ABSTRACT
Chronic diseases of lifestyle like diabetes mellitus and hypertension appear at greater rates in populations which consumed high fat, high calorie diets and engaged in low or no physical activity. Physical inactivity and unhealthy diets are major contributors of overweight and obesity which are risk factors for lifestyle diseases. This study aimed at determining the relationship between dietary practices, habits, physical activity and the prevalence of obesity, diagnosed diabetes and hypertension in the Swahili community of Old Town and Kisauni districts in Mombasa County, Kenya. A cross-sectional study design was used. Cluster random sampling was done to pick 207 households. Data was collected on food consumption, dietary habits and physical activity. Focus Group Discussions and Key Informants Interviews were used to collect qualitative data. Results indicate that dietary habits of the Swahili community involved preparation and consumption of high fat, sugar and coconut milk-based foods. Most (75.8%) of the interviewed members of this community had low physical activity. Their dietary habits and low physical activity levels were associated with obesity, diabetes and hypertension (p<0.05, 95% CI). Physical inactivity levels were associated with obesity [Odds Ratio, 0.49; 95% Confidence Interval, 0.27 - 0.88]. There is need to acquire sustainability of consumption of healthy diets and physical activity through education and provision of physical activity facilities to prevent obesity, a major risk factor for diabetes and hypertension.
Key words: Dietary practices, dietary habits, physical inactivity, obesity, hypertension, diabetes, Swahili, Kenya.
Chronic diseases of lifestyle are a group of diseases that shared similar risk factors as a result of exposure, over many decades, to unhealthy lifestyle. The unhealthy lifestyle involves lack of regular physical activity and consumption of diets rich in highly saturated fats, sugars and salt (Steyn et al., 2006).
The burden of these diseases is increasing globally and possesses a major public health concern, a large part of which is preventable (WHO, 2017). They are a major contributor to the burden of disease in developed countries and are increasing rapidly in developing countries (Lopez et al., 2006). The locus of the burden resides in the developing world, as it has been projected that, by 2020, about three-quarters of mortality due to heart disease, stroke, and diabetes will occur in developing countries and exceed by 2030 (WHO, 2017). Chronic diseases of lifestyle have an impact on the burden of disease in sub-Saharan Africa (Aikins et al., 2010). WHO projections showed that these diseases will be responsible for a significantly increased total number of deaths in Africa, South-East Asia and the Eastern Mediterranean, where they will increase by over 20% (WHO, 2011). In Kenya, these diseases account for 27% of the total deaths and over 50% of total hospital admissions (MOH, 2015). The major ones are cardiovascular conditions, cancers, diabetes, and chronic obstructive pulmonary diseases with their sequel and shared risk factors (MOH, 2015).
The chronic diseases of lifestyle are largely due to risk factors such as high blood cholesterol, high blood pressure, obesity, physical inactivity and unhealthy diet (Steyn et al., 2006). These risk factors can be classified as modifiable and non-modifiable (WHO, 2011). Nutrition is a major modifiable determinant of chronic lifestyle diseases (McNaughton et al., 2012). Scientific evidence supports the view that alterations in diet and physical activity have affected health throughout life (McNaughton et al., 2012; Reiner et al., 2013). The dramatic changes occurring in people’s diets around the world are referred to as nutrition transition. People consumed more fats, more animal-based products, and more sugar, as well as more processed foods and less fiber (Kearney, 2010). Lifestyle diseases are linked to high consumption of such foods (Bourne et al., 2002). Unhealthy diets, especially those which have a high content in fats and free sugars and physical inactivity are among some of the leading causes of these diseases including cardiovascular diseases (CVDs), type 2 diabetes and certain cancers (Whatnall et al., 2016).
Nutrition patterns are influenced by many factors, including individual preference, culture, traditions and beliefs (Nordstrom et al., 2013). People are normally proud of who they are and where they come from. The foods that people feed throughout their childhoods most often stay with them throughout their lives like favorite food types. Even in the midst of globalization where many aspects of healthy living are a concern, people hold onto the cultural cooking practices that are known to be the best and have helped them to shape up to the people they are and what they believe about life in general (Morgan, 2000). However, this does not mean that all types of cooking are healthy. In the US for example, in Georgia, Mississippi and Alabama, majority of the populations are overweight or obese. This has a lot to do with the famous Southern cooking that has been traditionally based on staples like fatback, fried potatoes, fried chicken, fried cabbage, fried catfish, fried eggs and a lot of other fried items (Balarajan, 2001). Besides widespread obesity rates, there are also increased levels of lifestyle diseases (Balarajan, 2001). Overweight and obesity predisposes affected individuals to the chronic diseases of lifestyle (Crino et al., 2015). The Swahili community of the Kenyan coast has specific cooking methods and diets based on their culture. They use coconut milk and a lot of sugar in their cooking. Their staple food has a lot of Indian influence, thus most of their cooking is rich in spices (MOT, 2015). Popular Swahili cuisine includes wali, that is, rice cooked in coconut milk, which is served with a thick meat stew or fish, and pilau, a spicy variety of wali. Goat meat and chicken curries are traditionally popular during special occasions. They also eat a lot of different grains, vegetables and fruits including beans, peas, tomatoes, potatoes, okra, kale, spinach, mangoes, coconut and bananas (MOT, 2015).
Physical activity is defined as any bodily movement produced by skeletal muscles that require energy expenditure (Singh, 2013). It is a key determinant of energy expenditure, and thus is fundamental to energy balance. Physical inactivity, that is, a lack of physical activity is an independent risk factor for lifestyle diseases. It is associated with increased levels of obesity, breast cancer, colon cancer, osteoporosis, stress, anxiety and depression. It is one of the major underlying causes of mortality in the world (Booth et al., 2012). It is estimated to cause 1.9 million deaths globally. Lifestyle diseases associated with physical inactivity are the greatest public health problem in most countries around the world (WHO, 2010). Many studies across sub-Saharan Africa have revealed the impact of a sedentary lifestyle on emerging chronic disease risk factors (Forrest et al., 2001; Aspray et al., 2000; Sobngwi et al., 2004). Steyn et al. (1999) showed an independent association between low levels of physical activity and having diabetes in a poor, peri-urban community near Cape Town, South Africa. It has also been shown that moderate amounts of physical activity are associated with health benefits, and can help reduce various chronic diseases related to lifestyle (Blair et al., 2001).
Studies have shown that there is a relationship between risk factors for lifestyle diseases and their prevalence (Nazri et al., 2008; Gothankar, 2009). A study on prevalence of overweight, obesity and self-reported chronic diseases among residents in Malaysia reported a relationship between overweight, obesity and chronic diseases of lifestyle (Nazri et al., 2008). In another study on prevalence of obesity and its associated comorbidities amongst adults, Gothankar (2009) reported an association between obesity, hypertension and diabetes. These studies determined the relationship between obesity and lifestyle diseases. Physical inactivity and unhealthy diets which are documented as major contributors of overweight and obesity were not looked into. This study was to investigate dietary practices, habits and physical activity in the Swahili community of the Kenyan coast in relation to the prevalence of overweight, obesity, diabetes and hypertension.
Location of the study
The study was conducted in Mombasa County of Kenya. It is situated in the Southeastern part of the former Coast province. It covers an area of 229.9 km2. Water mass accounts for 65 km2. It borders Kilifi to the North, Kwale to the South and West and the Indian Ocean to the East. The district lies between latitudes 3°-80’ and 4°-10’ South of the Equator and between longitudes 39°-80’ East of the Greenwich Meridian. This County is an island linked to the mainland by a road and a railway bridge to the northwest and a further road bridge to the north coast. A vehicular ferry links the island with the south coast at Likoni (Berry, 2014).
Experimental design
The study design assumed both quantitative and qualitative approaches and was a one-time cross-sectional study involving men and women aged 30 to 70 years old. Children as well as men and women whose age did not fall between 30 and 70 years were excluded from the study.
The study also assumed a comparative approach to determine any significant differences that existed between the Old Town and Kisauni districts’ respondents.
Diabetes mellitus and hypertension were documented based on self-reports and showing of clinic cards by already diagnosed individuals. Body mass index (BMI) was used to classify people into underweight, normal weight, overweight or obese. The BMI was calculated as a ratio between weight in kilograms and height of the respondent in meters squared (kg/m2) and compared with internationally recommended cut-off points for status (Kolimechkov, 2014). A person with a BMI of 30 or more is generally considered obese. A person with a BMI equal to or more than 25 is considered overweight (Kolimechkov, 2014).
Study population
The study population was the Swahili community. This community has been described as an ethnic-mixed group of people speaking closely related forms of Bantu speech, living on islands and coastal areas of East Africa. Historically, the Swahili developed as Arab and Persian traders established business contacts and married local women on the East African coast around AD 700 (MOT, 2015). The resulting people were Islamic Bantu-speaking fishers, traders and woodwork artisans, living in city-states varying from governorships to republics. The people's features vary from light-skinned Arab to Bantu. They have close association with Arabic and Islamic cultures (MOT, 2015). The Kenyan Swahilis are the Bajun, Fundi, Ozi, Pate, Vumba, Mvita (from Old Town, Mombasa), Shela, Amu (the dialect of Lamu Island) and Siyu, which are communities resulting from mestization among the ancient Arabs and Persians. In Mombasa, the Swahili maintain close relationships with Arabs, some native to Kenya and some Yemeni. They have a wide range of socio-economic activities, religious and cultural values. They are matriarchal and family or clan oriented. They are renowned as sailors, traders and artisans. They are a welcoming, hospitable people and enjoy meeting people from other places and cultures (MOT, 2015).
Target population
The target population consisted of men and women aged 30 to 70 years old from the Swahili community in Old town and Kisauni districts of Mombasa County. Old town is an historical home of the Swahili community. The town's inhabitants were mostly of the ancient Arabs (UNESCO, 2011). Kisauni on the other hand is sub-county (district) within Mombasa County. Old town has a high population of the Swahili people, therefore the community here possessed more Swahili culture and characteristics hence had slightly different dietary habits and practices compared to Kisauni district community, which had slightly deviated from the typical Swahili culture due to adopting other ethnic groups’ cultures (UNESCO, 2011).
Sampling and sample size
The sampling frame consisted of men and women residing in Old town and Kisauni districts, as the two study clusters. Both of these two districts were purposively selected for the study. The unit of analysis was the individual households, represented by the selected members of the households, who were administered with and responded to the survey questionnaire. A man and woman were randomly picked from each household. Simple random sampling was used where the members of the household picked papers from a hat and one man and one woman were selected. The sample size was calculated using the Fisher’s formula recommended by Mugenda and Mugenda (2003). A sample size of 207 households was achieved. Household lists of Old town and Kisauni districts were obtained from the local government offices. Proportionate sampling was used to get the specific number of households from each of the two study sites. From Kisauni district, 12,747/26,650 × 207 = 99 households and Old Town district, 13,903/ 26,650 × 207 = 108 households.
Dietary assessment
Two methods of dietary assessment were used in this study; a Food Frequency Questionnaire (FFQ) and 24-h recall. More than one method of assessing dietary intake is recommended as one method is susceptible to biases (Previdelli et al., 2016).
Physical activity assessment
The Global Physical Activity Questionnaire (GPAQ) was developed by WHO for physical activity surveillance in countries (WHO, 2004). It collected information on sedentary behavior and physical activity participation in three settings or domains which include: activity at work, travel to and from places and recreational activities. The GPAQ was validated by a WHO expert group working on physical activity measurement. Around 50 developing countries are now using the GPAQ for physical activity data collection (WHO, 2004). This study assessed physical activity in the three settings or domains. The data was analysed using EpiInfoTM CDC software (WHO, 2004). The interviewed household members’ mean physical activity was described using an indicator called metabolic equivalents (METs) then categorized in 3 levels of physical activity as low, moderate and high. This calculation and categorization was done using the GPAQ guide (WHO, 2004).
Focus group discussions (FGDs)
Ten volunteers from each of the study sites were selected and invited to a Focus Group Discussion (FGD), to respond to some structured questions that sought to elicit information on Swahili dietary habits and practices with particular emphasis on type of foods consumed and their preparation methods. Information derived from the FGD was used to complement that from household survey. Women were purposively selected to be involved in these discussions because they were involved in food preparation.
Key informants interviews (KIIs)
KIIs were used to seek in-depth information over and above what was collected from focus group discussions and household survey. The key informants, mainly the village elders, were identified by the community members based on their positions in the community and interaction with the community members.
Observation
Observations were made on the Swahili community’s way of life, their dietary habits, cookery ingredients and food preparation methods during data collection. These observations were used to verify the information given by the respondents.
Ethical considerations
An introductory letter was obtained from Egerton University Graduate School before carrying out the study. This facilitated the acquisition of ethical approval from the University’s Ethical Review Board. A study permit from the National Council of Science and Technology authorizing the carrying out of the study among Swahili people in Mombasa County was also acquired. Permission was also sought from the administration offices to carry out the study in the County. Individuals’ informed consent was obtained before interviewing them and this was after explaining to them the purpose of the study and how the results from the study will be used. They were also assured of strict confidentiality of all the information collected in the study. This was done by ensuring that their names were not included in the questionnaires.
Data analyses
Following the coding and computer entry of the data, both descriptive and inferential analyses of the data were undertaken, using the Statistical Package for the Social Sciences (SPSS) version 20 (SPSS Inc., USA). Appropriate descriptive analysis was used to generate frequency distributions and tables and inferential analyses to indicate relationships between various independent and dependent variables, including bivariate and multivariate analysis to measure the strength of relationships between the variables. The Chi-square test at 95% confidence intervals and a p-value <0.05 was used to test for differences between the Old town and Kisauni districts findings. Descriptive analysis was undertaken for the Focus Group Discussion and the Key Informant interviews to complement the analyses from the questionnaire survey findings. Nutri-survey program was used to analyze the 24-h dietary recall data. GPAQ data was cleaned and analyzed using EpiInfoTM CDC software. The interviewed household members’ mean physical activity was described using an indicator called metabolic equivalents (METs) then categorized in 3 levels of physical activity as low, moderate and high. This calculation and categorization was done using the GPAQ guide.
General household characteristics
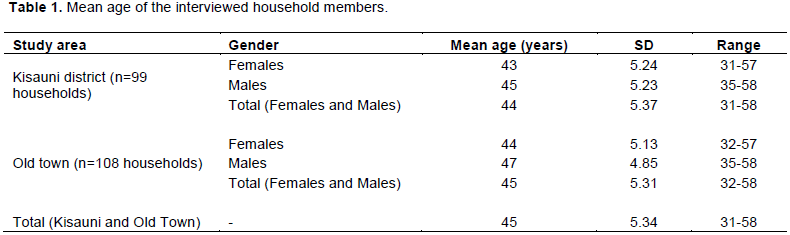
A total of 414 participants (198 from Kisauni district and 216 from Old town) were included in the study. Out of this, 99 women and 99 men were from Kisauni district and 108 women and 108 men from Old town district. The mean age of the household members that were interviewed in Kisauni district was 44 years whereas in Old town it was 45 years (Table 1). The mean number of household members in Kisauni district was 3.4 whereas in Old town it was 3.8.
Food consumption and dietary practices and habits
Nutrient intake
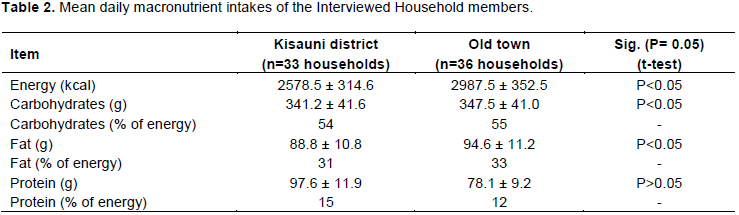
The nutrient intake of the individuals studied indicated comparable intakes between both Kisauni district and Old town. Percentage of calories coming from fat and carbohydrates was slightly higher in the community members from Old town than those in Kisauni district. This difference was non-significant. The percent calories coming from fat was 31% for the group from Kisauni district and 33% for the group from Old town, 15% came from proteins for the group in Kisauni district and 12% for the group in Old town and rest (54%) from carbohydrates for Kisauni district and 55% for Old town (Table 2). The individuals in Kisauni district had mean energy intake of 2578.5 kcal and those in Old town had mean energy intake of 2987.5 kcal. It was reported during the FGD in Kisauni district, that apart from the typical Swahili dishes, the community in Kisauni district consumes foods from other communities like sima (posho made from maize flour) and fish. One woman said, ‘Mbali na vyakula vya kikwetu, huwa twala sima na samaki.’ This is translated as, ‘Other than our typical foods we eat sima and fish.’ It was also reported that, ‘Foods like sima, sukuma wiki (kales) and githeri (mixture of maize and beans) are not common in the Swahili culture.
Dietary practices and habits
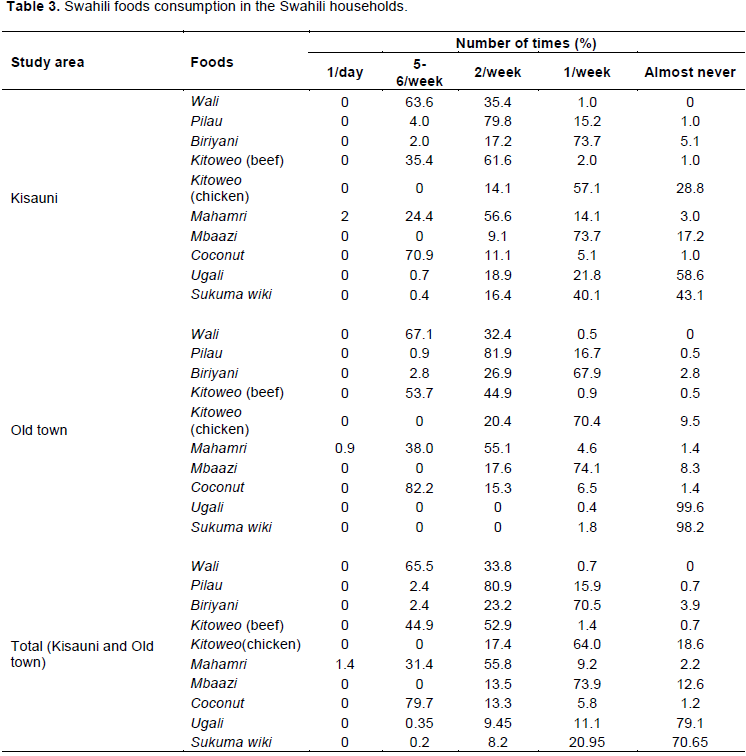
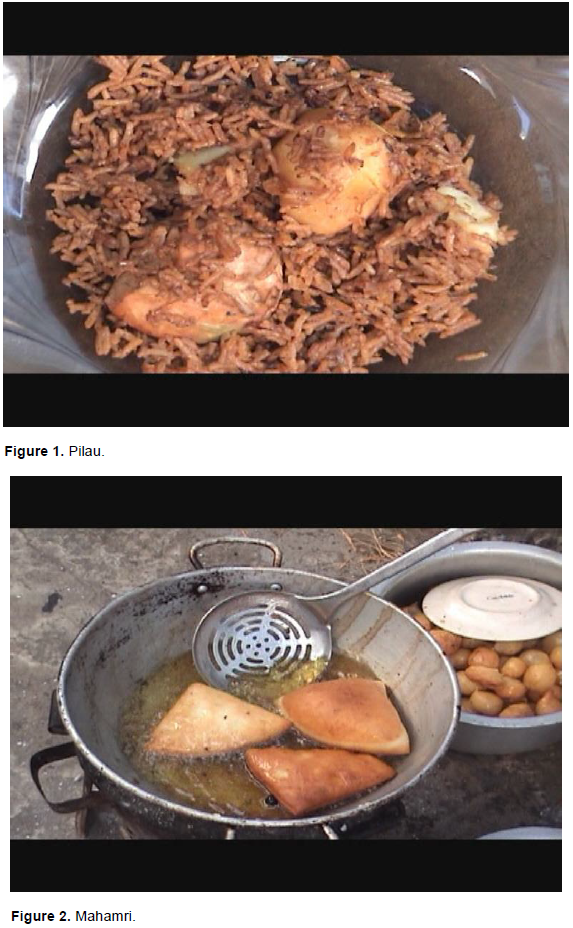
Dietary practices and habits were assessed using a FFQ. The frequency of some of the Swahili foods that were mostly consumed is shown in Table 3. These foods include: pilau (Figure 1) and biriyani, which are spicy varieties of rice and served with kitoweo (beef or chicken stew), mahamri (doughnut-like snacks flavoured with coconut milk and spices; Figure 2), mbaazi (pigeon peas cooked with coconut milk and served with thick coconut paste) and coconut meat stew (Figure 3). Other Swahili foods consumed included: samaki wa kupaka (fish cooked in coconut milk), uji wa mchele (porridge made from rice flour and coconut milk), katlesi (fried mashed potatoes coated with egg white), viazi vya jeera (spicy mashed potatoes), tambi (pasta), sharbati ya tende (milk shake prepared using coconut milk and dates), viazi vya tamu (sweet potatoes cooked in coconut milk), vibibi (pancakes cooked with coconut milk), kaimati (pastries cooked using coconut milk and coated with sugar; Figure 4), viazi vya karai (deep fried potatoes coated with wheat and gram flour paste; Figure 5) and mkate wa tambi (baked pasta bread flavored with coconut milk; Figure 6). These foods are high in fats and sugars. The high fat and sugar content was observed in the streets of Mombasa County as the foods and snacks were being prepared for sale. Some the foods are mostly consumed during special occasions and religious occasions like Muslim fasting period (Ramadan), maulid and idd as reported by the women in the FGDs and Key Informant Interviews (KIIs). These occasions occurred once or twice in a year but consumption of these foods may contribute to obesity because the foods are prepared and consumed in large quantities during this period. A significant difference was indicated in coconut milk intake between Kisauni and Old town districts. Members of the Swahili households in Old town district had a higher intake of coconut milk than those in Kisauni district. Coconut milk was obtained primarily by pressing the grated coconut's white kernel or by passing hot water through grated coconut, which extracts oil and aromatic compounds.
The women participating in the FGDs were very responsive when describing the Swahili diet and dietary habits. They said, “The Swahili diet is high in fat, species and sugars. They mentioned wali, pilau, biriyani, mahamri and mbaazi as the Swahili foods that are commonly consumed. "Foods like tambi, kaimati, sharbati ya tende, uji wa mchele, samaki wa kupaka among others are consumed during special occasions like Ramadan,” they said. It was also reported that three meals and two snacks are served in Swahili households and dining out was not common in this community. They preferred eating their meals at home. Food preparation and cookery methods were also discussed. The following were the representative responses given on this subject: “The ingredients used for preparation of most Swahili dishes include: cinnamon, cardamom, black pepper, mixed spices, tamarind among other spices.” “Most of the foods are deep fried.” “The fat used for frying is vegetable oil commonly known as uto.”
Dietary habits of the Swahili community generally involved preparation and consumption of high fat, sugar and coconut milk foods. These foods were frequently consumed in majority of the households.
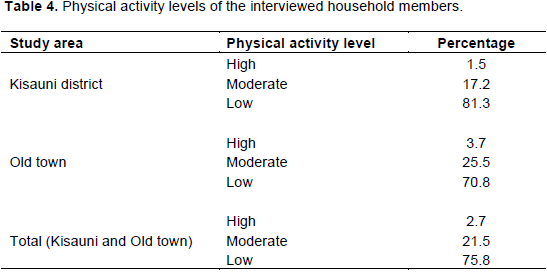
Physical activity levels
About 75.8% of the interviewed household members in both Kisauni and Old town districts had low levels of physical activity (Table 4). Majority (81.3 and 70.8% in Kisauni and Old town, respectively) of the individuals had low levels of physical activity. A significant difference between physical inactivity in Kisauni district and Old town district was indicated. Individuals in Kisauni district had lower physical activity levels than those in Old town. This was noted during the FGD in this district where it was reported that, ‘Kwa waswahili hakuna mazoezi mtu akitaka kwenda pahali kidogo mpaka tuktuk ama matatu’. This is translated as ‘In the Swahili community people do not engage in physical activity, they use vehicles to travel short distances’. Old town district is situated in an area that has no grounds for physical or recreational activity; the houses are very crowded. Despite the availability of grounds for physical or recreational activity in Kisauni, members of this district did not engage in physical activity. The women in both areas were mainly homemakers and those that worked had businesses that involved sitting down, cooking and selling the Swahili foods and snacks hence minimal movement. The men on the other hand said that they were not physically active. Few of them said they went to the gym, for swimming and some jogged hence 2.7 and 21.5% of the interviewed household members had high and moderate physical activity level, respectively.
Prevalence of overweight and obesity in the Swahili community of old town and Kisauni district
There was a high (87.2%) prevalence of overweight and obesity among the interviewed household members in both Kisauni and Old town districts as shown in Table 5. The mean BMI in both study areas was above 25, hence the high prevalence overweight and obesity. About 48.5 and 35.9% of the interviewed household members in Kisauni district were overweight and obese, respectively compared to 37.5 and 52.3%, respectively in Old town district. There was a significant difference between overweight and obesity levels in Kisauni and Old town districts. Old town had more individuals that were obese.
Prevalence of diagnosed diabetes mellitus and hypertension in the Swahili community
About 11.1 and 39.9% of the interviewed household members in Kisauni district had diagnosed diabetes and hypertension, respectively compared to 14.8 and 44.0%, respectively in Old town district (Table 6).
Association between the risk factors for chronic diseases of lifestyle (Unhealthy dietary habits and practices, physical inactivity, overweight and obesity)
Dietary habits of the interviewed household members in Kisauni and Old town districts were significantly associated with their physical activity levels, weight status and diagnosed diabetes and hypertension (p<0.05, 95% CI). Physical activity levels in Old town district were significantly associated with overweight and obesity (p<0.05, 95% CI, 0.27 - 0.88). Overweight and obese individuals had low physical activity levels.
Logistic regressions indicated that, in Kisauni district, the odds that someone who was physically inactive is 1.28 times likely to be obese than the individuals who were physically active whereas in Old town district, the odds are 0.49 times. Logistic regressions between dietary intake and obesity did not show statistical significance association between both.
Obesity among the individuals in Kisauni (p<0.05, 95% CI, 2.17 - 15.80) and Old town (p<0.05, 95% CI, 1.37 - 7.50) districts was statistically significantly associated with diagnosed diabetes. Obesity as assessed by BMI in this community was associated with hypertension and diabetes. In Kisauni district, the odds that someone who was obese (BMI>30) is 5.87 times likely to be diabetic than the individuals who had a BMI<30 whereas in Old town the odds are 3.20 times. On the hand, in Kisauni district the odds that someone who was obese (BMI>30) is 1.67 times likely to be hypertensive than the individuals who had a BMI<30, whereas in Old town the odds are 1.02 times.
The slightly higher macro-nutrient intake in Old town can be explained by consumption of typical Swahili foods which are high in sugars and fat. The Swahili community from Kisauni district on the other hand had diversified its diet by consuming foods from other communities which are not as high in fat and sugars like their typical foods. The high and frequent consumption of coconut milk in Old town is also attributed to the Swahili community’s dietary habits and practices (MOT, 2015).
In the study on dietary habits of the sub-urban Saudi Arabian community which is similar to the Swahili community, Bader and Khalid (2008) reported that around half of the participants eat meals regularly, two snacks between three main meals. More than three quarters (78%) do not eat meals from outside, and the types of fat and oil used were mostly of vegetables source (83.9%). Historically, the Swahili people developed as Arab and Persian traders established business contacts. They have close association with Arabic and Islamic cultures (MOT, 2015). This explains the similarity in dietary habits between the Saudi Arabian and Swahili communities (MOT, 2015).
The physical inactivity can be attributed to most of the individuals not participating in physical activity during leisure time and engaging in occupational and domestic activities that do not involve a lot of physical activity. The culture and religion, as stated in the focus group discussions, require the women to stay home as the men go out to work which translated into physical inactivity among the women who just had minimal movements around the house. Generally, in the urban settings, people tend to do less physical exercise. Public transport is mostly used thus walking is minimal. An increase in the use of passive modes of transport has been associated with declining physical activity levels (WHO, 2010). People do less labor-intensive work and watch television even in the poorer urban settings, compared to those living in rural settings (Miranda et al., 2016). Mombasa County is an urban area where majority of the people use public transport and are involved in jobs that are less labour-intensive hence sedentary behavior during occupational activities (MOT, 2015).
Old town had more obese individuals, which could be attributed to the physical inactivity and high caloric intake especially from coconut milk. Over 95% of coconut oil is fat and the fat content of scraped coconut is around 34% and of coconut milk around 24% (Amarasiri et al., 2006). The community in Kisauni district on the other hand consumed other foods that were not typical of this community which may be the explanation of their lower caloric intake. However, their physical activity level was low hence the cases of overweight and obesity among individuals in this district. Physical inactivity and unhealthy diets are major contributors to overweight (Whatnall et al., 2016).
The association between physical inactivity and obesity as well as between obesity and lifestyle diseases in this study is also reported in other studies. For instance, the physical inactivity of the Nigerian civil servants, studied by Forrest et al. (2001), was correlated to increased weight, BMI and waist-to-hip ratio in men. Similarly, Sobngwi et al. (2004) in Cameroon as well as Aspray et al. (2000) in Tanzania concluded that physical inactivity was associated with obesity in the people they studied in urban and rural settings. In a study on physical activity among middle-aged West African women, more walking was associated with a three-unit lower BMI (Sobngwi, 2004). Therefore, increased physical activity among members of the Swahili community would lead to a decline in the cases of overweight and obesity. Similar findings are reported in the study among the Saudis where Mohammed et al. (2002) reported that there was an association between obesity in the Saudi population and physical inactivity. He also reported that mean BMI is increased by decreased physical activity. In a study on prevalence of obesity and its associated comorbidities, Gothankar (2009) reported that there was a significant association between BMI (³25) and diabetes (p<0.05) and BMI and hypertension (p<0.05). Other results in a study on overweight, obesity, central adiposity and associated chronic diseases in Cuban adults, Diaz et al. (2009) reported that obesity was significantly more frequent in diabetics and hypertensive individuals. The association between hypertension and obesity has been documented in other countries. In Zimbabwe, Mufunda et al. (2000) found this strong association. Mohammed et al. (2002) also reported a significant association between high blood pressure and obesity among Saudi men and women. Joubert et al. (2007) on the other hand found that increased body mass index (BMI) was associated with hypertensive diseases and osteoarthritis.
Unhealthy dietary habits and practices and physical inactivity are major risk factors for obesity and chronic diseases of lifestyle like diabetes and hypertension among members of the Swahili community.
The findings of this study are important in providing a baseline that would help stakeholders come up with timely dietary and lifestyle interventions that would be used in the prevention of obesity and lifestyle diseases. Such interventions like sustainability of consumption of healthy diets require financial investments, which are small when compared with the resources needed for the treatment and management of these diseases as well as the losses due to morbidity and mortality.
The authors have not declared any conflict of interests.
The authors are grateful to the Higher Education Network for Applied Human Nutrition between East Africa and Germany (HENNA) and National Council for Science and Technology for funding the field work.
REFERENCES
|
Aikins A, Unwin N, Agyemang C, Allotey P, Campbell C, Arhinful D (2010). Tackling Africa's chronic disease burden: from the local to the global. Globalization and Health 6:5.
Crossref
|
|
|
|
Amarasiri W, Dissanayake AS (2006) Coconut fats. The Ceylon Medical Journal 51(2):47-51.
Crossref
|
|
|
|
|
Aspray TJ, Mugusi F, Rashid S, Whiting D, Edwards R, Alberti KG, Unwin NC (2000). Rural and urban differences in diabetes prevalence in Tanzania: The role of obesity, physical inactivity and urban living. Transactions of the Royal Society of Tropical Medicine and Hygiene 94(6):637-644.
Crossref
|
|
|
|
|
Bader FA, Khalid SA (2008). Dietary habits in a Suburban Saudi community. Biomedical Research 19(1):55-59.
|
|
|
|
|
Balarajan M (2001). The nutrition transition and its health implications in lower income countries. Public Health Nutrition 1:5-21.
|
|
|
|
|
Berry B (2014). FOTW "Flags of The World" Available at
View Accessed on 2/9/18.
|
|
|
|
|
Blair SN, Cheng Y, Holder JS (2001). Is physical activity or physical fitness more important in defining health benefits? Medical Science of Sports and Exercise 33(3):79-99.
Crossref
|
|
|
|
|
Booth F, Roberts KC, Laye MJ (2012) Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology 2(2):1143-1211.
Crossref
|
|
|
|
|
Bourne L, Lambert EV, Steyn K (2002). Where does the black population of South Africa stand on the nutrition transition? Public Health Nutrition 5(1A):157-162.
Crossref
|
|
|
|
|
Crino M, Sacks G, Vandevijvere S, Swinburn B, Neal B (2015). The influence on population weight gain and obesity of the macronutrient composition and energy density of the food supply. Current Obesity Reports 4: 1.
Crossref
|
|
|
|
|
Diaz ME, Santa MD, René GG, Mariano B, Iraida W (2009). Overweight, obesity, central adiposity and associated chronic diseases in Cuban adults. Medical Review Fall 4(11): 23-28.
|
|
|
|
|
Forrest KY, Bunker CH, Kriska AM, Ukoli FA, Huston SL, Markovic N (2001). Physical activity and cardiovascular risk population. Medical Science Sports Exercise 33(9): 1598-604.
Crossref
|
|
|
|
|
Gothankar SJ (2009). Prevalence of obesity and its associated comorbidities amongst adults. National Journal of Community Medicine 2(2): 221-224.
|
|
|
|
|
Joubert J, Norman R, Lambert EV, Groenewald P, Schneider M, Bull F (2007). Estimating the burden of disease attributable to physical inactivity in South Africa in 2000. South African Medical Journal 97: 725-31.
|
|
|
|
|
Kearney J (2010). Food consumption trends and drivers. The Royal Society 365: 2793-2897.
Crossref
|
|
|
|
|
Kolimechkov S (2014) Body Mass Index. STK Sorts UK.
www.stk-sport.co.uk
|
|
|
|
|
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL (2006). Global burden of disease and risk factors. Oxford University Press and World Bank, Washington DC.
Crossref
|
|
|
|
|
McNaughton SA, Crawford D, Ball K (2012). Understanding determinants of nutrition, physical activity and quality of life among older adults: the wellbeing, eating and exercise for a long life (WELL) study. BMC Public Health 10: 109.
|
|
|
|
|
Miranda JJ, Rodrigo MC, Robert HG, Avilez JL, Smeeth L, Checkley W, Antonio BO (2016). Patterns and determinants of physical activity in rural and urban areas in Peru. Journal of physical activity and health, 13 (6): 654-662.
Crossref
|
|
|
|
|
Ministry of Health (MOH) (2015). Kenya stepwise survey for non-communicable diseases risk factors report, Ministry of health. Division of non-communicable diseases, Nairobi.
|
|
|
|
|
Mohammed AA, Iman AH, Robin BH, Mansour A, Khalid A, Abdul RA, Omar SA (2002). Prevalence and risk factors of obesity and overweight in adult Saudi population. Nutrition Research 22: 1243–1252.
Crossref
|
|
|
|
|
Morgan B (2000). The nutrition transition in low-income countries: An emerging crisis. Nutrition Review 52: 285-298.
|
|
|
|
|
Ministry of Tourism (MOT) (2015). The Swahili Tribe. Available at:
View.
|
|
|
|
|
Mufunda J, Scott LJ, Chifamba J, Matenga J, Sparks B, Cooper R, Sparks H (2000). Correlates of blood pressure in an urban Zimbabwean population and comparison to other populations of African origin. Journal of Human Hypertension 14(1): 65-73.
Crossref
|
|
|
|
|
Mugenda OM, Mugenda GA (2003). Research methods, quantitative and qualitative approach, Acts press, P.O Box 45917, Kenya.
|
|
|
|
|
Nazri SM, Kamarul IM, Imai IM, Ahmad F (2008). Prevalence of overweight and self-reported chronic diseases among residents in Pulau, Malaysia. Southeast Asian Journal of Public Health 39(1):162-167.
|
|
|
|
|
Nordstrom K, Chritian C, Jonsonn H, Nordenfelt L, Gormann (2013). Food and Health: individual, cultural or scientific matters? Genes Nutrition 8:357-363.
Crossref
|
|
|
|
|
Previdelli NA, Andrade CS, Fisberg MR, Marchioni MD (2016). Using two different approached to assess dietary patterns: Hypothesis-driven and data-driven analysis. Nutrients 8:593.
Crossref
|
|
|
|
|
Reiner M, Niermann C, Jekauc D, Woll A (2013). Long-term health benefits of physical activity-a systematic review of longitudinal studies. BMC Public Health 13:813.
Crossref
|
|
|
|
|
Singh K (2013). A study of physical activity, exercise and physical fitness: Definitions and bifurcation for physical activity related research. Academic Sports Scholar 1(11).
Crossref
|
|
|
|
|
Sobngwi AM (2004). Physical inactivity: a mediator of cardiovascular risk. International Journal of Obesity Related Metabolic Disorders 26(4):5-7.
|
|
|
|
|
Steyn K, Fourie J, Temple N (2006). Chronic diseases of lifestyle in South Africa: Technical Report. Cape Town: South African Medical Research Council, South Africa.
|
|
|
|
|
Steyn K, Fourie JM, Lombard CJ, Katzenellenbogen J, Bourne L, Jooste P (1999). Hypertension in the black community of the Cape Peninsula, South Africa. East African Medical Journal 11:758-763.
|
|
|
|
|
United Nations Educational, Scientific and Cultural Organization (UNESCO) (2011). Mombasa Old town, world heritage convention: United Nations: United Nations Educational, Scientific and Cultural Organization.
|
|
|
|
|
Whatnall CM, Collins EC, Callister R, Hutchesson JM (2016). Associations between unhealthy diet and lifestyle behaviours and increased CVD risk in young overweight and obese women. Healthcare 4:57.
|
|
|
|
|
World Health Organization (WHO) (2004). Surveillance and population-based chronic disease prevention: Geneva, World Health Organization. Available at:
View
|
|
|
|
|
World Health Organization (WHO) (2010). Global status report on non-communicable diseases. Available at:
View
|
|
|
|
|
World Health Organization (WHO) (2011). Global status report on non-communicable diseases 2010. Available at:
View
|
|
|
|
|
World Health Organization (WHO) (2017). Non-communicable diseases. Fact Sheet. Available:
View
|
|