Understanding content of bottom ashes from incinerator especially toxic heavy metals is an important step towards ash utilization. The aim of this paper was to evaluate heavy metals levels of in bottom-ash from hospital waste incinerators in four different hospitals in Dar es Salaam city (Muhimbili National Hospital and three regional referral hospitals Mwananyamala Ilala and Temeke) in Dar es Salaam city, Tanzania. It has been estimated that Tanzania has an average annual generation of healthcare waste of 6,745 tons per year with a generation rate of about 0.41 kg/occupied bed/day of healthcare waste. Burning of hospital waste releases toxic metals in the bottom ash which can pollute the environment if not well managed. The samples were collected from a pile of bottom ash, according to Standard Guide for sampling waste piles ASTM D6009-96, digested with a 3:1 of concentrated acids HNO3 and HClO4. The concentration of heavy metal were determined using Inductively Coupled Plasma-Optical Emission Spectrometer (ICP-OES). The maximum concentration of other metals were 0.348 ± 0.161 Cr (Ilala Regional Hospital), 0.019 ± 0.012 Cd (MNH) and 0.677 ± 0.499 Pb (Ilala Regional Hospital). The level of metals determined exceeded the US-EPA regulation maximum permissible limit in good soil quality and therefore classified as harmful and toxic. There is a need to explore environmentally friendly techniques for proper disposal of ash generated by incinerators, to minimize heavy metals in products ending up in the healthcare waste.
Incinerator’s fly ashes and bottom ashes are potentially toxic due to heavy metals contained in ash residues of incinerators (Patra et al., 2017). They also contain other organic toxic chemicals including dioxins, PCBs and PAH. A study on the potential effects of metals and other pollutants in the environment (Michelle et al., 2001) showed that heavy metals are very persistent and may spread beyond the area close to the hospital incinerator. Many hazardous compounds including inorganic pollutants such as heavy metals, sulphur dioxide nitrogen dioxide and organic chemicals such as brominated dioxins, chlorinated and PCBs are released from incinerators and PCNs. Study has identified innumerable toxic substances, which are emitted in pile gases and in ashes, also many unidentified substances of unknown toxicity levels (Allsopp et al., 2001).
Studies have shown ash products formed by the combustion of dry active hospital wastes contain a mixture of unburned carbon and various metal oxides, alumina and silica (McDougall and Pyrah, 1999; Singh and Prakash, 2007; Gidarakos et al., 2009; Zhao et al., 2010). The incinerated bottom ashes ranges in physical form from a mixture of powder to a freely flowing homogeneous powder, trace metallic items, and char or slag. Basically, the bottom ash should be homogeneous, chemically and biologically inert, and free of organic materials with low carbon content. Studies indicated the composition of the incinerator solid residue (ash), which depends on the composition of hospital waste mixture incinerated (McDougall and Pyrah, 1999; Gidarakos et al., 2009; Manyele et al., 2011).
During hospital waste incineration man-made organic chemicals as well as toxic forms of some of heavy metals can be created. The most important constituents of the emission byproducts, in terms of health effects include particulates matters, combustion products of man-made chemicals and heavy metals; the latter two can be adsorbed onto the smaller particulates making them hazardous. In Tanzania, most of hospitals incinerators have low incineration efficiency, with few of them made of fire brick and other refractory materials (Manyele and Anicetus, 2006). Therefore, in these cases, it is more important for the purpose of protecting the living environment and the health of the public, to assess the levels of pollutants emanating from the use of incinerators for medical waste treatment and disposal for early detection of extent of risks posed by ashes and flue gases thereby devising appropriate measures to alleviate or reduce the identified plausible risks.
The Dar es Salaam city, for the past three decades is the fastest growing city among East African countries with a growth rate above or near 5% (Mhache, 2012). Due to over population and rural to urban migration, the city like many other metropolitan cities in developing countries, faces a very big challenge of managing healthcare waste generated in healthcare facilities (HCFs). According to the Tanzania Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) (URT, 2014), an average annual generation of hospital waste in Tanzania is about 6,745tons. Currently, the hospital waste generation rate is about 0.41 kg/occupied bed/day. In dispensaries and healthcare centers the healthcare waste generation rate is about 0.03 kg/patient/day (URT, 2014). Study on medical waste generation rate focusing district hospitals in Tanzania revealed high waste generation rate, indicated about 2,250 kg/day generated in Amana and 2,500 kg/day generated in Ligula hospital. According to Kagonji and Manyele (2011) the generation rate of medical waste of each patient per day was also high, about 1.8 kg/patient/day at Amana hospital and 2.0 kg/patient/day at Ligula hospital. Muduli and Barve (2012), indicated that in Tanzania healthcare centers, most of the waste generated is not appropriately managed especially when it comes to waste segregation, collection, storage and disposal or treatment (leading to incineration of waste contaminated with toxic heavy metals. Appropriate management of healthcare waste (HCW) is very important to the wellbeing of the people and country at large due to its potential environmental hazards and public health risks which may be posed by healthcare waste. The healthcare waste produced in the course of healthcare activities may carry a higher potential for infection, injury and toxicity.
The World Health Organization (WHO) and UNICEF have graded radioactive waste as the most hazardous waste followed by healthcare waste (HCW) (WHO/ UNICEF, 2015. The safe healthcare waste disposal in developing countries like Tanzania is often limited. The only viable technique is incineration of the waste. Otherwise inappropriate disposal of healthcare wastes, like contaminated sharps (syringes and needles) that may be scavenged and reused, may lead to significant numbers of health risks including spread of hepatitis C, hepatitis B, HIV/AID and many other infections problems.
Gautam et al. (2010) indicated that about 73% of the total healthcare waste needs to be incinerated according to international practices. The reason for the increased HCW generation in the country include the multiplication and expansion of healthcare centers especially in urban areas due to drastic population growth as well as on-going immunization campaigns for different diseases outbreak, like tetanus and tuberculosis where the usage of disposable syringes and needles in avoidance of transmission is very common.
In less developed countries like Tanzania, healthcare waste generated usually ends up disposed at dumpsites and landfills, while in developed countries where land is meager and environmental protection controls are tight, environmental policies be likely to lessen landfill disposals as much as possible. Becquart et al. (2009) estimated that about 16 million tons of bottom ashes are produced per annum. In these developed countries, due to problems associated with land filling, bottom ashes are used in road construction and maintenance. According to Okada et al. (2007), about 80% of municipal solid waste is incinerated and the incinerator bottom ash is recycled in different ways. For example in a country like China, more than 80% of the MSW ends up as landfill, and compost production in these land filling ranks as the second major application; only very few processes involving the recycling of bottom ashes have been undertaken (Li et al., 2004).
According to WHO (1994), medical waste forms about 15% of the total hospital waste which is considered to be hazardous and may be toxic or radioactive. Poor management of these medical wastes can cause significant problems and associated health risk (Syed et al., 2017; WHO, 2004). Poor management practice may create a risk, and pollute the environment through emitted smokes and improperly disposed of incinerator by product (Askarian et al., 2013). According to Matiko (2015) the incineration of medical waste as a treatment option is viewed as dangerous. The incineration practice is worsened when operated by untrained or improperly trained operators (Batterman, 2004). Furthermore, when healthcare waste containing toxic metals like mercury is incinerated without proper care, it may release mercury vapor in the atmosphere. When this vapor is inhaled by humans it may be toxic, deadly or lead to life frightening injuries to respiratory and neurological systems (Howard, 2002).
According to Matee and Manyele (2015), the proper healthcare waste management starts from generation stage followed by segregation followed by collection, transport and lastly disposal of hospital waste must be properly managed so as to minimize the health risks to patients, healthcare providers, the general public and safety of the surrounding environment. The improper disposal of medical waste including bottom ash normally sent to the landfill may amplify the health risk by spreading infections and of exposure to toxic chemicals like heavy metals. The common categories of medical waste generated in different Dar es Salaam hospitals included: general, pathological, radioactive, chemical, infectious, sharps like syringes, pharmaceutical wastes and pressurized containers. These categories are also generated in referral hospitals but at varying quantities (Manyele, 2004).
According to Walter (2002), during incineration process, there are two types of residues generates, bottom ash and fly ash. The amount of bottom ashes generated during incineration process is approximately 20 to 30% by weight of the incoming solid waste material (Walter, 2002). Moreover, the inherent ash content of the general waste, fly ash can also contain other mass by virtue of chemical reagents used to treat the inherent fly ash. Systems must be included in the incinerator design so as to handle and treat the two ash streams. However, these two ash streams they can be processed in combination. Pirkle et al. (1991) indicated that heavy metals may not be destroyed or damaged in the incineration process even at elevated temperature but they are simply concentrated up to high levels in the ash residues or dispersed over the surrounding environment from the incinerator stack as a flying ash. For example, if one is exposed to elevated levels of heavy metal like lead, a person can have numerous adverse effects on renal function, developmental effect and reproduction adverse in animals and humans (Bernard et al., 1995; Pirkle et al., 1991).
The by-product of incineration can be categorized into two: bottom ash and fly ash. According to Anamul (2012), most of the ash in the bottom ash is the residues inside the burner after incineration process. The flying ash settles on post burner equipment such as scrubbers. Therefore, it should be noted that bottom ash is the remainder resulting from the incineration of waste material (Anamul, 2012). Recent research paper reported that metals, such as Ni and Zn in the bottom ashes from medical waste incinerators were having high leachability. The current best use of the by-product to safely get rid of ashes is to put ashes in construction materials, or can be used in cement, or to solid waste landfills (Anamul, 2012). However, the bottom ash from medical waste has some special characteristics that must be considered before it can be reused.
The bottom ash from medical waste incineration may contain a large proportion of toxic heavy metals or toxic organic compounds that might hinder its reuse. Previous study by Anamul (2012) has indicated that bottom ash from medical waste contains higher amounts of heavy metals such as Ni, and Zn than does Municipal Solid Waste (MSW). The composition and distribution of toxic heavy metals in bottom ash from hospital incinerators may vary depending on the type of incinerator in use (Anamul, 2012).
Sabiha-Javied and Tofail (2008) also analyzed different heavy metal (Cd, Cr, Cu, Ir, Pb and Zn) in the hospital incinerator bottom ash. The concentration level of heavy metals Pb and Zn were found to be relatively higher than that of other constituents in the waste. The higher concentration level of heavy metals and dioxins such as polychlorinated dibenzodioxin (PCDDs) and polychlorinated dibenzofurans (PCDFs) were also observed in hospital incinerator bottom ash by several researchers (Racho and Jindal, 2004; Gidarakos et al., 2009).
Mohajer et al. (2013) indicated that it is predicted that incinerated healthcare waste may contain heavy metals such as Cr, Pb, Cd, Hg, Zn and many other as well as carcinogenic organic compounds like PCBs, dioxins, benzene, and many other cancer causing organics. If these medical waste by-products are not well disposed, they can pollute the entire environment and pose public health problems such as gastrointestinal abnormalities, acute respiratory syndromes, and various cancers (Zhao et al., 2010; Auta and Morenikeji, 2013).
In Ghana for example, they have guidelines advocating for controlled disposal of medical waste incinerator bottom ash at landfills. The key components indicated in the guideline are: monitoring of hospital waste incinerator bottom ash quality, environmental pollution potential, and treatment strategies so as to ensure the safety of hospital incinerator bottom ash to be disposed of (Adama et al., 2016). This may not be the case for most of African countries where the observations made at the waste incinerator in Dar es Salaam city showed continuous dumping of bottom ash in an open dump pit very close to the incinerator. This habit can lead to high toxic heavy metal levels observed in soils around the dumping site. This paper analyses the toxic heavy metal content of the bottom ash at three regional hospitals and one National hospital at Dar es Salaam city.
Key parameters of Healthcare Waste Management in the studied Hospitals
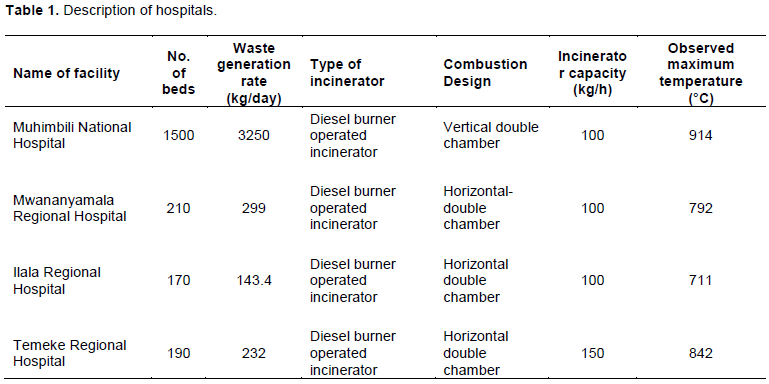
Quantities of healthcare waste generated in a given hospital ranges widely depending on different factors such as size of the hospital, number of outpatient and number of beds. The Muhimbili National Hospital (MNH), which is a National Referral Hospital, has 1500 beds, attended up to 1200 outpatients per day. The volume of healthcare waste generated per day is 325 kg,followed by Mwananyamala Regional hospital having 210 beds and 299 kg/day of waste generated (Table 1). The volume of healthcare waste generated is 3 times higher than the capacity of incinerators. This was also observed earlier (Manyele and Anicetus, 2006), which means most hospitals had low incineration capacity and they cannot accommodate all wastes generated in the respective hospital with few of them are fire brick incinerators.
The volume of hazardous waste generated was very high. The result from investigation reveals that there was a poor segregation at the source of generation of infectious and sharps waste by use of color coding system. This was contrary to what was observed earlier (Matee and Manyele, 2015). Other studies in different African countries show that healthcare waste is either not properly or insufficiently segregated or not segregated at all. Though government policies and action plans are in place, but they are not sufficient or not comprehensive enough to address this problem (Matiko, 2015; Msuya et al., 2003). For the perfect working incinerator, the combustion efficiency is assured by operating the secondary combustion chamber at a temperature ≥1000°C (Baharun et al., 2005). This was not the case for the incinerators visited (Table 1). The maximum temperature observed was 914°C at Muhimbili National Hospital and the lowest was at Ilala Regional hospital with 711°C.

Sources of heavy metals in healthcare waste
During use phase of medical equipment in hospitals, a small portion of the toxic heavy metal may be lost from the products either by corrosion or wear. The heavy metals may be discharged directly to the environment or end up in HCW. The sources of discharges of the toxic heavy metals to the environment and waste water are not addressed in this study, but focus is on the heavy metals in the incinerated waste. Apart from the lost part of the heavy metal, main part of the toxic heavy metals will still be present in the material when the discarded products are disposed of as waste material. The toxic heavy metal will either be part of those collected for recycling or disposed of in the municipal solid waste incinerators (MSWI) or go directly to landfills. However, since the toxic heavy metal content of the data presented here is based on per unit weight of the waste incinerated, the data remain valid whether some part is lost in the HCW, wastewater and vapourization during use. A minor part of the toxic heavy metals will be disposed of as chemical waste and recycled or landfilled via chemical waste treatment. Only very few and incomplete analyses exist of the content of heavy metals containing products in HCW and other complex waste fractions like photographic waste from radiology units. The reason is that these heavy metals are not homogeneously distributed in the medical waste material and it is necessary to sort very large amounts of this waste material to get results of a satisfactorily statistical significance. Figure 1 shows the flow of heavy metals from hospital supplies to the incinerator ashes via healthcare waste.
For instance, the main use of lead compounds, which are lead oxides for cathode ray tubes and crystal glass and stabilizers for polyvinyl chloride (PVC), other uses include plastic syringes, sharp wastes and batteries. With reference to the knowledge of the application of the heavy metals and disposal pattern of the heavy metal containing-products, it is possible to identify the type of chemical based products that may end up in solid waste. For the quantification of the sources, it is necessary to have appropriate knowledge of the consumption of the heavy metals by application both past and today. However, as many products may contain heavy metals, which can last for many years, meaning that they have high half-life; especially those which can be used for infrastructure and in the building sectors, the current analyses of sources of heavy metals to the waste materials may underestimate the contribution from these products.
Flow of heavy metals during incineration of healthcare waste
The known purposes of incineration process are basically to reduce the volume of the waste, to utilize the energy contents and to destroy harmful organic compounds and microorganisms in the waste materials. At the same time, some of the heavy metals during waste, incineration are mobilized or vaporize and accelerates the release of the metals to the environment or some times to the atmosphere. The incineration process typically takes place at temperatures about 1000°C, at which temperature organic materials will burn and be mineralized completely. At this temperature, heavy metals will depend on their physical properties of vaporization, melting or remain in metallic form. The fate of the heavy metals by the incineration will also depend on the waste composition and type of actual process, especially the flue gas cleaning technology (Schachermayer et al., 1995). A schematic view of the flow of toxic heavy metals through an incinerator using wet scrubber for flue gas cleaning is shown in Figure 2. It is important to note that many types of incinerators of this kind in addition may have carbon filter and specific processes for further treatment of the residues, like gypsum precipitation, washing and stabilization of the residues.
Measured Levels of heavy metals in bottom ash
Overall analysis
The bottom ash samples from the four hospitals were tested for eight heavy metal concentration (Cd, Cu, Fe, Zn, Mn, Cr, Pb, As). Most of these toxic heavy metals are required in human body and they can be present in all tissues of the body. Therefore, it is not surprising to find high level of these toxic metals because waste materials from these hospitals contain pathological human parts as well as placentas which are always incinerated. Based on Figure 1, the heavy metal content in the incinerated waste results from sources found in the Waste collected from the hospital cleanliness.

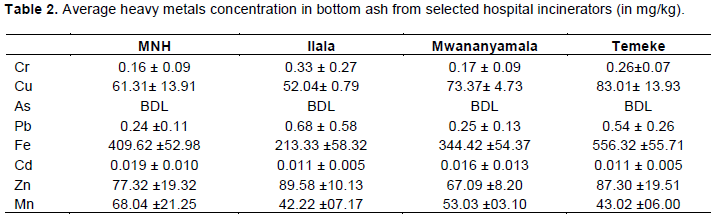
Table 2 summarizes the average metal concentrations of the heavy metals in the bottom ash of the selected hospital incinerators in Dar es Salaam. The average concentration of chromium arranged from highest can be reported as 0.33 ± 0.27 mg/kg (Ilala regional hospital), >0.26 ± 0.07 mg/kg (Temeke regional hospital), >0.17 ± 0.09 mg/kg (Mwananyamala regional hospital) and >0.16 ± 0.09 mg/kg (Muhimbili National Hospital).
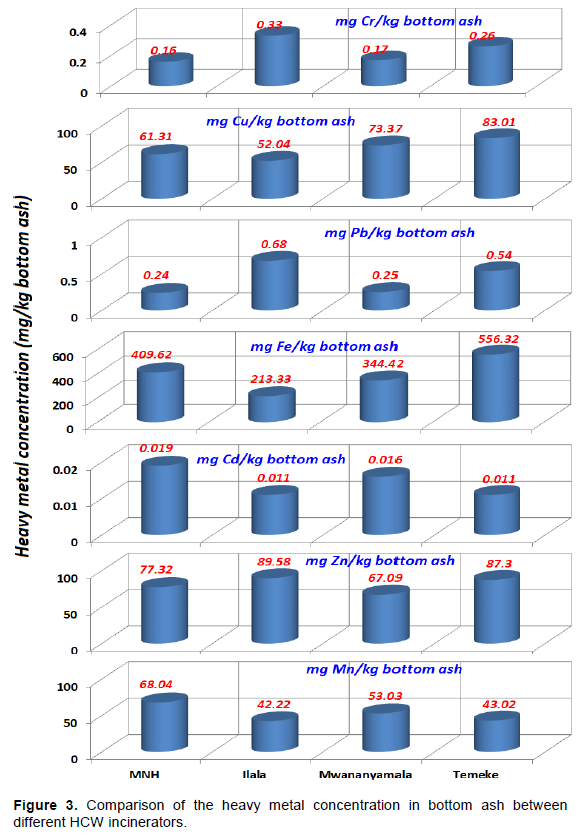
The detected levels were higher than the recommended limit (USEPA, 2010) which is 0.1 mg/kg. These values were about 6 times higher than the values detected in earlier studies (Xu et al., 2016), where the level of chromium was 0.05 mg/kg, but 3 times lower with values detected by Al-Muzaini (2016) which was 0.94 mg/kg. Figure 3 compares the experimental results in graphical form.
Chromium
The variation in the concentration of Cr within incinerator ashes was probably due to two factors. The first factor was the variation in the hospital waste’s composition and the second factor was the differences in the services offered within the hospitals and influx of materials in the hospital (Powell, 1987a). These levels were not unexpected since hospital wastes normally contain about 20% nonorganic materials and, occasionally, the levels can increase as high as 30% (Powell, 1987b). Another factor which leads to high level of chromium in bottom ash is the operating temperature of the incinerator. It is known that the higher the temperature, the lower the concentration of the chromium. The lowest concentration was observed at Muhimbili National hospital where the maximum operating temperature was 914oC, while Ilala regional hospital detected highest level of Cr where the maximum operating temperature was lowest at 711oC. The chromium is normally used in tanning, in wood processing especially in conservation and pigments and dyes for plastic materials. Also in paints and textiles materials and in some cases the Cr alloys (European Commission, 2003). Due to the presence of colored plastics in the waste collected that could be one of the sources of Cr metal in the incinerated healthcare bottom ash material.
Zinc
Zinc concentration ranges from 67.09 ± 08.20 mg/kg detected at Mwananyamala regional referral hospital to 89.58 ± 10.13 mg/kg detected at Ilala regional referral hospital. These values are higher than 0.5 mg/kg which was detected in Singapore by Paula et al. (2017). However, these values were within the USEPA (2007), permissible allowable limits for waste disposal to landfill which is 70 mg/kg. Other metals like lead, zinc metal has a melting point 419.5°C. This temperature is very low compared to incineration temperature. Therefore most of the zinc may have escaped in the flue gas.
Zinc is one of the essential elements to human beings. Because of its nature as an essential trace element, the oral uptake of trace amounts of zinc is essential for human survival. The recommended dietary allowance (RDA) for zinc is 11.0 mg/day for men and 8 mg/day for women (Trumbo et al., 2001). When the recommended amount is excess, immediate symptoms of zinc toxicity including abdominal pain, nausea, and vomiting can be observed. Additional effects include anemia, lethargy, and dizziness (Porea et al., 2000).
During incineration process, about 40% of zinc and copper can remain in a slag and remained 60% of them are volatilized and go into the fly ash and may escape into the atmosphere (Zhang and Kasai, 2004). The melting point of the respective metal has a strong influence on the he rate of volatilization of the heavy metal (Zhang and Kasai, 2004). Hence, the amount of zinc in a slag decreases with increase in temperature. This was evident from another study (Zhao et al., 2009), where the mean level of zinc in the incinerated bottom ash was 4,510 mg/kg, while in the fly ash the mean concentration was 75,093 mg/kg. In order to effectively control the removal process of Zn as it is for metals like Pb with lower melting points it is important to understand their vaporization behaviors from molten materials, usually in chlorine-bearing slag so as to keep community safe on metal toxicity (Barin, 1989).
Copper
The mean concentration of copper ranged from 52.04 ± 7.90 mg/kg to 83.01± 13.93 mg/kg, which was detected at Ilala regional referral hospital and Temeke regional referral hospitals, respectively. These values are twenty times higher than the values detected earlier (Patra et al., 2017) which was 2.2 mg/kg. However, these values are lower than the landfill disposal limits in Singapore for instance, which is 100 mg/kg (Patra et al., 2017). In this case, it is obvious that the higher the amount of waste with various composition of waste is the major factor for observed different value per facilities. The source of Copper is in building’s materials, house wiring materials, house plumbing materials, heating utensils, air conditioning as well as refrigeration, architectural materials, electrical and electronic products, industrial machinery and many others applications (Lam et al., 2010). Copper compounds for example CuSO4 are used in agricultural activities and can be used as fungicides, insecticides, bactericides, pigments. In animal husbandry they can be used in animal feeds, dietary supplements, antifouling paints, and as heat and light stabilizers in polymers. Also copper compounds can find its application in wood preservatives and electroplating.
Iron
The minimum average for Iron concentration, 213.33 ± 58.32 mg/kg, was found for ash samples collected from Ilala regional referral Hospital and the maximum average level detected was 556.32 ± 55.71mg/kg detected at Temeke regional referral hospital. The average level of iron in the incineration bottom ash correspond with the values detected by other researchers earlier, 314 .0 mg/kg (Racho and Jindal, 2004).
The variability could be due to the amount and type of waste generated and collected for incineration. However it is a common metal found in any incinerated medical waste. It was difficult to establish any reference regarding Fe because TBS has not provided any specifications for this metal. However WHO (2003) provides standard for consumption of Fe not exceed 0.8 mg/kg of body weight. Iron is ranked fourth most abundant element in the earth’s crust and it is one of the components of stainless steel which is an alloy of metal Iron, carbon, chromium, silicon, molybdenum, and nickel. The highest concentration of iron in the bottom ash could be due to its high melting point which is 1,493°C higher than most of the incinerators maximum operating temperature. The main component of medical equipment such as needles, scalpel, hypodermic blades and much other compliance are made up of iron. That could be the reason of high level of level of iron to be high in the analyzed bottom ash (Yang and Ren, 2010).
Manganese
Manganese element is one of essential element for living organisms, including human beings. Most enzymes require manganese for example, manganese superoxide dismutase, and some enzymes are activated by the manganese for example kinases and decarboxylases (USEPA, 1984; Hurley and Keen, 1987). The highest mean concentration of manganese was 68.04 ± 21.25, which was detected at Muhimbili National Hospital while the lowest was 42.22 ± 07.17 detected at Ilala regional referral hospital. These values are lower than 214.4 ± 4.11 mg/kg as reported in previous literature (Zhao et al., 2009).
Most of the organs of the body like kidney, liver, pancreas and other organs contain good amount of Manganese compound (Tipton and Cook, 1963). It also accumulates preferentially in the brain in infants and young animals (Kontur and Fechter, 1988). Therefore, incineration of human parts increases concentration of manganese in the bottom ash. The steel alloys and manganese compounds can be another source of Manganise (IPCS, 1999). Manganese dioxide and many other manganese compounds are also used in manufacture of batteries, glass and fireworks. Potassium permanganate is also a known oxidant which is commonly used for cleaning, bleaching and disinfection purposes in hospital laundry. Also, food remains in healthcare is the most important source of manganese (USEPA, 2002). The tolerable upper intake level of Mn is 11 mg/day for adults, based on a recent review (Greger, 1999).
Cadmium
Cadmium can be found in many applications including PVC stabilizer and as a pigment in other plastics, as well as in nickel - cadmium batteries and in some metal plating. Also pigments used in plastic (main use), ceramics, glass and paint (USEPA, 1996). The highest concentration was recorded at Muhimbili National Hospital, 0.019 ± 0.001, while the lowest was recorded at Temeke regional hospital, 0.011 ± 0.005 mg/kg. The levels were extremely low when compared with an earlier study that recorded 7.14 mg/Kg (Adama et al., 2016). However, the levels were within the acceptable permitted standard 0.005 mg/kg (USEPA, 2007).
Cadmium is one of the heavy metals which is not essential for plant or animal life. The solubility of cadmium is relatively high compared to other heavy metals. That is why, cadmium is more mobile in soil, and more bioavailable and tends to bioaccumulate. Therefore, using landfill in disposing the ashes is not recommended because of bioavailability, cadmium can find its way to agricultural products. Cadmium can accumulate in the human body and especially in the kidneys through food web, which can lead to kidney dysfunction (Jorup et al., 1998).
Lead
Lead concentration ranges from 0.24 ± 0.11 mg/kg to0.68 ± 0.58 mg/kg at Muhimbili National Hospital and Ilala regional hospital respectively. These levels are slightly lower than levels detected somewhere else with average of 0.85 mg/kg (Patra et al., 2017), though higher than maximum acceptable limit of 0.05 mg/kg (USEPA, 2007). Like Zn and other heavy metals, such as Cd, have high volatility and sometimes can easily form high volatile compounds (CdCl2 or PbCl2), and thus tend to be transferred into fly ash during the incineration process (Sukandar et al., 2006; Shim et al., 2005).
Most of medical waste incinerated in the selected hospitals contained mostly sharps which consisted of plastic needles and other colored plastic materials. Therefore, it was not surprising that the Pb content was high in the analysis because lead is normally used in pigmentation of plastic materials as well as termination of polymerization process. The low level of lead could be due to its lower melting point which is 328°C, and it is lower than observed incineration temperature ranges between 711 to 914°C. Therefore, melted lead compounds during incineration might have adsorbed on surface area of bottom ash.
Arsenic
The Arsenic compounds found its way in many applications including wood preservatives (such as, chromium copper arsenate); electronic appliances (such as, semiconductors); in agricultural products (such as, fungicides, herbicides, pesticides, and silvicides); nonferrous alloys; animal feed additives; glass; ceramics; and dyeing and printing (USEPA, 1996; Matee and Manyele, 2015). It is most commonly found sulfide ores as arsenopyrite. However, Arsenic was not detected in all four incinerators.
Estimation of the quantity of heavy metals in the waste loaded into the incinerator
Based on the average concentration of the metals in the incinerator bottom ashes (mg metal/kg bottom ashes) (Table 2), and knowing the amount of waste loaded into the incinerator per cycle (Table 1), the quantity of the metals in the waste load (g/kg waste) was estimated for Cr, Cd, Cu, Zn, Pb and Mn. The data for Fe was excluded due to contribution of other sources such as grate and top frame supporting the firebricks, especially for Temeke Hospital Incinerator. Figure 4 presents the results for the four incinerators studied.
Thus, knowing the waste incinerated per day, and hence the corresponding waste generation rate, the quantity of the heavy metals disposed via bottom ashes can be estimated. This can be followed by feasibility studies regarding extraction of the metals from the ashes, given the current price of the metals in the market. The concentration of Pb in the waste is important because Pb is conserved in the combustion process; all the Pb fed to the combustor exists with the bottom ash, is collected as fly ash, or is emitted as fine particles in the stack gas.
Estimation of the quantities of heavy metals disposed of per year via bottom ashes
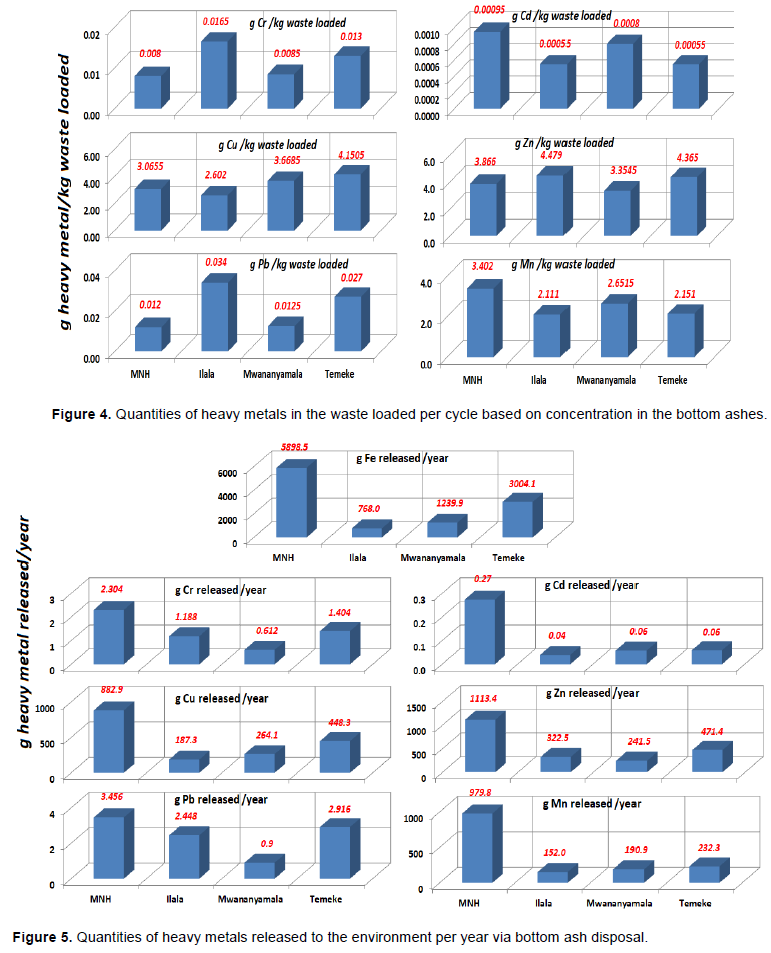
Generally, toxic heavy metals are strongly attached to the bottom ashes due to the high content of alkaline material in these residues, which strongly limits the solubility of heavy metals, and also because these heavy metals are integrated in a silicate matrix created during the incineration process. Due to high concentration of toxic heavy metal in the bottom ashes, and weight reduction of 95%, the amount of heavy metals in g/kg ashes was estimated per cycle. Knowing the number of cycles per day and hence number of cycles per year (360 days), the kg of heavy metals emitted into the environment based on disposal of bottom ash was estimated for each metal as presented in Figure 5.
The quantity of iron released to the environment via ash disposal was the highest compared to other metals due to additional sources released into the ashes during incineration. This is caused by oxidation of iron bars due to rusting and high temperature corrosion (Xu et al., 2016). Moreover, the iron and steel content in the incinerated waste is also high due to many items made of iron or steel entering the healthcare waste stream as reported also by Matee and Manyele (2015) and Manyele et al. (2011). Results show that MNH has the highest release of metals attributable to the large quantities of waste generated per day and thus per year. This because, based on Table 2, most of the metal concentration for MNH were within the observed range for incinerators in other hospitals.
Lead (Pb) emissions from waste incineration process, are influenced by the concentration of Pb in the waste feed, the chemical form of Pb, the physical matrix of the waste, the degree of ash carryover from the primary combustion chamber, thermal conditions in the primary and secondary combustion chambers that affect Pb volatilization, and the air-pollution control system efficiency for fine-particle removal from the gas. The method of feeding waste to the combustion chamber (in batches vs. continuous feeding) can have an indirect effect on Pb emissions. Figure 5, demonstrated that lead will end up in the slag, while cadmium, which due to its low boiling point it will evaporates during the incineration, will tend to adhere to particles mainly end up in the electrostatic precipitator dust.
The environmental concerns related to incineration have traditionally been focused on the vapor (flue gas) as an important source of immediate heavy metal release to the environment. In most cases, emitted heavy metals will be deposited relatively close to the incinerators although a part of the metals - and especially mercury- may be transported over long distances. It is evidently noted that although only a very small part of the heavy metal content of the waste is emitted to the air, emission from waste incinerators may constitute a significant part of the total air emission from a country (Lassen and Hansen, 1996; Drivsholm et al., 2000). However, as the flue gas cleaning systems improve to modern standard, disposal of slag and in particular flue gas cleaning residues are becoming major subjects of concern.