of inhibition was taken and recorded (NCCLS, 2000).
Determination of effect of thioridaxine dilutions treatment on MIC of chloramphenicol
Serial doubling dilutions of chloramphenicol (using its MIC of 30 ug as a basis) was carried out. Chloramphenicol was chosen for this assay because it showed a mean ± S.E resistance loss of 40.5 ± 17.1 across all the dilutions (Table 3) and 45% is a borderline of ≤50.0% which is the benchmark for the purpose of this study. The idea is that any thioridaxine dilution that can reduce the MIC may enhance its sensitivity and therefore, loss of resistance is likely to shore up from 45%. Sterile cotton wool plugged test tubes numbering 11 (eleven) were set up on a test tube rack and labeled 1 to 11. Using a sterile pipette, 1 ml of sterile nutrient broth was dispensed into tubes 2 to 7. Two milliliters of Nutrient broth was dispensed into tube 8 as Nutrient broth control. Tubes 2 to 7 were then labeled with chloramphenicol concentrations of 120, 60, 30, 15, 7.5, 3.75 and 1.88 ug/ml. A 250 mg capsule of chloramphenicol was dissolved in 10 ml of sterile water and diluted to 240 ug/ml using RV/O in a sterile 200 ml transparent bottle. From this 240 ug/ml chloramphenicol preparation, 2 ml volume was pipetted into tube 1. From tube 1, one milliliter was pipetted into tube 2 and mixed and 1.0 ml was pipetted into tube 3 and mixed. From tube 3, 1.0 ml was pipetted into tube 4. Finally, 1.0 ml was pipetted into tube 7, mixed and 1.0 ml was pipetted out and discarded. The diluted S. aureus inoculum was then dispensed in 0.5 ml volume into tubes 2 to 7. Into tube 10, two milliliters of the diluted broth culture was dispensed. Into tube 9, two milliliters of the 240 ug/ml chloramphenicol diluted drug was dispensed. The first dilution of thioridaxine (2000 ug/ml) was then added (in 0.5 ml volume) to each tube and the content of each tube was properly mixed. The set up was repeated for each of the other dilutions of thioridaxine. All tubes were incubated in a water bath at 37°C for 24 h. The MICs as affected by each thioridaxine dilution were read and recorded.
RESULTS
Table 1 shows the antibiotic susceptibility pattern of S. aureus strains 1-5 isolated from mid-stream urine samples of which their sensitivity responses to gentamicin, tetracycline, chloramphenicol, augmentin, erythromycin, cloxacillin, cotrimoxazole and streptomycin are shown. S. aureus strains 1 and 3 resisted three antibiotics each (cloxacillin, tetracycline and augmentin), SA2 strain resisted two drugs (erythromycin and cloxacillin) while SA4 resisted two antibiotics which were cloxacillin and augmentin. Only S. aureus strain 5 (SA5) resisted 4 (50.0%) antibiotics and these were erythromycin, cloxacillin, augmentin and tetracycline. The highest (11.8±1.4 mm) and least (0.8±10.0 mm) zones of inhibition by all five strains were recorded for streptomycin and augmentin, respectively. All the five S. aureus uropathogens resisted cloxacillin. Because S. aureus strain 5 resisted more than three antibiotics, it was considered a multidrug resistant uropathogen and was used further in the study.
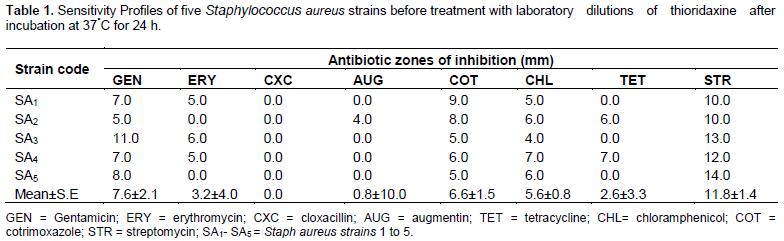
Table 2 shows the sensitivity profile of SA5 (S. aureus strain 5) after treatment with thioridaxine dilutions. The uropathogen was resistant to erythromycin, tetracycline, cloxacillin and augmentin. The uropathogen SA5 was sensitive to gentamicin, cotrimoxazole, chloramphenicol, and streptomycin with 8.0, 5.0, 6.0 and 14.0 mm zones of inhibition, respectively (Table 1). Table 2 also shows data of zones of inhibition of S. aureus strain 5 after treatment with laboratory dilutions of thioridaxine. Zones of inhibition before and after treatment were also mathematically computed to obtain ≤50.0% loss in resistance (that is, improvement in sensitivity). Treatment with 2000 ug/ml thioridaxine recorded a 60.0% loss of resistance to cotrimoxazole.
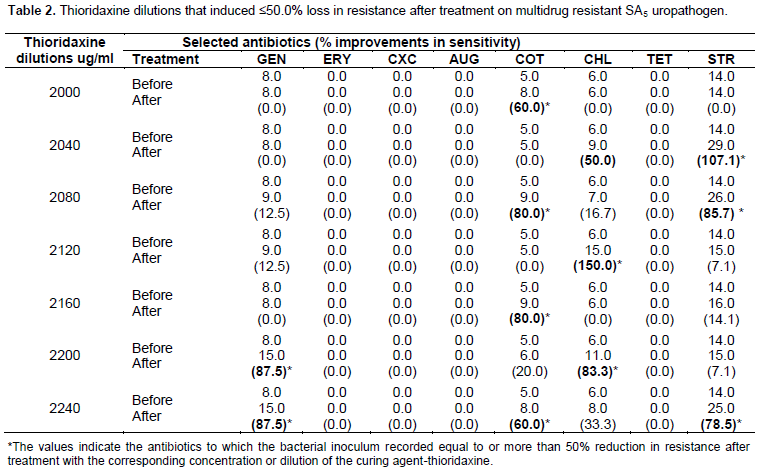
Sensitivity improvement or resistance losses of 50.0 and 107.1% were recorded for chloramphenicol and streptomycin, respectively, after treatment with 2040 ug/ml dilution of the chemical agent. After 2080 ug/ml thioridaxine treatment, 80.0 and 85.7% resistance losses were recorded for cotrimoxazole and streptomycin, respectively. The same curing treatment resulted in a less than 20% resistance loss to gentamycin and chloramphenicol, respectively.
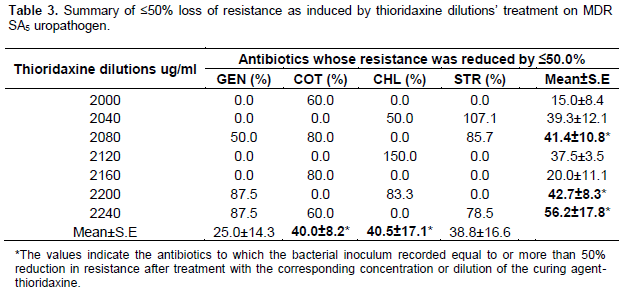
Resistance loss of 150.0% was recorded for chloramphenicol after the uropathogen was treated with 2120 ug/ml dilution of thioridaxine whereas 80.0% loss of resistance was recorded for cotrimoxazole after 2160 ug/ml thioridaxine treatment. For the same treatment, less than 15.0% loss was recorded for streptomycin. After 2200 ug/ml treatment, 87.5 and 83.3% loss of resistance were recorded for gentamycin and chloramphenicol, respectively, while 20.0% and less than 10% losses were recorded for cotrimoxazole and streptomycin, respectively. Lastly, resistance losses of 87.5, 60.0 and 78.5% were recorded for gentamicin, cotrimoxazole and streptomycin, respectively, after 2240 ug/ml thioridaxine treatment. Table 3 is a summary of ≤50% loss of antibiotic resistance after 2000 to 2240 ug/ml treatment with thioridaxine laboratory dilutions. With regard to Table 1, only gentamicin, cotrimoxazole, chloramphenicol and streptomycin recorded ≤50% loss in resistance. Only thioridaxine dilution of 2240 ug/ml recorded mean ±S.E loss of resistance for all the four antibiotics of 56.2±17.8%. Less than 45, 45, 40, 40 and 30% loss of resistance were effected by 2200, 2080, 2040, 2120, 2160 and 2000 ug/ml laboratory dilutions of thioridaxine, respectively, for all four antibiotics. All the dilutions put together recorded mean ±S.E loss of resistance of 40.5±17.1, 40.0±8.2, 38.8±16.6 and 25.0±14.3% in that descending order for chloramphenicol, cotrimoxazole, streptomycin and gentamycin, respectively. This means chloramphenicol and cotrimoxazole recorded borderline loss of resistance as compared with the benchmark of ≤50%. Data on the effect of thioridaxine dilutions on the minimum inhibitory concentration (MIC) of chloramphenicol on the multidrug resistant S. aureus strain 5 uropathogen are shown in Table 4.
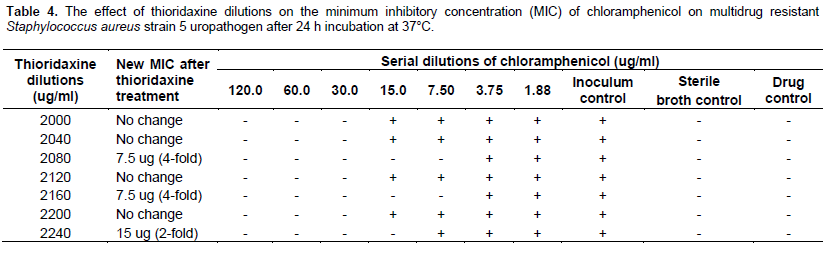
At the end of 24 h incubation at 37°C of the experimental set up, inoculum control tubes for all thioridaxine dilutions (2000 to 2240 ug/ml) showed turbidity (cloudiness) as expected. As expected also, sterile broth control and drug control tubes remained clear at the end of incubation. Laboratory dilutions of 2000, 2040, 2120l and 2200 ug/ml did not affect the minimum inhibitory concentration (MIC) of chloramphenicol as the MIC remained 30 ug. Reductions in MIC of chloramphenicol were however effected by 2080, 2160 and 2240 ug/ml thioridaxine dilutions. Thioridaxine dilutions of 2080 ug/ml and 2160 ug/ml reduced chloramphenicol MIC to 7.5 ug each which is a four-fold reduction, while 2240 ug/ml reduced the MIC to 15 ug (a two-fold reduction).
DISCUSSION
This study has the underlining intent of making suggestions aimed at reclaiming some common old and not too old drugs which are losing therapeutic usefulness owing to ineffectiveness in terms of therapeutic outcome. The alternative is to replace the old drugs with new ones but it will be counter-productive because such new drugs may be more costly, may be toxic (that is, may have more adverse side effects), their use may need much longer stay in the hospital (or longer duration of treatment) and their use may require treatment in intensive care units. Antibiotic susceptibility profiles of all five strains (uropathogens) of S. aureus before thioridaxine treatment in this study showed that the five uropathogen strains were sensitive to gentamicin, cotrimoxazole, chloram-phenicol and streptomycin with mean± SE zones of inhibition of 7. 6 ± 2.1, 6.6 ± 1.5, 5.6 ± 0.8 and 11.8 ± 1.4 mm, respectively. The implication of this is that 4(50.0%) of the antibiotics recorded positive reactions at the end of incubation. Whereas, the five uropathogen strains were resistant to cloxacillin, strains SA1 and SA3 resisted three antibiotics each which were cloxacillin, tetracycline and augmentin.
Strain SA2 resisted erythromycin and cloxacillin while SA4 resisted cloxacillin and augmentin. The fact that SA5 strain resisted more than three antibiotics (that is, erythromycin, cloxacillin, augmentin and tetracycline) qualifies it as a multidrug organism (Jan et al., 2004; Otajevwo, 2012). Strain SA5 was sensitive to gentamycin, cotrimoxazole, chloramphenicol and streptomycin. Findings suggest that infections or diseases caused by MDR S. aureus strain 5 in the study environment and perhaps in other environments can be treated successfully with gentamicin/cotrimoxazole/ chloramphenicol/streptomycin (that is, any one of the four) only or in synergistic combination a physician may consider safe and potent. The privilege of choosing any of the four (except streptomycin perhaps) will be cheering to low income patients in terms of cost and availability. The almost total resistance recorded against augmentin is worrisome because it is a drug that is used to treat a good number of human diseases. Some authors have also expressed similar worry over augmentin in terms of antibiotic susceptibility (Oluremi et al., 2011; Otajevwo, 2012; Otajevwo, 2014). It was not clear whether the site from where the pathogens were isolated had any direct or indirect effect on the antibiograms of the strains as recorded in this study. However, it may be possible that pH changes or variation from site and presence /absence of oxygen could affect the response of S. aureus (a facultative aerobe) to relevant antibiotics it is exposed to in vitro. The sensitivity profile obtained in this study however, is subject to verification and confirmation by other researchers.
The fact that each of the five strains was resistant to two-four of the antibiotics used in this study may suggest that very large population of S. aureus organisms have been exposed to several antibiotics (Oluremi et al., 2011). Thioridaxine laboratory dilutions of 2000, 2040, 2080, 2120, 2160, 2200 and 2240 ug/ml were used to treat and cure five uropathogenic strains of S. aureus with the intent of reducing their resistance significantly or eliminating it completely. The loss of (≤50%) resistance after treatment with the stated dilutions of thioridaxine was used as the basis of establishing the curing effects of these dilutions. The use of 50% and above loss in resistance as a criterion to determine the extent of plasmid curing was according to the scheme provided by Akortha et al. (2011). Stanier et al. (1984) reported that the elimination of plasmids by dyes and other natural agents reflects the ability of such an agent to inhibit plasmid replication at a concentration that does not affect the chromosome. After treatment with 2000 to 2240 ug/ml thioridaxine dilutions, S. aureus strain 5 still remained completely resistant to erythromycin, cloxacillin, augmentin and tetracycline. This could be due to the fact that plasmids responsible for resistance to these drugs may be chromosome- mediated or non- conjugative plasmids (Akortha and Filgona, 2009). Many authors have profusely reported occurrence of multidrug resistant S. aureus in their studies (Gales, 2000).
Thioridaxine dilution of 2000 ug/ml induced 60.0% loss of resistance of the uropathogen to cotrimoxazole. Also, only two antibiotics namely chloramphenicol and streptomycin recorded 50.0 and 107.1% resistance losses respectively after 2040 ug/ml thioridaxine treatment (Tables 2 and 3). In a similar study, some authors have used 2000 ug/ml thioridaxine dilution treatment to induce loss of resistance (enhance antibiotic sensitivity) in some multidrug resistant strains of Pseudomonas aeruginosa and recorded elimination (curing) of antibiotic resistance in thioridaxine treated strains (Mukherjee et al., 2012). It was concluded in their report that the antipsychotic drug-thioridaxine is a potent agent able to eliminate drug resistance plasmids which are much longer in size than the plasmids of other gram negative bacteria (Mukherjee et al., 2012). From these results, it seems thioridaxine dilution of 2240 ug/ml and perhaps, 2080 or 2200 ug/ml may possess the capacity to eliminate resistance put up by multidrug resistant strains of S. aureus and therefore, could be administered in the therapeutic control of various infections caused by such bacteria. According to Mukherjee et al. (2012), the simultaneous application of thioridaxine to patients may open up a new arena of therapy. The simultaneous application of thioridaxine may not only act as an additional antibacterial agent but may also help to eliminate the drug resistant plasmids from the infectious bacterial cells (Spendler et al., 2006). Hence, patients suffering from MDR S. aureus infections may be administered thioridaxine at standard human doses (using 2240 or 2080 or 2200 ug/ml as a basis) along with antibiotics especially gentamicin, chloramphenicol, cotrimoxazole or streptomycin.
Also in this study, sensitivity enhancement effect of thioridaxine laboratory dilutions on the minimum inhibitory concentration (MIC) of chloramphenicol as it affected MDR S. aureus strain 5 uropathogen showed a four-fold (7.5 ug), four-fold (7.5 ug) and two-fold (15 ug) reductions in MIC of chloramphenicol as recorded for 2080, 2160 and 2240 ug/ml thioridaxine dilutions, respectively. Some authors had reported similar findings on MDR S. aureus strains (Otajevwo and Momoh, 2013) as well as on MDR strains of Pseudomonas aeruginosa using acridine orange (Otajevwo and Okungbowa, 2014). Otajevwo (2012) reported similar results using ethidium bromide dilutions on MDR strain of E. coli. A fast and accurate determination of MIC can ensure optimal effective treatment of patients while at the same time avoiding over-prescription. This will save money for healthcare providers as well as reduce development of resistance (NCCLS, 2000; McGowan and Wise, 2001).
The MIC of chloramphenicol which is 30 ug (based on long standing research) was reduced to 7.5 ug (four-fold reduction), 7.5 ug (four-fold reduction) and 15 ug (two-fold reduction) by thioridaxine laboratory dilutions of 2080, 2160 and 2240 ug/ml, respectively, as tested on multiple resistant drug strain of S. aureus isolated from the urinary tract of a patient.
According to Dimitru et al. (2006), there is a significant correlation between MIC values and the inhibition zone diameters obtained by a 30 ug disc. The lower the MIC and the larger the zone of inhibition, the more susceptible the microorganism is to the antimicro-bial agent and conversely, the higher the MIC and smaller the zone of inhibition, the more resistant the microorganism (Dimitru et al., 2006).
The medical implication therefore of the four-fold, four-fold and two-fold reduction of chloramphenicol MIC by thioridaxine dilutions of 2080, 2160 and 2240 ug/ml, respectively, is that when doses of one of these dilutions or a combination of any two are incorporated into the manufacture of chloramphenicol or any other related antibiotic and then administered to a patient diagnosed to be suffering from a disease caused by MDR S. aureus strain, a better result in terms of outcome (cure of the disease) may be achieved as it will require four times its concentration to function in vivo.
In a related work, Kohler (2010) showed that the resistance of P. aeruginosa to tetracycline efflux was reduced from MIC 0.032 to 0.004 ug/ml (an eight- fold reduction) by treatment with phenothiazine. Crowle et al. (1992) demonstrated that non- toxic concentrations of phenothiazine in the lungs achieved complete elimination of Mycobacterium tubercolosis. In a related study, some workers had reported the capacity of an aqueous methanolic plant- extract- epidiosbulbin- E- acetate (EEA) to decrease the MIC of antibiotics against MDR bacteria thus making antibiotic treatment more effective (Shiram et al., 2008).
CONCLUSION
Thioridaxine laboratory dilution of 2040 ug/ml induced ≤50% resistance losses for gentamicin, cotrimoxazole, chloramphenicol and streptomycin. Also, 2080, 2160 and 2240 ug/ml thioridaxine dilutions effected chloramphenicol MIC reductions by four-fold, four-fold and two-fold, respectively. Hence, patients suffering from MDR S. aureus infections may be administered thioridaxine at standard human doses (using 2080, 2160 and or 2240 ug/ml as a basis) along with any of the above antibiotics (singly or in combination). It is hoped that this simultaneous or part application of thioridaxine with antibiotics will eliminate plasmids while enhancing the penetration of antibiotics into pathogenic bacterial cells especially those of MDR S. aureus. The likely effect of this is that patient recovery will be facilitated and hospital stay and hospital cost would be drastically reduced.
CONFLICT OF INTERESTS
The author did not declare any conflict of interest.
REFERENCES
|
Akortha EE, Aluyi HAS, Enerijiofi KE (2011). Transfer of amoxicillin resistance gene among bacteria isolates from sputum of pneumonia patients attending the University of Benin Teaching Hospital, Benin City, Nigeria. J. Med. Sci. 2(7):1003-1009. |
|
|
Akortha EE, Filgona J (2009). Transfer of gentamicin resistance genes among enterobacteriaceae isolated from the outpatients with urinary tract infections attending three hospitals in Mubi, Adamawa State. Sci. Res. Essay 4(8):745-752. |
|
|
Amara L, Spendler G, Martins A, Molnar J (2013). Efflux pumps that bestow multidrug resistance of pathogenic gram negative bacteria. Biochem. Pharmacol. J. 2(3):119-121. |
|
|
Barth VN, Charnet E, Martin LJ, Need AB (2006). Comparison of rat dopamine D2 receptor occupancy for a series of anti-psychotic drugs like thioridaxine. Life Sci., 78(26):3007-3019. |
|
|
Bhalakia N (2008). Isolated and plasmid analysis of vancomycin resistant Staph. aureus. J. Young Investigators. 18:1-5. |
|
|
Bauer AW, Kirby WMM, Sherris JC, Turk M (1966). Antibiotic susceptibility testing by a standardized single disc method. Am.J.Clin. Pathol. 45:493-496. |
|
|
Byron F, Brehm S, Eric AJ (2003). Sensitization of Staphylococcus aureus and Escherichia coli to antibiotics by these sesquiterpenoids. Antimicrob. Agents Chemother. 47(10):3357-3360. |
|
|
Chakrabarthy PK, Mishra AK, Chakrabarti SK (1984). Loss of plasmid-like drug resistance after treatment with iodo-deoxyuridine. Indian J. Expt. Biol. 22: 333-334. |
|
|
Crowle AJ, Douvas SG, May MH (1992). Chlorpromazine: a drug potentially useful for treating Mycobacterial infections. Chemotherapy 38:410-419. |
|
|
Diekema DJ, Pfaller MA, Schmitz FJ (2001). Survey of infections due to Staphylococcus spp: Frequency occurrence and antimicrobial susceptibility of isolates collected in the United States, Canada, Latin America, Europe and the Western Pacific region for the SENTRY antimicrobial surveillance programme. Clin. Infect. Dis. 32(2):5114-5132. |
|
|
Dimitru G, Poiata A, Tuchilus C, Buiuc D (2006). Correlation between linezolid zone diameter and minimum inhibitory concentration valves determined by regression analysis. Rev. Med. Chir. Soc. 110(4):1016-1025. |
|
|
Gomber C, Saxena S (2007). Anti-Staphylococcal potential of callistemon rigidus. Cent. Eur. J. Med. 2:79-88. |
|
|
Gupta TD, Bandyopathy T, Dastidar SG, Bandopadhyay M, Mistra A, Chakrabarty AN (1980). R- plasmids of Staphylococci and their elimination by different agents. Indian J. Expt. Biol. 18:478-481. |
|
|
Jan MB, John DT, Sentry P (2004). High prevalence of oxacillin resistant Staph aureus isolates from hospitalized patients in Asia-Pacific and South Africa: Results from SENTRY antimicrobial surveillance program. 1998-1999. Antimicrob. Agent Chemother. 46:879-881. |
|
|
Lakshmi VV, Padma S, Polasa H (1989). Loss of plasmid antibiotic resistance in Escherichia coli on treatment with some compounds. FEMS Microbiol. Letts. 57:275-278 |
|
|
Kohler NO (2010). Non- antibiotics Reverse Resistance of Bacteria to Antibiotics in vivo. J. Antimicrob. Chemother. 24(5):751-754. |
|
|
Madigan M, Martinko J, Parker J (2003). Brock Biology of Microorganisms (10th edn). Prentice Hall, Upper Saddle River, NJ., USA. 500p. |
|
|
Mbata TI (2007). Prevalence and antibiogram of UTI among prisons Inmates in Nigeria Inter. J. Microbiol. 3(2):10-15. |
|
|
McGowan JE (2006). Resistance in non-fermenting gram negative bacteria: multidrug resistance to the maximum. Am. J. Infect. Control 34:29-37. |
|
|
McGowan AP, Wise R (2001). Establishing MIC breakpoints and the interpretation of in vitro susceptibility tests. J. Antimicrob. Chemother. 48:17-28. |
|
|
Mukherjee S, Chaki S, Das S, Sen S, Datta SK, Dastidar SG (2011). Distinct synergistic action of piperacillin and methylglyoxal against Pseudomonas aeruginosa. Indian J. Exp. Biol. 49:447-551. |
|
|
Mukherjee S, Chaki S, Barman S, Das H, Koley, Dastidar SG (2012). Effective elimination of drug resistance genes in pathogenic Pseudomonas aeruginosa by an antipsychotic agent–thioridaxine. Curr. Res. Bacteriol. 5:36-41. |
|
|
Namita J, Pushpa S, Lalit S (2012). Control of multidrug resistant bacteria in a tertiary care hospital in India. Antimicrob. Resistance & Infection Control. 1:23-30. |
|
|
NCCLS (2000). Methods for dilution, Antimicrobial Susceptibility Tests for bacteria that grow aerobically. Approved Standard (5th edition). Wayne, PA, USA. |
|
|
Neu HC (1989). Overview of mechanisms of bacterial resistance. Diagnost. Microbiol. Infect. Dis. 12:109-116. |
|
|
Obaseki-Ebor EE (1984). Rifampicin curing of plasmids in Escherichia coli K12 rifampicin resistant host. J. Pharm. Pharmacol. 36: 467-470. |
|
|
Ochei J, Kolhhatkar A (2008). Medical Laboratory: Theory and practice, 10th edition. New Delhi: Tata McGraw-Hill Publishing Company. 1338p. |
|
|
Okeke IN, Lamikanra A, Edelman R (1999). Socio-economic and behavioural factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg. Infect. Dis. 5:18-27. |
|
|
Oluremi BB, Idowu AO, Olaniyi JF (2011). Antibiotic susceptibility of common bacterial pathogens in urinary tract infections in a Teaching Hospital in Southwestern Nigeria. Afr. J. Microbiol. Res. 5(22):3658-3663. |
|
|
Oskay M, Oskay D, Kalyoneu F (2009). Activity of some plant extracts against multidrug resistant human pathogens. Iranian J. Pharm. Res. 8(4): 293-300. |
|
|
Otajevwo FD, Momoh SA (2013). Resistance marker loss of multi-drug resistant (MDR) Staphylococcus aureus strains after treatment with dilutions of acridine orange. J. Med. Med. Sci. 2(2):43-62. ISSN: 2241-2328. |
|
|
Otajevwo FD, Okungbowa A (2014). A study on resistance loss of multidrug resistant (MDR) Pseudomonas aeruginosa strains after treatment with dilutions of acrdine orange. Intl. J. Med. Med. Sci. 6(1):24-33. |
|
|
Otajevwo FD. (2012). Sensitivity enhancement of multidrug resistant urinary tract Escherichia coli isolate to some commonly used Antibiotics after treatment with non-toxic laboratory concentrations of homodium bromide. IOSR J. Pharm. 2(3): 540-568 |
|
|
Ramesh A, Halami PM, Chandrasekhar A (2000). Ascorbic acid induced loss of a pediocin-encoding plasmid in Pediococcus acidilactici CFR K7. World J. Microbiol. Bio. 16:695-697. |
|
|
Reddy G, Shridhar P, Polasa H (1986). Elimination of Col. E1 (pBR322 and pBR329) plasmids in Escherichia coli on treatment with hexamine ruthenium III chloride. Curr. Microbiol. 13: 243-246. |
|
|
Shiram V, Jahagirdar S, Latha C, Kumar V, Puranik V, Rojatkar S (2008). A potential plasmid curing agent, 8-epidiosbulbin E acetate from Dioscorea bulbifera L against multidrug resistant bacteria. Intl. J. Antimicrob. Agents. 32(5): 405-410 |
|
|
Stanier RY, Adelberg EA, Ingraham JL (1984). General Microbiology, 4th edn. The Macmillan Press Ltd, Basingstoke London. |
|
|
Trevors JT (1986). Plasmid curing in bacteria. FEMS Microbiol. Rev. 32(3):149-157. |
|
|
Viveiros M, Jesus A, Brito M, Leandro C, Martins M. (2010). Inducement and reversal of tetracycline resistance in Escherichia coli K12 and expression of proton gradient-dependent multidrug efflux pumps genes. Antimicrob. Agents Chemother. 49:3578-3582. |
|
|
Woo PCY, Lau, SKP, Yeun KY (2003). Facilitation of horizontal transfer of antimicrobial resistance by transformation of antibiotic-induced cell wall- deficient bacteria. Med. Hypot. 61(4):503-508. |
|
|
World Health Organization. (2012). Antimicrobial resistance in the European Union and the World. Lecture delivered by Dr Margaret Chan, Director-General of WHO at the Conference on combating antimicrobial resistance: time for action. Copenhagen, Denmark, March 14th, 2012. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


