ABSTRACT
This study evaluated the health impacts of WASH interventions in 9 intervention communities against 9 control communities in disaster-prone areas in northern Ghana. We extracted community-specific data on patient-reported cases of WASH-related diseases from health facilities in the study areas. Also, we used key informant interviews and household questionnaires to seek information for validation. The impact was measured using the before-after study with concurrent control (BAC) method of Health Impact Evaluation in WASH interventions. The findings indicate a substantial increase in the number of WASH facilities across the intervention communities. However, some respondents complained of access to inadequate quantities and increase downtime of water systems when there is a breakdown. Access to improved sanitation facilities was still a challenge, although a steady increase in the number of household access to latrines was observed. We extracted about 2,315 reported cases of WASH-related diseases, comprising diarrhoea (83%), dysentery (8%), typhoid fever (7%) and intestinal worms (2%). Impacts on diarrhoea prevalence were generally lower than reported figures, and varied across the intervention communities, ranging from 0 to 7% reduction. We recommend that greater attention be given to the sustainability of the intervention to ensure service delivery, rather than as a one-time investment, to achieve more significant impacts.
Key words: Disaster-prone communities, WASH, sanitation, public health.
Typical environmental disasters in Ghana include droughts, epidemics, floods and wildfires. However, floods account for about one-third of all disaster-related deaths in the country (WHO, 2017). In the three (3) northern regions of Ghana, disasters significantly impact vulnerable populations in disaster-prone areas and may lead to unnecessary losses in social and economic capital. In particular, recurrent flooding events, which are the most pervasive in terms of financial damages and the number of people affected, usually result in the disruption of services
from water, sanitation and hygiene (WASH) facilities (Care Nederland, 2012). Such occurrences could lead to significant damages to property and trigger other emergencies such as the outbreaks of water-borne/related diseases (e.g. diarrhoea, cholera and malaria). Consequently, there is a reduction in productivity, economic losses and social pressures.
Ensuring quality of water supply (during collection, handling, storage, and use), and the maintenance of proper sanitation and hygiene practices after such flooding events also presents immense challenges to the health of these communities. Rehabilitation costs are usually high and unaffordable, leading to a drastic fall in the living conditions and opportunities for future development in the affected communities. The situation is exacerbated in communities where there is a lack of WASH facilities and services. In such circumstances, the challenges include the prevalence of water-borne, vector-borne and sanitation-related diseases as a result of poor drinking water quality, inadequate sanitation and poor hygiene and women, children and the youth are the most affected. Over the years, flooding and its devastating effects have been the narrative of the three (3) northern regions of Ghana.
Impact of WASH interventions on public health
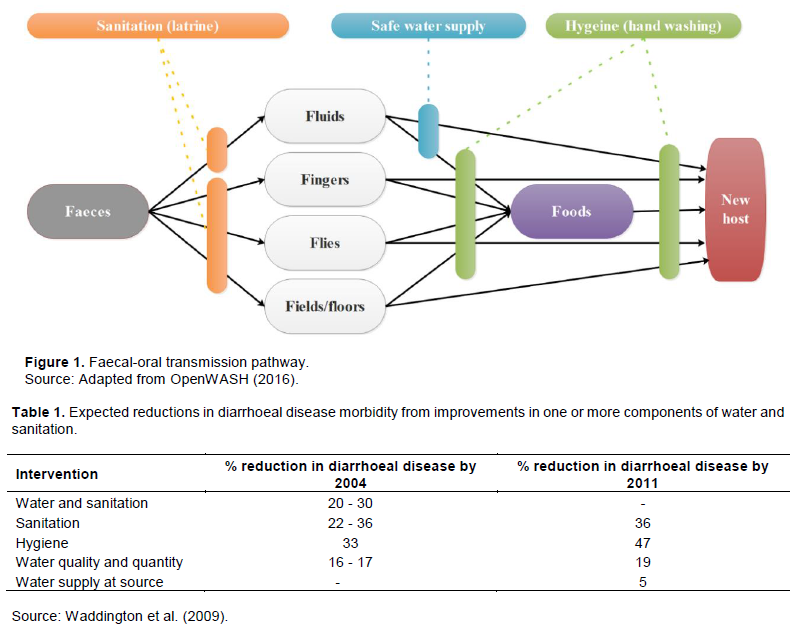
The vital role of WASH in maintaining health has long been recognized, considering the critical role it plays in reducing illness and death from infectious diseases (McKeown and Record, 1962). Diarrhoea and selected parasitic diseases have been identified to be among the major diseases related to WASH. Infectious diarrhoea is probably the largest contributor to the disease burden from WASH (Prüss et al., 2002). The infection results from the ingestion of faecal contaminated fluids or foods, through various faecal-oral transmission pathways, as illustrated in Figure 1, is facilitated by poor WASH practices. Moreover, globally, diarrhoea is the second leading cause of mortality in children under the age of five (5), excluding pre-term birth complications (Liu et al., 2012). Diarrhoeal diseases, acute respiratory tract infections, cholera, Shigella dysentery, viral hepatitis A and diphtheria are the most common cause of death in emergencies associated with poor WASH services. However, all these causes of death are preventable. From the health perspective, improving access to safe water supply and sanitation services is a preventive intervention, whose primary outcome is a reduction in the number of episodes of diarrhoea and, accordingly, a proportionate decrease in the number of deaths (WHO, 2004). WASH interventions, such as the provision of clean piped drinking water, enhanced facilities for excreta disposal and the promotion of handwashing with soap at critical times, improve health and reduce infectious disease incidence (Burger and Esrey, 1995; Dangour et al., 2013; Esrey et al., 1991; Laxminarayan et al., 2006; WHO, 2004; WHO and UNICEF, 2014).
Table 1 presents percentage reductions in diarrhoea incidence estimated from pooled analyses for water supply at source, water quality interventions, sanitation interventions and hygiene (handwashing with soap at critical times). Esrey et al. (1991) examined the impact of improved water supply and sanitation facilities. They reported significant reductions in morbidity for diarrhoea (26%), trachoma (27%), ascariasis (29%), schistosomiasis (77%) and dracunculiasis (78%). Similarly, by improving water supply and excreta disposal, the median reduction of 22% in diarrhoea morbidity rate has been reported (Burger and Esrey, 1995). The authors, however, stated that the magnitude of this reduction might vary depending on several factors such as age, type of service provided and the general living conditions of people. Furthermore, a systematic review and meta-analysis of WASH interventions to reduce diarrhoeal illness in less developed countries found a strong consistency in the effectiveness of the interventions (Fewtrell et al., 2005). Moreover, other scholars have maintained that sanitation and hygiene promotion are still the two most effective interventions for controlling endemic diarrhoea (Laxminarayan et al., 2006). A study conducted by the WHO found that using an improved water source reduces diarrhoeal disease risk by 24 to 73% (WHO, 2004). A meta-regression based on a single study by the WHO suggested that enormous health benefits could be gained by transitioning from basic on-site piped water to systematically managed water, with significant reductions in diarrhoea ranging from 73 to 79%, depending on baseline condition (WHO and UNICEF, 2014). A review by Mills and Cumming (2016)demonstrated that there is good evidence that poor WASH contributes to the majority of the burden of diarrhoea and related adverse health effects, and strong consensus around this point. The review further reported that there is suggestive evidence that increasing water quantity directly reduces the risk of diarrhoea and other WASH-related diseases. In spite of the aforementioned correlation between WASH interventions and public health, Care Nederland (2012)cautions that other factors may mask the expected outcome of WASH interventions (e.g. the provision of flood-resilient WASH facilities), especially in disaster-prone areas.
WASH intervention in disaster-prone communities in northern Ghana
In a bid to reduce the burden of the yearly flooding on improved WASH facilities in the northern part of Ghana, the WASH in Disaster Prone Communities (DPC) programme was designed to improve sustainable access to disaster-resilient WASH facilities in 265 communities in 24 districts. At the community level, the objectives of the programme included the provision of flood resilient improved water and sanitation facilities (for households and schools) and the promotion of behaviour change towards proper WASH practices through educational campaigns (UNDP, 2019). The programme covered 200,000 people, 25% of them being school children, in Disaster Prone Communities (DPC) in the Upper East, Upper West and Northern regions of Ghana. It was a collaboration between both international and local stakeholders, namely the UN-Habitat, UNDP, UNICEF and WHO, with support from Government partners in the WASH sector, as well as the private sector and non-governmental organizations. One of the expected outcomes of the programme was the reduced burden of WASH-related diseases among men, women, boys and girls in disaster-prone communities in the three (3) regions of northern Ghana.
According to WHO (2017), the WASH in DPC Programme had already achieved tangible results after more than two (2) years of implementation. It was on track to deliver the expected outcomes in terms of access to resilient water and sanitation systems for the targeted population across the three regions of northern Ghana.
This study evaluated the health impact of the WASH intervention in the DPCs. Specifically, this research (1) assessed the impact of the WASH in DPC Programme by collating and analysing health data at the sub district; (2) gathered scientific evidence from previous and ongoing epidemiological studies to support the main objective of the assessment; and (3) highlighted recommendations for similar future programmes.
Study design
This study used both qualitative and quantitative methodologies. The study encompassed nine (9) districts, comprising three (3) districts in each of the three (3) study regions. In each district, two (2) communities (1 intervention and 1 non-intervention) were selected. The study communities were chosen on the basis of the availability of a community-based health facility (e.g. Community-based Health and Planning Services (CHPS) Compound or Health Centre). This was to help minimize the complexities associated with the evaluation of the outcomes of the interventions in these communities in relation to reported cases of WASH-related diseases.
The before-and-after study with concurrent control (BAC) method was used to evaluate the impact of the WASH intervention. In BAC studies, the pre- and post-intervention results of two groups (the experimental or intervention group and the control group) are compared to measure the effectiveness of an intervention (Mahajan, 2015; Robson et al., 2001; Schmidt et al., 2011). As noted by Robson et al. (2001), the intrinsic validity of the before-and-after method may be threatened by several factors (e.g. significant external influences other than the intervention, the Hawthorne effect, maturation effect, placebo threat, regression-to-the mean, etc.); however, it can be useful in providing preliminary evidence of the effectiveness of an intervention. Shadish et al. (2002)noted that the plausibility of results from the BAC method depends on (1) the similarity of the intervention and control cluster (a set of households), and (2) the observed disease trend. Thus, in this study, clusters in the intervention and control communities were randomly allocated to ensure similarity between the intervention and control communities. By a rigorous cluster randomized design, we selected both the intervention and control clusters for the study. In all, nine (9) each of the intervention and control clusters were chosen for the study. Once an intervention cluster was selected, a community from an enumerated list was selected randomly. To select control clusters, each intervention sub-district where a cluster was chosen, was then matched to a control cluster, considering the local geography, hydrogeology, infrastructure, agricultural productivity, and household construction. Once a control cluster was selected, a community from an enumerated list of the communities was selected randomly.
The changes in the prevalence of WASH-related diseases such as diarrhoea, cholera, diphtheria, dysentery, typhoid and worm infections (that is, helminths) are key indicators used to determine the impact of WASH intervention on health (Ramesh et al., 2015). Therefore, this study used data on reported cases of theses WASH-related diseases in the health facilities in the study communities.
Profile of study areas
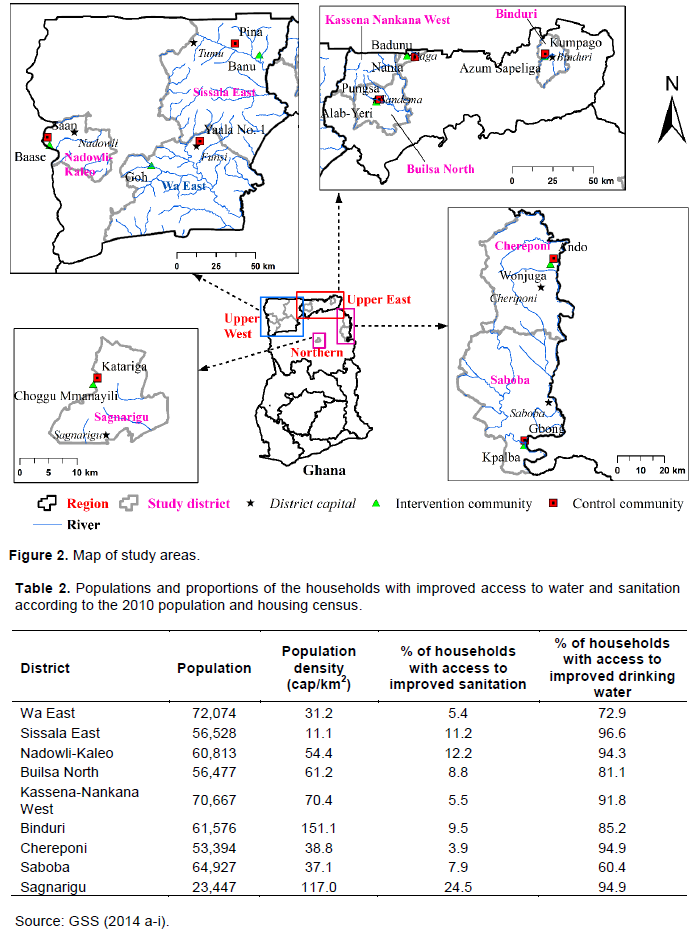
Figure 2 shows the locations of the districts and communities selected for the study. Available data on the demographic and socioeconomic characteristics are aggregated at the district and regional levels. According to the district analytical reports of the 2010 population and housing census, the population of the study districts is dominated by females, averaging 51.5%, with the remainder being males. Generally, the majority (81.2-100%) of the population in the districts live in rural areas. Agriculture is the main economic activity in the study regions, serving as the source of livelihood for over 75% of the population. Among the economically active class, the unemployment rate is higher among females (3.0%) as compared to males (2.5%).
Though access to improved sources of drinking water is relatively good (60.4-96.6%), the case for sanitation is poor (3.9-24.5%), as presented in Table 2. This observation is similar to the national trend (Appiah-Effah et al., 2019). A large proportion (mostly > 80%) of the population across the districts practices open defecation due to the lack of access to toilet facilities. The three regions in northern Ghana lie in and are drained by the Volta River System (White Volta, Black Volta and the Oti rivers).
Data collection and analysis
Four (4) different methods were used in the collection of data: document review, collation of data from health facilities, key informant interviews, and household survey. The document review involved a desktop review of all available project deliverables, reports and the literature on the WASH on the DPC programme. Pre- and post-intervention data on reported cases of the indicator diseases, for both the intervention and control populations, were collated for the analysis. Semi-structured questionnaires were used for the household surveys and key informant interviews. The key informants included opinion leaders, school officials, health officials and environmental health officers (EHOs). The information from the variety of stakeholders was to verify and improve the reliability of the findings from the medical records.
The collated data were organized and analyzed in Microsoft Excel. The health impact of the intervention was evaluated using the BAC method of Health Impact Evaluation in WASH interventions. In this study, we focussed on the first four indicator diseases with the most reported cases. The most prevalent indicator disease, among the four, was then selected for further analysis. By difference-in-difference (DID) analysis (Schmidt et al., 2011)of both the intervention and control communities, the effect of the intervention was estimated.
General disease trends and the basis for selection of outcome disease for impact analysis
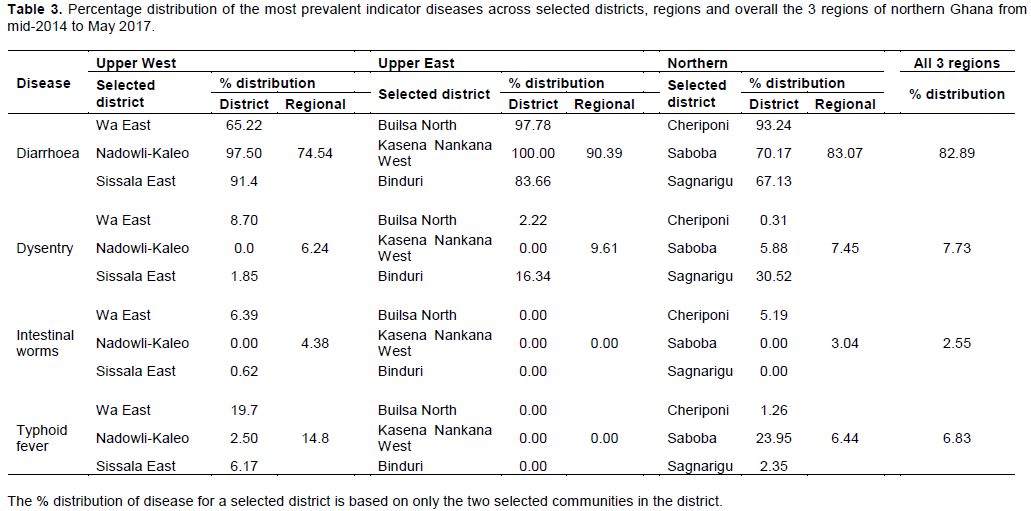
From the data gathered from the various health facilities, diarrhoea, dysentery, intestinal worms, and typhoid diseases were the WASH-related diseases reported. A total of 2,315 reported cases of these diseases were recorded in the 3 study regions from the middle of 2014 till the time of visit (May 2017). Of the 2,315 reported cases, about 83% were diarrhoeal illness, 8% dysentery cases, 7% typhoid cases and 2% intestinal worm cases. Table 3 shows the percentage distribution of these diseases across the selected districts, regions and overall, the 3 regions put together. Diarrhoea was the most prevalent WASH-related disease among the four diseases. Therefore, in proceeding with further analysis of the impact of the interventions, diarrhoea disease was used as the outcome measure. This was to make the results more plausible as compared to using other disease outcomes.
Diarrhoea disease trend by age and sex
Of the 82% diarrhoea cases, children aged up to 5 years constituted 56% while those above 5 years accounted for 26%. Also, 64% of reported WASH-related diseases were children less or equal to 5 years, whereas 36% were above 5 years. Females had a higher prevalence of diarrhoea (54%) as compared to males (46%) from the study.
Health impact analysis of WASH interventions on a community by community basis
Here, compares the trends in disease prevalence between the intervention community and the control community.
Wa East district (Goh and Yaala No. 1)
The Goh community had two boreholes fitted with hand pumps, which served as the only source of water for domestic use. Water from these boreholes was available all year round unless there was a mechanical breakdown, which does not take long to fix (usually within two weeks). Regarding sanitation and hygiene facilities, households had built traditional pit latrines with tippy-tap for hand washing (Figure 3). However, in the control community, Yaala No. 1, households used water from unlined communal hand-dug wells, which were reported to have inadequate yield and usually dried up during the dry season. A nearby river served as an alternative source of water for domestic use. There was also the practice of open defecation in the community. The result from the study showed a decline in diarrhoea prevalence for Goh from 6 to 4% with no change in the prevalence (10%) for Yaala No.1 during the same period (Figure 4a). This gave a calculated DID of 4%, suggesting a 4% reduction in diarrhoea prevalence in Goh by the intervention (Figure 5). The reported positive impact could be as a result of the access to improved WASH facilities by households. Also, as revealed by discussions with opinion leaders, the frequent and vigorous WASH education carried out by the EHOs assigned to the community gives credence to the observed trend. This was also confirmed by the EHO attached to the team, who indicated that Goh was soon to be declared ODF after the verification process.
Nadowli-Kaleo district (Baase and Saan)
Baase community had two boreholes that were constructed in 2016. Hitherto this, they used water from a nearby river for domestic activities. Households reported that the yield of the boreholes was inadequate; hence, they resorted to a nearby river. With regards to sanitation facilities, households had constructed traditional pit latrines with tippy-tap after they were triggered under a Community-Led Total Sanitation (CLTS) programme undertaken in the community. Saan, on the other hand, had one borehole, which was reported to be unreliable. Moreover, households in Saan reported the use of a communal toilet facility, which has no handwashing facility.

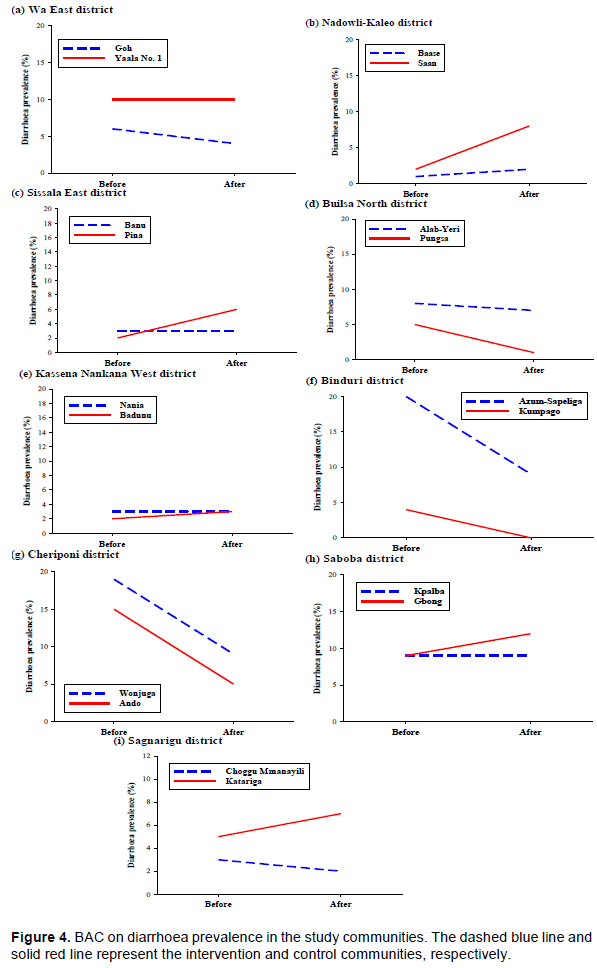
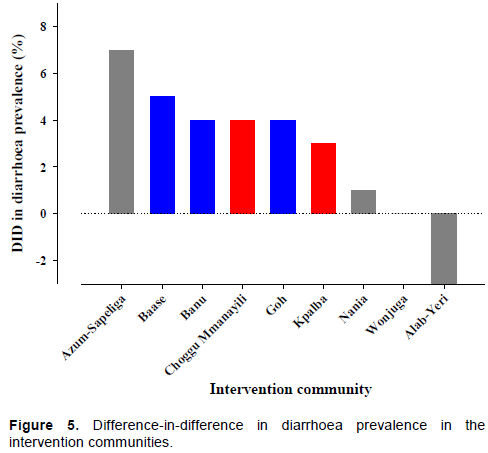
In the case of Baase, there was a slight increase in the prevalence of diarrhoea from 1 to 2% over the period. For Saan, diarrhoea prevalence increased from 2 to 8% (Figure 4b). This gives a calculated DID of 5%, indicating that the impact of the intervention is a 5% reduction in diarrhoea prevalence in Baase (Figure 5). The vigorous implementation of the CLTS approach carried out in the community could have partly contributed to the positive impact observed in the Baase community. This was seen in the reported increased access to improved water (borehole) coupled with an increased number in the construction and use of household toilet facilities.
Sissala East district (Banu and Pina)
There were three boreholes constructed in Banu, but only one was functional at the time of the assessment, serving as the only improved source of water for domestic use. The respondents indicated that one borehole was highly inadequate, compelling them to resort to the River Kaalon as an alternative water source. Banu had also been declared as an ODF community. The majority of households have constructed their latrines. The Pina community has only one borehole located close to its CHPS compound, and this was reported to be inadequate. This was evident by the long queues observed at the water point at the time of the visit. Households used a nearby river as an alternative source. In the case of sanitation, the majority of households in Pina did not have household latrines and practised open defecation.
In Banu, diarrhoea prevalence showed an almost steady scenario of 3% over the period. The results for Pina also showed an increase in diarrhoea prevalence from 2 to 6% (Figure 4c). This gives a calculated DID of 4%, suggesting that the impact of the intervention is a 4% reduction in diarrhoea prevalence in Banu (Figure 5). Efforts made at obtaining ODF status could be a major indicator of gains made in Banu. As expected, diarrhoea prevalence was lower in Banu as compared to Pina.
Builsa North district (Alab-Yeri and Pungsa)
Although Alab-Yeri was a DPC community, it was reported that no infrastructure had been provided under the project at the time of the visit. However, there existed two boreholes and one unprotected hand-dug well in the community. The two boreholes had been constructed for the school and CHPS facility, respectively. The community depends on the hand-dug well as a source of water for domestic use. The hand-dug well dries up during the dry season; hence, households compete with pupils for the use of the school’s borehole. Moreover, households did not have latrines and resorted to open defecation. Pungsa, on the other hand, reported inadequate potable water and low sanitation coverage.
Diarrhoea prevalence in Alab-Yeri dropped slightly from 8 to 7% over the period. Pungsa, on the otherhand, had an decrease in diarrhoea prevalence from 5 to 1% (Figure 4d). This gives a calculated DID of -3% (Figure 5), suggesting that there has been no impact (no effect) of the WASH in the DPC programme in Alab-Yeri. The negative impact (no effect) of the project in Alab-Yeri could be because the implementation of facilities had not begun as of the time of the assessment. Therefore, the downward trend observed could not be attributed to the WASH in DPC programme but other factors that may include other interventions.
Kassena Nankana West district (Nania and Badunu)
Nania has two boreholes that were reported to yield water all year round, but they experience mechanical breakdowns from time to time. There are also some hand-dug wells as alternatives. Households have also constructed latrines. Though households reported they practice handwashing after using the toilet, we observed no handwashing scheme attached to the latrines. Badunu, the non-intervention community, also had limited access to both improved water and household toilet facilities.
The diarrhoea prevalence for Nania showed a steady trend of 3% over the period. However, Badunu showed a slight increase from 2 to 3%. (Figure 4e). The calculated DID, therefore, 1% (Figure 5), inferring that the impact of the intervention was only a 1% reduction in diarrhoea prevalence in Nania. The relatively low impact of the programme, despite the availability of the boreholes, could be attributed to the reported long walking distances to the water points and frequent breakdown of the boreholes. Due to this challenge, it was reported that households were unable to fetch adequate quantities for their daily use. Also, most households had no latrines, while those who had, had no handwashing facilities. Such conditions could result in faeco-oral transmission, hence the low impact.
Binduri district (Azum-Sapeliga and Kumpago)
Azum-Sapeliga has benefited from 3 boreholes from the programme; however, at the time of the visit, one of them was non-functional. Households reported that potable water was not adequate. Also, households had constructed latrines with tippy tap and ash for hand washing. Households indicated their preference for soap over ash, most of them had resorted to the latter due to financial reasons after a campaign was undertaken by UNICEF on handwashing with soap and water. The non-intervention community, Kumpago, also had limited access to improved water facilities, with the majority of households also not having access to improved household toilets.
The results showed a steady decrease in diarrhoea prevalence from 20 to 9% in Azum-Sapeliga over the period. Kumpago also showed a decline in diarrhoea prevalence from 4 to 0% (Figure 4f). The estimated impact of the intervention based on the DID was relatively high in Azum-Sapeliga: diarrhoea prevalence reduced by 7%. It is worth mentioning that in this community, the chief was actively involved in rallying community members to improve upon the WASH situation in the community.
Cheriponi district (Wonjuga and Ando)
The results gathered showed an increase in the number of WASH facilities in Wonjuga after the intervention. At the time of the study, the community had three functional and two non-functional boreholes fitted with hand-pump, which are used by households for various domestic activities. The respondents indicated access to adequate improved water supply. A significant number of inhabitants had household latrines, which were mainly traditional pit latrines. On the other hand, Ando, the non-DPC, had only one functional borehole, which all households depended on for water for domestic use. Although some households have traditional pit latrines, the number observed was inadequate and hence, the majority of the population practised open defecation.
Although Wonjuga showed a decline in diarrhoea prevalence from 19% to 9% over the period, Ando also had the same percentage drop in prevalence (15 to 5%), as shown in Figure 4g. Thus, the calculated DID was 0%, indicating that the trend in Wonjuga would have remained the same without the intervention (the no effect situation). The trend observed in Wonjuga and Ando suggests that these two communities are quite homogeneous. The similar trend may also be attributed to the WASH interventions which took place in the control community (Ando) earlier. The community reported benefitting from hygiene education by environmental health officers. Hence, both communities have been sensitized on proper WASH practices and how to prevent diarrhoea diseases.
Saboba district (Kpalba and Gbong)
There were only two functional boreholes fitted with hand-pump in the Kpalba community, although it was an intervention community. Access to boreholes fitted with hand-pump was found to be limited according to the qualitative study from the households. Households, therefore, accessed surface water from the River Oti for their daily domestic chores. Prior to the installation of the boreholes with hand-pumps, residents in Kpalba relied on unimproved water sources. Although the community had benefitted from the CLTS approach in creating demand for household latrines, uptake was observed to be very low. Gbong, as the non-intervention community, also had limited access to improved water facilities, with the majority of households also not having access to improved household toilets.
Diarrhoea prevalence for Kpalba showed a steady trend of 9%, while Gbong showed an increase of 9 to 12% (Figure 4h). The calculated DID was 3%, which inferred that the impact of the intervention reduced diarrhoea prevalence in Kpalba by 3%.
Sagnarigu district (Choggu Mmanayili and Katariga)
In Choggu Mmanayili, a small-town water supply scheme with standpipes has been constructed from which households access water for domestic activities. According to the households, the water is available all year round. Household use either self-constructed or communal latrines. Households also reported that WASH awareness campaigns had been organized by the UN-Habitat and World Vision, which, in their view, had brought improvement to their health status. Katariga, the non-intervention community, also had limited access to improved water facilities, with the majority of households also not having access to improved household toilets.
Over the period, diarrhoea prevalence in Choggu Mmanayili slightly decreased from 3 to 2%, whereas it increased from 5 to 7% (Figure 4i) in Katariga, resulting in a DID of 4%. Hence, the impact of the intervention in Choggu Mmanayili was a 4% reduction in diarrhoea prevalence. Choggu Mmanayili could be described as peri-urban and close the capital town of the region, Tamale. Therefore, the inhabitants of Choggu easily benefit from sensitization programmes on the benefits of proper WASH practices. Hence, the facilities provided are used, and the benefits derived as shown by the analysis.
Diarrhoea was the most prevalent WASH-related disease in the study communities, as it accounted for over 80% of the reported WASH-related cases. This finding agrees with the global level report by Prüss et al. (2002). Moreover, children less than five years were the most affected as they constituted the majority (56%) of the cases. Interviews with health officers confirmed these results. They indicated that children from early birth through age 5 were the most affected by diarrhoea. Further to this, the health officers acknowledged the relationship between the availability and use of improved WASH facilities and diarrhoea. However, they emphasized that it was not the sole cause of childhood diarrhoea. The result is consistent with the report by the Ghana Demographic and Health Survey (GSS et al., 2015), which indicated that diarrhoea prevalence is high among children below 5 years since they are at increased risk of contamination from the environment. Compared to age, the difference in diarrhoea prevalence by sex was relatively small. The study results, however, contradicted that of the GSS et al. (2015), which reported that diarrhoea prevalence was higher in males (52%) than in females (48%).
The reduction of diarrhoea prevalence as a result of the WASH intervention varied across the intervention communities, ranging from cases of no impact to a 7% reduction (Figure 5). The highest percentage reduction (7%) was observed in Azum-Sapeliga, a community in which the chief actively participated in promoting proper WASH practices. Due to the large difference in the diarrhoea prevalence at baseline, it could be argued that factors other than the intervention, such as maturation effect (socioeconomic development), might have significantly contributed to the observed difference (Schmidt et al., 2011; Shadish et al., 2002). However, we posit that the active participation of the chief of the community in promoting proper WASH practices cannot be overlooked and might have contributed significantly to the relatively high impact of the programme observed. Thus, we recommend that getting the active support of opinion leaders must be a priority to ensure the success of intervention programmes. Similarly, in Baase, the active involvement of the community members through the CLTS resulted in quite a substantial decrease in diarrhoea in the community.
Moreover, the 0-7% reductions in diarrhoea prevalence observed were low compared to what is reported in the literature. For instance, a review by Wolf et al. (2014), which included a meta-analysis 61 studies, suggests that water and sanitation interventions could reduce diarrhoea prevalence by 34 and 28%, respectively. The low levels of reductions in diarrhoea prevalence observed in this study could partly be because diarrhoea has many causes for which improved water, sanitation and hygiene only constitute some of the many sources of infection. Also, the neglect of the WASH interventions as a result of them not working, broken down or underused will probably result in a small impact. We argue that separating WASH as independent interventions in health impact analysis is not necessarily helpful, as they act upon interlinked transmission pathways, and often cannot be provided in isolation from each other. Care Nederland (2012)also noted that although ensuring WASH facilities are more flood-resilient can reduce how vulnerable communities, it is important to recognize that many other factors can limit the impact of the intervention.
Furthermore, behavioural factors play an essential role in determining the uptake and sustainable adoption of WASH technologies and practices. While WASH interventions are potentially highly efficient, their effectiveness in part depends on behaviour change and context. The installation and functioning of water and sanitation facilities need to be accompanied by the transfer of knowledge on how to use them, together with sustainable behaviour change (Waddington et al., 2009). Maintenance and periodic replacement of existing services/facilities and hygiene promotion are also necessary to achieve improvements (Bartram and Cairncross, 2010).
From the findings of the study, we recommend that more considerable attention should be given to the sustainability of the intervention (especially, the technical and financial aspects), rather than as a one-time investment, to ensure service delivery to achieve more significant impacts. Also, the CLTS approach should focus on triggering households to construct their latrines and hygiene facilities around the same time as the provision of the water facilities. Moreover, households should be encouraged to continue the use of WASH facilities at critical seasonal periods; for example, rainy seasons, where households use rainwater for most of their domestic activities, including cooking and drinking. In addition, since the provision of water, sanitation and hygiene facilities do not solely impact on diarrhoea, and other WASH-related diseases, the intervention should be packaged such that it incorporates other aspects of environmental sanitation such as wastewater, solid waste and faecal sludge management. Furthermore, the project should ensure the establishment of strong and coherent databases to enhance impact evaluation and sustainability analysis. Finally, rigorous studies should be conducted besides measuring coverage and prevalence of diarrhoeal and other WASH-related disease rates. Monitoring and evaluation of interventions should focus on other socio-cultural, economic and environmental conditions.
The qualitative and quantitative findings of the assessment agree that there has been a substantial increase in the number of water, sanitation and hygiene facilities across the intervention communities. The results indicate that interventions are needed to improve the quality of service delivery for water, sanitation and hygiene, particularly for deprived communities, including DPCs. Access to improved water sources increased considerably over the past two years of the intervention. Despite the increase in water facilities, a section of the respondents complained of poor water quality, access to inadequate quantities and increased downtime when there is a breakdown. Households, therefore, supplement water demand with unimproved sources such as river, stream, dams and rainwater, compromising the health benefits of the intervention. Access to improved household latrines was still a challenge, although the study acknowledges the steady increase in the number of household access to latrines. All this progress was noted with some level of satisfaction by many of the households and key informants interviewed.
Diarrhoea was the most prevalent WASH-related disease identified in the study communities. Evidence from this study also shows that the WASH interventions have made an impact on the reduction of diarrhoeal diseases. However, the extent of reduction (up to 7%) was low compared to that of other studies (over 20%). This indicates that some level of reduction in diarrhoeal diseases can be expected from sustainable investments in water, sanitation and hygiene interventions. That notwithstanding, the study could not measure the extent to which water, sanitation and hygiene independently contributed to the reduction in diarrhoeal diseases since it could not gather detailed information on the quality of service delivered by either water, sanitation or hygiene.
The authors have not declared any conflict of interests.
This research was supported by the World Health Organization (WHO), Ghana under the WASH in Disaster Prone Communities (DPC) Programme
REFERENCES
|
Appiah-Effah E, Duku GA, Azangbego NY, Aggrey RK, Gyapong-Korsah B, Nyarko KB (2019). Ghana's post-MDGs sanitation situation: An overview. Journal of Water, Sanitation and Hygiene for Development 9(3):397-415.
Crossref
|
|
|
|
Bartram J, Cairncross S (2010). Hygiene, sanitation, and water: forgotten foundations of health. PLoS Med 7(11): e1000367.
Crossref
|
|
|
|
|
Burger SE, Esrey SA (1995). Water and sanitation: Health and nutrition benefits to children. In: Child growth and nutrition in developing countries: Priorities for action. pp. 153-174.
|
|
|
|
|
Care Nederland (2012). Techniques to improve the resilience of community WASH systems in flood-prone areas.
|
|
|
|
|
Dangour A, Watson L, Cumming O, Boisson S, Che Y, Velleman Y, Cavill S, Allen E, Uauy R (2013). Interventions to Improve Water Quality and Supply, sanitation and Hygiene Practices and Their Effects on the Nutritional Status of Children. In Child Growth and Nutrition in Developing Countries: Priorities for Action, edited by P Pinstrup-Andersen, A Pelletier, A Alderman 8:153-75. Cornell University Press.
Crossref
|
|
|
|
|
Esrey SA, Potash JB, Roberts L, Shiff C (1991). Effects of improved water supply and sanitation on ascariasis, diarrhea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull WHO, 69:609-621.
|
|
|
|
|
Fewtrell L, Kaufmann RB, Kay D, Enanoria W, Haller L, Colford Jr JM (2005). Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis. The Lancet Infectious Diseases 5(1):42-52.
Crossref
|
|
|
|
|
Ghana Statistical Service (GSS) (2014a). 2010 population and housing census: District analytical report, Binduri district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014b). 2010 population and housing census: District analytical report, Builsa North district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014c). 2010 population and housing census: District analytical report, Chereponi district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014d). 2010 population and housing census: District analytical report, Kassena Nankana West district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014e). 2010 population and housing census: District analytical report, Nadowli-Kaleo district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014f). 2010 population and housing census: District analytical report, Saboba district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014g). 2010 population and housing census: District analytical report, Sagnarigu district. Accra, Ghana.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014h). 2010 population and housing census: District analytical report, Sissala East district.
|
|
|
|
|
Ghana Statistical Service (GSS) (2014i). 2010 population and housing census: District analytical report, Wa East district. Accra, Ghana.
|
|
|
|
|
GSS, GHS, ICF International (2015). Ghana Laxminarayan demographic and health survey 2014. Rockville, Maryland, USA.
|
|
|
|
|
Laxminarayan R, Mills AJ, Breman JG, Measham AR., Alleyne G, Claeson M, Jha P, Musgrove P, Chow J, Shahid-Salles S, Jamison DT (2006). Advancement of global health: Key messages from the Disease Control Priorities Project. Lancet 367(9517):1193-1208.
Crossref
|
|
|
|
|
Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn J, Rudan I, Campbell H, Cibulskis R, Li M, Mathers Black RE (2012). Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet, May.
Crossref
|
|
|
|
|
Mahajan A (2015). Limitations of CBA study: Controlled before after study. Lung India 32(6):670-671.
Crossref
|
|
|
|
|
McKeown T, Record RG (1962). Reasons for the decline of mortality in England and Wales during the nineteenth century. Population Studies 16(2):94-122.
Crossref
|
|
|
|
|
Mills JE, Cumming O (2016). The impact of water, sanitation and hygiene on key health and social outcomes: Review of evidence. Retrieved from View
|
|
|
|
|
OpenWASH. (2016). Ethiopia's One WASH National Programme. Retrieved from
View
|
|
|
|
|
Prüss A, Kay D, Fewtrell L, Bartram J (2002). Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environmental Health Perspectives 110(5):537-542
Crossref
|
|
|
|
|
Ramesh A, Blanchet K, Ensink JH, Roberts B (2015). Evidence on the effectiveness of water, sanitation, and hygiene (WASH) interventions on health outcomes in humanitarian crises: A systematic review. PLoS ONE 10(9):e0124688.
Crossref
|
|
|
|
|
Robson LS, Shannon HS, Goldenhar LM, Hale AR (2001). Guide to Evaluating the Effectiveness of Strategies for Preventing Work Injuries. NIOSH.
|
|
|
|
|
Schmidt WP, Norman G, Cumming O (2011). Evaluating the health impact of urban WASH programmes: An affordable approach for enhancing effectiveness (No. DP#001). Retrieved from
View
|
|
|
|
|
Shadish WR, Cook TD, Campbell DT (2002). Experimental and Quasi-Experimental Designs for Generalized Causal Inference (2nd ed.). Boston: Houghton Mifflin Company.
Crossref
|
|
|
|
|
UNDP (2019). Water, sanitation and hygiene in disaster prone communities in Northern Ghana: Consolidated final narrative report.
|
|
|
|
|
Waddington H, Snilstveit B, White H, Fewtrell L (2009). Water, sanitation and hygiene interventions to combat childhood diarrhoea in developing countries. New Delhi: International Initiative for Impact Evaluation.
|
|
|
|
|
World Health Organization (WHO) (2004). Comparative quantification of health risks. Geneva.
|
|
|
|
|
World Health Organization (WHO) (2017). Terms of reference - End of project evaluation: for the assessment of health impact of WASH intervention in WASH in DPC Communities, Northern Ghana, Ghana.
|
|
|
|
|
WHO UNICEF (2014). Progress on Drinking Water and Sanitation - 2014 Update. Switzerland.
|
|
|
|
|
Wolf J, Prüss-Ustün A, Cumming O, Bartram J, Bonjour S, Cairncross S, Clasen T, Colford JM, Curtis Jr V, De France J, Fewtrell L, Freeman MC, Gordon B, Hunter PR, Jeandron A, Johnston RB, Mäusezahl D, Mathers C, Neira M, Higgins JP (2014). Assessing the impact of drinking water and sanitation on diarrhoeal disease in low-and middle-income settings: A systematic review and metaregression. Tropical Medicine and International Health 19(8):928-942.
Crossref
|
|