This study examined the barriers to open defecation (OD) free in Kwahu Afram Plains South District, Ghana. A combination of diverse tools was used to collect the data (in-depth interviews, Focus Group Discussions (FGDs) and observation), different means was adopted in selecting the participants. Much of the time in the early stages of the field work was spent having interactions with various groups within the community. Notable groups include the community care coalition, savings groups, mother to mother support groups and community child protection committee (CPCC), the fishmongers as they waited for fish at the beach, and the fishermen who had either returned from fishing or did not go for fishing and were relaxing under their shed. A questionnaire was administered to 169 households randomly selected from 6 communities in the Tease Area Council and 5 communities in the Samanhyia Area Council. The findings revealed that, 69% indicated their responsiveness to continue OD if subsidy is not introduced. 64% alluded that, every household should own a sanitary toilet facility however in terms of measures to ensure sanity at the toilet facility. 110 respondents representing 65% were not able to articulate a measure to the usage of sanitary toilet facility. 74% were not able to articulate a measure to ensure cleanliness at the toilet facility. The findings of the research conclude that, the inability of households to construct toilet facility highly influenced the state of open defecation in communities and this is translated into the limited toilet facilities in communities.
The Joint Monitoring Programme (JMP) of the World Health Organization (WHO) and UNICEF defines improved sanitation as “a sanitation system in which excreta is disposed of in such a way that there is reduced risk of faecal-oral transmission to its users and the environment”. Specific types of improved sanitation facilities recognized by the JMP include flush or pour-flush latrine, pit latrine with a slab, ventilated improved pit (VIP) latrine and the composting toilet (Karnib, 2014). To be accepted as ‘improved’, a sanitation facility is required to be used exclusively by only one household.
Access to improved latrines at home and in public places is a crucial defense to humans and the environment against faecal-oral transmission of pathogenic agents (Mara et al., 2010).
The case of low-income peri-urban and urban slums is of much greater concern due to their frequent association with vector-borne diseases, bacterial infections and contamination of drinking water amidst a rapidly growing population (Nakagawa et al., 2006).
Nevertheless, the impact of latrine provision on public health is dependent on the response of the intended users, especially their commitment to regularly use and maintain the facility. To ensure regular latrine usage, the choice of technology, the design and construction of facilities, as well as their operation and maintenance should be directly linked to the defecation practices, preferences and cultural values of the intended users (Garfi and Ferrer-Marti, 2011). It is, therefore, crucial to understand the factors that influence latrine usage and the barriers to regular use in any cultural and socio-economic context. Understanding of such factors is required to guide the development of technical and social interventions that are consistent and likely to stimulate local drivers of latrine usage (Sarkingobir and Sarkingobir, 2017).
In Ghana, only 14% of the population has access to improved sanitation as against an MDG target of 54% set for 2015 (JMP, 2014). The proportion of Ghana’s population depending on shared sanitation, including public toilets (59%), is the highest in the world (JMP, 2014). According to the JMP, 19% of Ghanaians practice open defecation while 8% depend on various forms of unimproved sanitation options such as bucket latrines. In terms of technology mix, nearly half of Ghanaian households depend on dry sanitation systems such as the simple pit and ventilated improved pit latrines while 10% depend on wet or flush on-site systems (Ghana Statistical Service, 2008). Sewerage is only piloted in parts of the country and covers only about 3% of Ghanaian households (GSS, 2013). To improve the status of sanitation in the country, the government has over the last decade introduced a number of policies including the adoption of the community-led total sanitation (CLTS) approach and a strong advocacy for households in residential areas to acquire their own toilet facilities, with public sanitation facilities only recommended for transport terminals and other commercial centers (Ministry of Local Government and Rural Development, 2010a). In spite of the recent efforts to improve sanitation in Ghana, the statistics show that progress towards the Millennium Development Goals (MDGs) has been slow, with some policies simply not yielding the anticipated results. For instance, the use of hygiene education and subsidies to increase household latrine uptake under the Rural Water Supply Programme IV (2005-2009), implemented in selected districts in the Ashanti Region, failed to generate the expected response from the beneficiaries (Ampadu-Boakye et al., 2011). In each of the participating districts, 226 latrines were allocated to be constructed with 50% subsidy. However, in some districts, less than 5% of the allocated latrines were actually constructed under the programme. Among the reasons attributed to the poor response to the intervention in these districts was the failure to conduct background studies in the communities prior to the start of the project.
Thus, this study was conducted in the coastal peri-urban setting of Ghana to understand the factors influencing latrine usage and the barriers or constraints that discourage regular use of existing household and communal latrines.
Description of the study areas
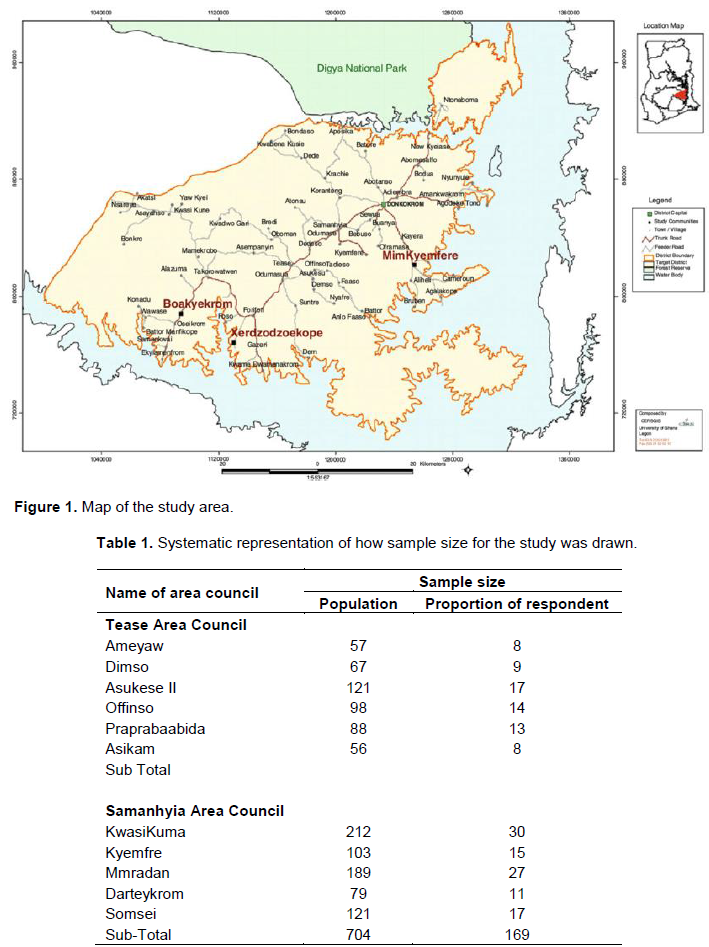
The study was conducted in two area councils of the Kwahu Afram Plains South District. The Area Councils were Samanhyia Area Council and Tease Area Council (Figure 1). The Kwahu Afram Plains South District was carved out from the Kwahu North District and forms part of the newly created districts in the country. The Afram Plains South District is located between Latitudes 6° 401 N and 7° 101 N; longitudes 0° 401E and 0° 10 I E; at the North-Western corner of Eastern Region with a total land area of approximately 3,095 km2. The district is bounded to the north by the Kwahu Afram Plains North, to the south by Kwahu South, to the east by the Volta River and to the west by two districts in the Ashanti region precisely Sekyere East and Ashanti-Akim Districts (GSS, 2013).
Data collection and analysis
The study communities were selected due to peculiar socio-economic and demographic characteristics as a result of the differences in their physical locations, which invariably influence their defecatory preferences and practices (Table 1).
Proportion of respondents
A proportional sampling technique was used to sample participants for the study.
Proportion of respondent = Population per community/Total population (both councils) ×100
A combination of diverse tools was used to collect the data (in-depth interviews, Focus Group Discussions (FGDs) and observation), different means was adopted in selecting the participants. Much of the time in the early stages of the field work was spent having interactions with various groups within the community. Notable groups include the community care coalition, savings groups, mother to mother support groups and community child protection committee (CPCC), the fish mongers as they waited for fish at the beach, and the fishermen who had either returned from fishing or did not go for fishing and were relaxing under their shed. A total of 297 respondents were selected from the Samanhyia Area Council and Tease Area Councils of the Kwahu Afram Plains South District.
All the informants and discussants for the study were purposively selected. They were people that is believed to have rich information and from whom one could learn much about issues of central importance to the purpose of the research. Informants and participants were made up of adult males and females and the youth living in the community. A set of selection criteria was developed which aided in hand-picking the informants and participants. Informants for the in-depth interviews were drawn from the Environmental Health and Sanitation Directorate of the District Assembly, chiefs and opinion leaders, Water and Sanitation Management Committee (WATSAN). The criteria for selecting key informants were: being an indigene or migrant who had lived in the community for at least ten years, having good knowledge of the history of the community, and should be above 18 years old.
Data processing and analysis
The data was checked for distribution and outliers. The questionnaire was coded in Statistical Package for Social Sciences (SPSS) version 17; descriptive statistics was done to derive numerical and non-numerical data presentation models including graphs, tables and frequencies among others for the quantitative data. For qualitative, data was coded according to the objectives. Grouping of the coded data was done according to themes after reading through. The recorded interviews were transcribed for the qualitative study and were used in write-up under specific themes.
Demographic characteristics of respondents
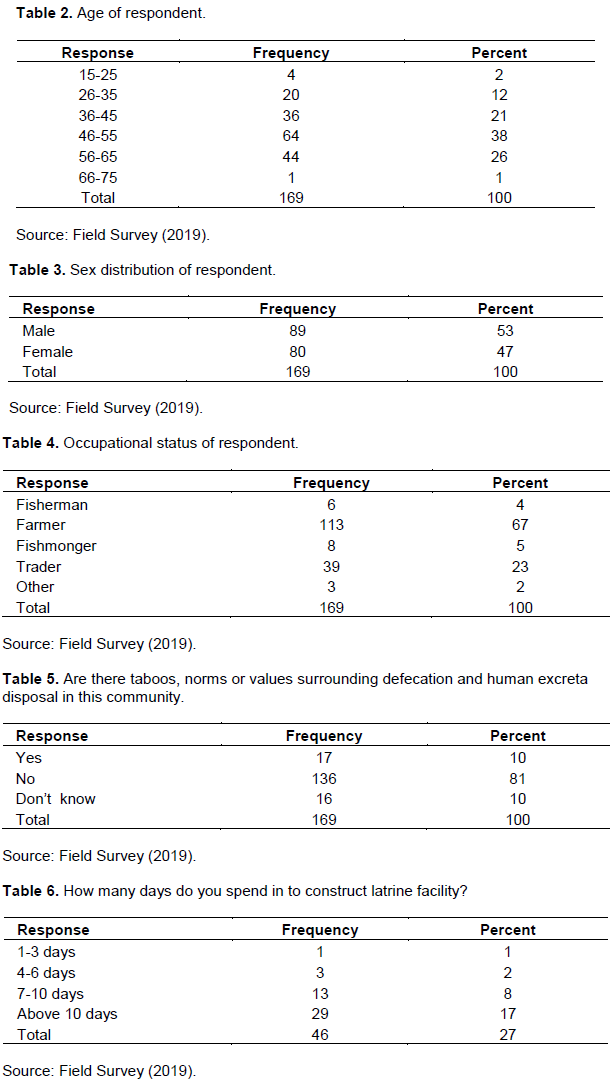
The finding of the study specifies that 38% of the respondents were between the ages of 46-55 years. 26% of the respondents were between the ages of 56-65 years. 21% were between the ages of 36-45 years. 12% of the respondents were between 26-35 years while 2 and 1% of the respondents were between the ages of 15-25 years and 66-75 years. It can be observed that, the majority of the respondents were within the labour force representing 59% (Table 2).
Table 3 shows that, the sex distribution of the respondents. From the table, 53% were male while 47% were found to be female.
The findings of the study reveal that, 67% of the respondents were farmers while 23.1% were traders. 5% of the respondents were fishmongers while 4% of the respondents were fishermen. The remaining 2% were pupil teachers (Table 4).
Determination of the social, economic, and physical barriers to open defecation free
According to Table 5, majority of the respondents representing 81% indicated that, there is no taboo that regulates open defecation in the community. However, 10% of the respondents indicated otherwise.
The findings of the study revealed the following taboos that have restricted families to end open defecation.
“…The faeces of in-laws should never mix. To avoid the father-in-law and daughter-in-law’s faeces mixing, there are gender-segregated open defecation sites so that the taboo is not broken…”
Another respondent indicated that “… I do not use another family’s open defecation site, lest you are bewitched. Our family lineage believes that person’s faeces can be used to bewitch us. Therefore, we avoid using a defecation site other than their own. Witchcraft still plays a major role in our community and we have a mortal fear of being bewitched…”
The findings of the study describes that, faeces could easily be picked up and used for witchcraft once they have left. So it is common for people upon visiting a neighboring house to walk all the way back to their own home, should they feel the urge to attend to a ‘call of nature’.
According to Table 6, majority of the respondents representing 17% indicated that, it took them more than 10 days to construct toilet facility. 8% indicated 7-10 days period, 2% indicated between 4-6 days period while 1% indicated 1-3 days period.
According to the Chairman of the WATSAN committee, “…Site selection and orientation usually do not take more than a day to carry out this first phase of the construction activity. Much of the time is spent on procurement processes. I will need a huge sum of money to procure all the needed materials for the construction. I will need a concrete ring ( 32” × 16”) at least 3, 1 ring cover, 2 bag of 50 kg cement, 10 cement bag of sand, 3 cement bag of gravels, 280 bricks, 1 set of pan with siphon, 3 ft HDPE pipe 4” and a skilled labour and mason. As a farmer, I cannot afford to procure all these materials within a day or two. I will have to buy them one at a time. This will take
me more than 20 days to get set for the construction...”
The findings of the study further describes that, excavation in a rock areas also takes more for people to own a toilet facility. A respondent indicated that “the rocky nature of the land sometimes extend our time period. I am willing to construct the toilet facility but it takes granite before I can successfully dig the hole. This prolongs the time to complete the projects and this motivates us...”
A respondent also indicated “… the time and season can affect their reactiveness to get a toilet facility constructed on time. In the raining season, some of the dug-outs can cave in which will retire the success of the projects and hence more often get demotivated by the raining season…”
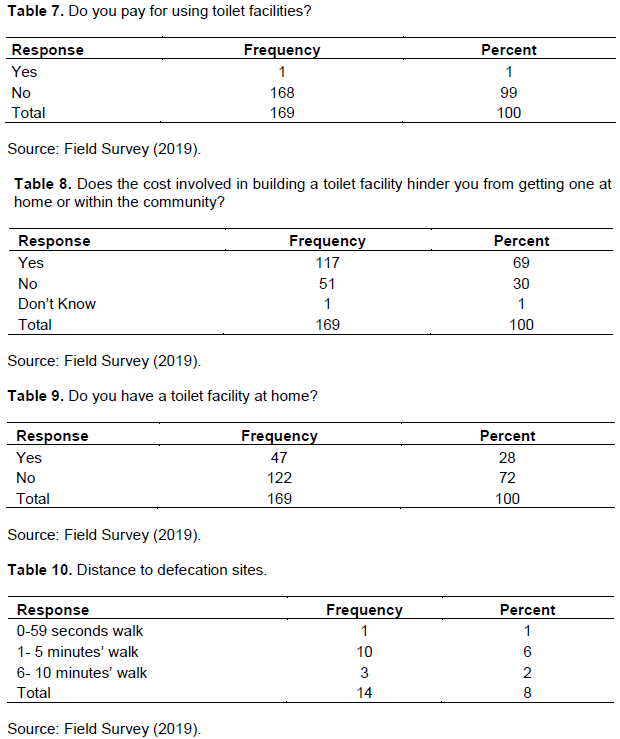
According to Table 7, the findings of the study specify that, majority of the respondent do not pay for access to toilet facility in their community. 99% of the respondents indicated that, they do not pay for access to toilet facility. 6% of the respondents indicated that, they pay for access to the toilet facility. A respondent indicated that “…I pay GHC 0.30p to access the toilet facility of a neighbor. The GHC 0.30p paid covers my two children and wife. My neigbour told me that, in an instance when the toilet becomes full, he will use the money to pay for its discharge…”
The findings of the study specifies that, 69% indicated that, the cost involved in building a toilet facility hinders them from owning a toilet facility. 30% indicated that, the cost do not deter them to construct a toilet facility or own a toilet facility (Table 8).
In a focus group discussion at Somsei Community, a respondent indicated that, “…I am a farmer and I earn less than GHC300.00 a month and I pay for my grandchildren school fees and feeding fees. I cannot afford to construct a toilet facility of my own. Instead of using the money for the toilet construction, I will use the money to cater for the wellbeing of my wards which is paramount to me. Education is the key and I must live to leave a legacy full of promising future”.
A retired head teacher also indicated that,“… the money of yesterday did not have the value to cater for my wards fees and toilet facility. I have six children and the younger one is in senior high school. The education of my wards is very important to me and even though I know the health hazard of the unavailability of toilet, I cannot construct one. I am on retirement; I do not earn any money at the end of the month and hence would find it difficult to pay GHC 1000.00 for the toilet construction...”
Chiefs and opinion leaders in a focus group discussion also indicated that, artisans charge exorbitantly. The study shows that, some of them take more than GHC 1500.00, which discourages the community for the construction of their own toilet facility. “We have directed our members to own their own toilet; however, due to the charges of the artisans we are unable to hold community members”, the Chief of Somsei said.
However, Table 9 indicated that, 28% of the respondents had available toilet facility. 72% of the respondents do not have the toilet facility. Many people who did not have toilet facility indicated the high cost of the toilet building materials and service charge as the main factors that hinders them from acquiring one of their own. The study shows that, 72% people who did not have toilet facility use the free-range system where they explore a bush or in between houses and defecates there. One person defecates on stones while 24 defecate in rubber polythene and either towns or bushes. One person uses flush or pour-flush toilet.
According to Table 10, 6% of the respondents walk less than 5 min to the defecation site. 2% of the respondents walk between 6 and 10 min while 1% uses less than 59 s to visit the defecation site.
The findings of the study reveals that, distance covered to access toilet facility does not trigger them to own a toilet facility. 25% of the respondents were dissatisfied with the distance to defecation site however 75% were satisfied with the distance.
A respondent indicated that, “… I have no option since I cannot own a toilet facility, I am not perturbed. As long as I can get-ride of the faeces I am okay…”
The focus group discussion indicated that, community members enjoy defecating in bushes and love to defecate. They mentioned that, they dot pay for access to an open defecation site and faeces are not seen the next day due to the free ranch of pigs. The pigs eat the faeces and the place is always clean.
Assessment of knowledge base of people on effects of open defecation free (ODF)
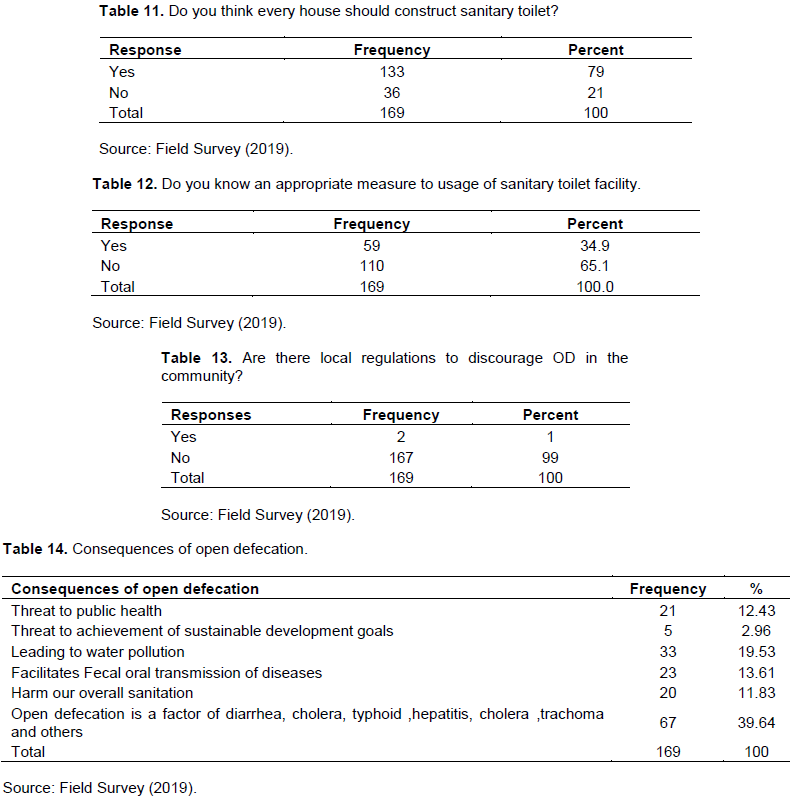
The findings of the study revealed that, 79% of the respondent had adequate knowledge on the advantages of sanitary toilet facility while 21% did not have any knowledge on the importance of sanitary toilet facility (Table 11).
A farmer indicated that “…I spent almost the whole day in the farm. I normally use the open space to defecate and hence do not see the relevance of owning a toilet facility when its usage would be less…”
The findings of the study further established the following significances of sanitary toilet facility during the focus group discussions.
A respondent indicated “…Sanitary toilet facility helps prevent the spread of diseases…” The head teacher of Bebuso Primary School indicated “…The availability of toilets is even shown to increase the school attendance of teenage girls, who may not go to school during their menstrual cycle…”
The WATSAN committee chairperson of Bebuso Community also indicated that “… The waste from infected individuals in the community can contaminate a community’s land and water, increasing the risk of infection for other individuals…”
The District Environmental Health Officer in the Kwahu Afram Plains South District mentioned that“…Without proper sanitation facilities, people often have no choice but to live in and drink water from an environment contaminated with waste from infected individuals, thereby putting themselves at risk for future infection. Inadequate waste disposal drives the infection cycle of many agents that can be spread through contaminated soil, food, water, and insects such as flies…”
The findings of the study describes that, 65% of the respondents know an appropriate measure to use of toilet facility while 35% do not know any measure to ensure sanity at the toilet facility (Table 12).
The study further established that, the 35% were mostly people who defecate in bushes. A respondent indicated that “… I defecate in the bush and in the bush, I do not clean the place. The pigs eat the faeces during the day. So I do not know any measure ensures cleanliness if the toilet facility. The pigs are our cleaners…”
During the focus group discussions, the study further established the following measures from the respondents.
According to a respondent “… Through the intervention of World Vision I participated in a handwashing workshop and I got to know that, one must wash the hands thoroughly after visiting the toilet…” A pupil from Koranteng Primary school indicated “…using liquid soap is a better option than bar soap as the latter could be a source of infection…”
Another respondent also indicated that “…Wash your hands thoroughly with soap every time you use the toilet…”
The findings of the survey describes that, 99% of the respondents indicated that there is no local regulation that discourage open defecation (OD) in the community. 1% of the respondent indicated that, there is a local regulation that restricts open defecation (Table 13).
Findings from the focus group discussion indicated that, majority of the respondents do not have toilet facility and hence practice open defecation and most of the opinion leaders see no problem with it.
An opinion leader indicated that, “… I am aware that open defecation is not good however we cannot restrict members not to defecate in bushes. Community members have complained on the cost of materials and other charges. We therefore became considerate and hence until 20 years to come, I do not think we can restrict members not to defecate in bushes…”
Another opinion leader indicated that, “… I saw the need for a local regulation but sometimes lineage influences the enforcement of the rules. I might not default but my nephew might default and as a leader of the community, I cannot allow my nephew to face the law. I will plead for forgiveness. When this happens, if other family members default I cannot say they should be sanctioned because my nephew was set free...”
The findings of the study further specify that, respondents were guided by set of guidelines that regulates open defecation. The community has restricted members not to defecate openly but rather should join others who have some facilities. However, they have given a year momentum for each household to have a toilet facility. Amidst this, members still defecate openly, the respondents alluded.
The study further maintained that, the byelaws are not enforced since most of the respondents through focus group discussions indicated that, they were not aware of the existence of byelaws.
The findings of the survey describes that, 39.64% believe that open defecation is a factor of a factor of diarrhea, cholera, typhoid, hepatitis, cholera, trachoma and others, 11.83% believes that open defecation is harmful to the Afram Plain District overall sanitation (Table 14).
Some of the views of the participants are reflected in the following quotes “Defecating in the open has been the cause of our illness in our communities. Nowadays it can cause some more health upsets. Open defecation brings about infections. The health consequences of open defecation are many (different diseases) because you do not know people who are infected in area that you want to defecate as well. Most at times has foul stench which is capable of affecting people especially girls. A nurse among the FGD mentioned that, in children, vaginal infections are usually caused by bacteria from the anus. These bacteria may be moved to the vagina when girls, particularly those aged 2 to 6 years, wipe from back to front or do not adequately clean the genital area after bowel movements”.
Another female participant in the FGD also alluded that “I was very weak and did not have appetite for food. I had running stomach at dawn so they took me to the health center in this community. We were told that what brought about it is open defecation. It was then that I realized that, all these mosquitoes, when they perch on the faces, they will carry around and when they touch us or our food, it causes running stomach.