Full Length Research Paper

ABSTRACT
Healthy eating during adolescence is a fundamental prerequisite for optimal physical growth, psychosocial and cognitive development and prevention of diet-related chronic diseases. This study assessed the dietary habit, nutritional status and associated factors among adolescents in Tamale metropolis, Ghana. An analytical cross-sectional survey of 402 adolescents was used in this study. Semi structured questionnaire was used to solicit information on the adolescents’ socio-demographic characteristics and dietary practices. Descriptive statistics and regression analysis were used to summarize the data and to assess factors associated with the adolescent’s dietary habits and nutritional status. Meal skipping (87.8%), particularly breakfast was observed as the main unhealthy eating habit among adolescents in the Tamale metropolis. The prevalence of underweight, overweight and obesity as observed among adolescents were 26.1, 5.2, and 0.7%, respectively. Adolescents whose caregivers/parents are of low socio-economic status were 27% less likely to practice unhealthy dietary habits compared to those whose parents/caregivers are of high socio-economic status (OR=0.73; 95%CI: 0.54-0.99; P=0.04). The risk of adolescents being underweight as against normal in males was 2.46 times higher (RRR=2.46; 95% CI: 1.50-4.04; P=0.001) compared to the risk of being underweight in females whereas the risk of being overweight or obese as against normal was 57% lower (RRR=0.43; 95% CI: 0.14-1.36; P=<0.001) in males compared to the risk of being overweight or obese in females. More than quarter of the adolescents were underweight and factors such as unhealthy dietary habits, average socio-economic status, and adolescents whose mothers were unemployed were predictors of underweight.
Key words: Adolescents, dietary habit, nutritional status, overweight, underweight, obesity.
INTRODUCTION
Adolescence is a transitory period of rapid growth and maturation in human development that requires quality nutrients to support their growth spurt. Furthermore, adolescence is an intense anabolic period when the requirements for all nutrients increase. During this period, an individual achieves 20% of final adult height, 50% of adult weight and 45% increase in bone mass (Kedir et al., 2016).
The World Health Organization (WHO) identified ado-lescence as a period in human growth and development that occurs after childhood and before adulthood, from ages 10 to 19 years where physiological, psycho-social and cognitive development occurs. Many lifestyle factors including poor eating habits acquired during adolescence can lead to serious diseases later in life. Healthy eating behavior during adolescence is a fundamental pre-requisite for physical growth, psychosocial development and cognitive performance, as well as prevention of diet-related chronic diseases in adulthood. According to the 2018 Global Nutrition Report, data from 195 countries show both male and female adolescents’ obesity rates are increasing by 6.5 and 4.7%, respectively annually. Also, 15% of adolescents in Africa are overweight and obese and are at increased risk of getting diabetes and other diet related non- communicable diseases later in life (Akseer et al., 2017).
Ghana is one of the few sub-Saharan African countries at a later stage of the nutrition transition where diet changes are already affecting the health of majority of the population (Abrahams et al., 2011). These dietary intake changes among Ghanaian population were first noticed in the 1990s (Goody and Goody, 1995).
The dietary intake among adolescents in developing countries including Ghana is of concern as most traditional diets (predominantly cereal and tuber based, fresh fruits and vegetables, and foods low in fat) are gradually being replaced with more Westernized diets which lack diversity and are high in calorie-rich processed foods (Ochola and Masibo, 2014). Adolescents spend most of their time in school coupled with the autonomy to make food choices while in school making them vulnerable to sub-optimal dietary habits.
Dietary habit analysis has emerged as a useful epidemiological approach to assessing the overall diet and its relation with disease conditions. Adolescent dietary habits have been useful in understanding the occurrence of chronic diseases. Dietary habits also have an added advantage of being easily understood and used by the general population (Abizari and Ali, 2019).
In Northern Ghana, the dietary habit of adolescents is influenced by so many factors including poverty, educational environment, cultural practices, etc. Adolescents from resource-constrained households have limited access to healthy foods and health care services, which put them at higher risk of sub-optimal nutrition and dietary intake (Nikoi and Anthamatten, 2012). Adolescents who normally spend most of their time with their peers in school are usually left with no option than to eat what is available to them. A study conducted by Abiba et al. (2012)revealed that, about 73% of adolescents do not get to eat eggs and meat occasionally while 56% of them also consume both light and heavy diet as snacks.
Adolescence is a stage of human development that requires major food nutrients including protein, calcium, iron and other vitamins. These nutrients are of greater demand during adolescence than any other time in the life cycle. It is therefore believed that bone mass achieved during adolescence and young adulthood may decrease the risk of fractures and osteoporosis later in life. Consequently, failure to consume adequate diet can disrupt normal growth and development (WHO, 2003). According to the Ghana Demographic Health Survey (2014), 14% of adolescents in Ghana are underweight. Also, a study in the Northern Region revealed that, 6.3 and 6.0% of adolescents were underweight and overweight/obese, respectively (Abizari and Ali, 2019).
Nsiah-Asamoah (2017) found that adolescents who usually engaged in unhealthy dietary habits failed to meet their daily nutritional needs. A study conducted among Ghanaian Junior High School adolescents found that 62.8% usually skipped breakfast (Buxton, 2014). Similarly, a study carried out in the Northern Region also revealed that 30% skipped breakfast, 73% did not consume egg and 37% snack twice a day (Abiba et al., 2012).
Northern region is the second poorest region (50.4%) (GSS, 2014a) and has the highest burden of malnutrition (GDHS, 2014) in the country despite the fact that most non-governmental organizations in Ghana are based in Northern Ghana and have implemented several interven-tions to improve the nutritional situation of the population. This could be due to the fact that the interventions and initiatives implemented so far especially targeting adolescents are not evidence driven. Hence, the study was designed to assess dietary habits, nutritional status and associated factors among adolescents in the region to provide data that could be used in prioritizing, designing and initiating evidence- based intervention programs, aimed at improving adolescents’ nutrition.
MATERIALS AND METHODS
Study area
The study was carried out in Tamale metropolis of Northern region, which is ecologically situated in the Guinea Savannah zone. The area is characterized by drought-resistant trees such as baobab, dawadawa, shea, mango and neem. It lies between longitudes 1°E and 3°W and latitudes 9°S and 11°N of the equator. Tamale metropolis shares boundaries with Savelugu/Nantong to the North, Tolon and Kumbungu to the North West, East Gonja to the South and Yendi District to the East. The major occupation of the people is farming. Rice and maize are the main cereal crops cultivated in the area. Few farmers also cultivate yam, cassava, pepper and some other crops. Most farmers keep small ruminants as well as poultry at their backyard to supplement their crops. The area has a population of about 223,252 (GSS, 2014b), with adolescents being 46,820 representing 21% of the entire population in the metropolis. Economic activities that provide jobs for the people are very few in the study area, hence poverty is chronic. As urbanization is expanding in the region, sedentary life style, consumption of fast foods and Western diet are becoming common.
Study design
The study design used in this study is an analytical cross-sectional study design, which involves five communities and four schools. A total of 402 adolescents (10-19 years old) were covered. A semi structured questionnaire was used to generate data to answer the research question.
Sample size determination
The minimum required sample for this study was estimated using the formula for estimating single proportion as follows: 95% confidence interval, 5% margin of error and 50% prevalence as there was no known prevalence of dietary habits in adolescents in the study area.

Sampling procedure
There are 115 communities within the metropolis. A sampling frame (Data base of all the 115 communities) was formed. Excel software was used to generate random numbers for each community in the sampling frame. The communities with the random numbers from 1 to 5 were then selected (lamashegu, changli, sabonjida, aboabo and sakasaka). The metropolis also has 112 junior high schools. A sampling frame was also formed for the 112 schools and Excel was used to generate random numbers for the schools, SDA Junior High, Zogbeli Junior High, E.P Junior High and Lamashegu Junior High were selected.
Adolescents from 10 to 19 years who live within the Tamale metropolis were included in the study. Households within the communities were visited. Houses with adolescents aged 10 to 19 years were selected. Also, any adolescent who was found around these areas were also interviewed. In all, 202 adolescents were interviewed in the selected communities. Within the schools, adolescents from 10 to 19 years from each class were also selected and interviewed. For each chosen school, the list of students who fall within the inclusion criteria was obtained (that is, sample frame), and a total of 50 students were carefully chosen from each school using systematic sampling. Thus, in the four schools 200 adolescents were selected and interviewed.
Data collection methods
A semi structured questionnaire was developed for the data collection. The questionnaire consisted of both close ended and open-ended questions. Section A was structured to gather information about the respondents’ socio-demographic and economic characteristics. Section B was made up of respondents’ dietary habits. Section C contained respondents’ dietary intake whilst Section D comprised the respondents’ anthropometric data. The questionnaires were drafted in English language and translated into the local dialects for individuals who could not read or understand English. For those who could read and write (particularly the school pupils) the questionnaires were given to them to complete. However, for those who were not conformable completing the questionnaire on their own because they could not read and write the researchers administered the questionnaire to them. All the interviews were conducted using English and some selected local languages, which included Dagbani and Twi. The anthropometric data that were measured included weight, height and age. The weight of the adolescents was taken using SECA 876 electronic scale (Manufactured by SECA, United States of America). The scale was placed on a flat horizontal surface and set to zero. Participants were advised to remove any object on them that could affect the readings of their weights before mounting the scale. All adolescents were made to stand on the scale with their heads upright and hands by their sides. Readings were taken to the nearest 0.1 kg. Heights of the adolescents were also measured using the SECA 206 mechanical tape (microtoise) (Manufactured by SECA, United States of America). The microtoise was fixed to a flat vertical wall and adolescents were made to stand (without shoes) on a horizontal platform with his/her heels together.
Data analyses
Data were entered and analyzed using Statistical Package for Social Sciences (SPSS) software, version 20, Microsoft office Excel, and WHO Anthroplus.
Descriptive statistics were used to describe the socio-demographic and household characteristics of the adolescents and their parents. Means, standard deviations and ranges were calculated for continuous variables, whereas frequencies and proportions were calculated for categorical variables. Household wealth status was assessed from possession of 17 durable items including electricity, radio, color TV, black TV, satellite dish, mattress, sewing machine, refrigerator, DVD/VCD, computer, electric fan, mobile phone, bicycle, motorcycle, washing machine, animal-drawn cart, and car (GDHS 2014). Based on these, the wealth index was determined using principal component analysis (PCA) and categorized into three (3) groups (low socio-economic status (SES), middle socio-economic status and high socio-economic status). A socioeconomic score of 0-8 was considered low SES, 9-15 was considered middle SES and 16-32 was considered high SES. To score dietary diversity, the 14 food groups were regrouped into 10 food groups; starchy staples, dark green leafy vegetables, other vitamin A rich fruits and vegetables, other fruits, other vegetables, meat, poultry and fish, eggs, legumes, nuts and seeds, milk and milk products (FAO, 2021). Adolescents who consumed less than five (5) food groups were classified as consuming a ‘less diversified diet’ while adolescents who consumed five (5) food groups and above were classified as consuming a ‘diversified diet’ (FAO, 2021). Overall dietary habits were determined using meal consumption pattern and meal skipping habits. Under meal consumption pattern, a score of 0 was assigned to adolescents who consumed breakfast, lunch and supper 0-1 day/week, 1 was assigned to those who consumed breakfast, lunch and supper 2-3 days/week, 2 was assigned to those who consumed breakfast, lunch and supper 4-5 days/week and 3 was assigned to those who consumed breakfast, lunch and supper 6-7 days/week. The maximum score was 9. Under meal skipping, scores of 3, 2, 1 and 0 were given to adolescents who never skipped meals, sometimes skipped meals, quite often skipped meals and very often skipped meals, respectively. Also, adolescents who mostly skip breakfast were given a score of -1 and those who skipped any other meal (lunch and supper) were given a score of 0. Under meal skipping habits the maximum score was 3. In all the total score was 12. Adolescents who had a score of less than 5 were classified under ‘unhealthy dietary habits’ and a score of 5-12 were classified under ‘healthy dietary habits (George et al., 2014; Reedy et al., 2014; Harmon et al., 2015; USDA, 2020).
Chi-square test was done to establish the association between the dependent (nutritional status and dietary habits) and independent variables (socio-demographic factors, wealth index and dietary habits of respondents). Thereafter, all variables with P values of <0.05 were included in the logistic regression model as well as the multinomial logistic regression models. The benchmark
P value of <0.05 was selected because of its closeness to zero (0); thus it would reveal the most desired effect and improve the estimated models.
Binary and multinomial logistic regression models were estimated based on the factors established in the Chi-square to determine possible risk factors or predictors of underweight, overweight/ obesity and dietary habits of adolescents.
Level of statistical significance was set at P-value < 0.05
Ethical consideration
Ethical clearance was obtained from Kwame Nkrumah University of Science and Technology, Komfo Anokye Teaching Hospital. Consent was obtained from the participants before questionnaires were administered and all participants were assured of confidentiality.
Reliability and validity
Test-retest reliability was conducted by giving the questionnaires to same respondents and repeated for the purposes of ensuring that same or much similar results could be obtained using same questionnaires. Again, established face validity was achieved by giving the questionnaires to colleagues who better appreciate the topic to go through it and ensure that, the questions really capture the topic under investigation.
RESULTS
Background characteristics of adolescents
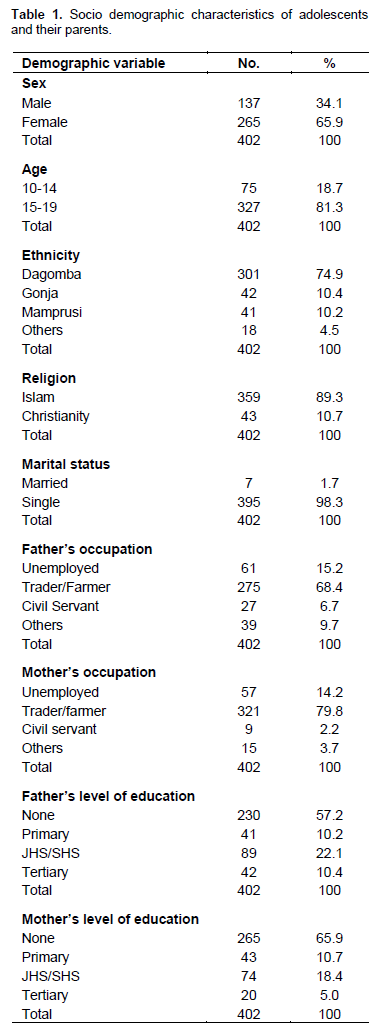
A total of 402 adolescents were recruited for the study. Out of the 402, 201 were in school adolescents while 201 were out of school adolescents. Their mean age was 15.7 ± 1.4 years. Out of the 402 adolescents, 34.1% were males and 65.9% were females. 18.7% had their ages ranging from 10-14, while 81.3% aged 15-19 years.
Majority of the adolescents interviewed were of the Dagomba ethnic group (74.9%). Greater portions (89.3%) of the respondents sampled for this survey were practicing the Islamic religion with almost all of them being single (98.3%). Out of the participants interviewed, 20.6% and 11.5% of their fathers and mothers, respectively, had completed higher than junior high school education. About 65.9 and 57.2% of mothers and fathers, respectively had no formal education. The most common occupation for mothers was trading (70.1%) while 34.8 and 33.6% of the fathers were farmers and traders, respectively (Table 1).
Dietary habits of adolescents
In investigating adolescents’ dietary practices, self-reported usual habits related to meal consumption frequency, meal skipping, snacking and out of home eating were assessed.
Meal consumption habits/meal frequency
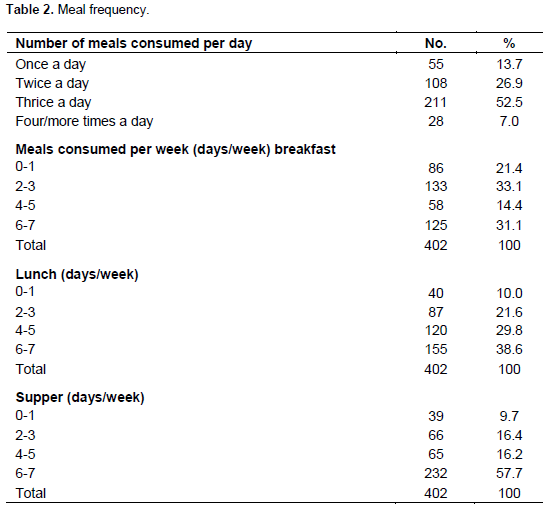
Approximately, 53% of the adolescents in Tamale reported that they usually eat 3 meals a day (Table 2). The remaining reported consuming 2 meals (26.9%) or more than 3 meals (7.0%) a day. The proportion of adolescents who consumed breakfast, lunch and dinner during a typical week, was 31.1, 38.6 and 57.7%, respectively (Table 2).
Meal skipping
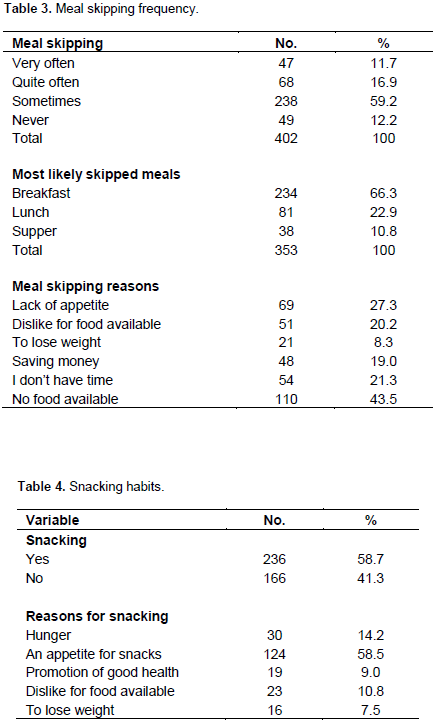
About 12% of the adolescents indicated that they often skipped meals whilst 12.2% never skipped meals. It was found that the most frequently skipped meal was breakfast (66.3%) while supper was the least meal frequently skipped (10.8%). The main reasons for meal skipping included food unavailability (43.5%), lack of appetite (27.3%), lack of time (21.3%), dislike for food (20.2%), saving money (19.0%) and losing weight (8.3%) (Table 3).
Snacking habits
Majority (58.7%) of the adolescents in the study were found to have a habit of snacking. The main reasons for snacking comprised an appetite for snacks (58.5%), hunger (14.2%), dislike for available food (10.8%), promotion of good health (9.0%) and to lose weight (7.5%). Snacks that were most frequently consumed in a typical week as reported by the adolescents were carbonated soft drink (24.9%), vegetables (18.7%), cookies/biscuits (15.2%) and toffees (10.9%) (Table 4).
Purchased meals (out of home eating)
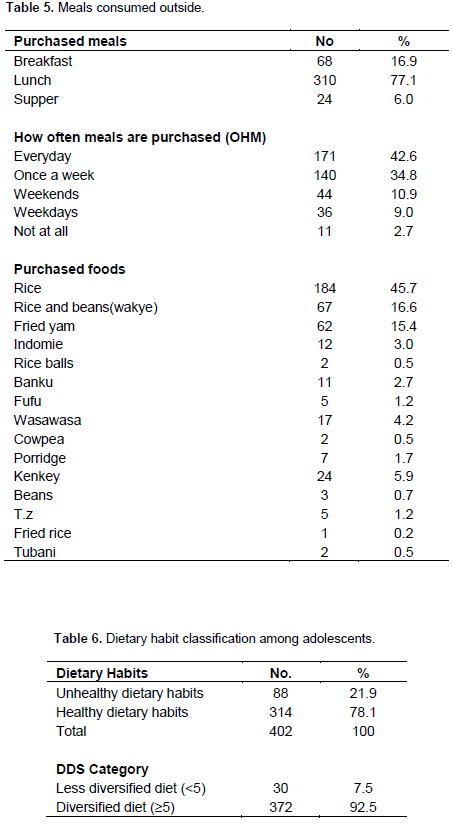
Lunch was consumed by majority (77.1%) of adolescents outside the home, with the least purchased meal being supper (6.0%). 42.6% of the adolescents ate outside their home every day, 34.8% ate outside their home once a week, 10.9% ate outside their home every weekend, 9.0% ate outside their home during weekdays and 2.7% never ate outside. Adolescents also mentioned rice, rice and beans (wakye), kenkey, wasawasa, fried yam, indomie, fufu, banku, Tuozafi (TZ), rice balls and cowpea as foods normally consumed out of home. The majority (45.7%) purchased rice whilst only 0.2% purchase fried rice (fried rice) (Table 5).
Dietary diversity category
On the whole, 21.9% of the adolescents who participated in the present study had poor or unhealthy dietary habits compared to 78.1% who had healthy dietary habits. Adolescent mean dietary diversity score in this study was 7.8±2.4. Majority (92.5%) of the adolescents in the metropolis consumed a diversified diet and 7.5% of the adolescents consumed a less diversified diet (Table 6).
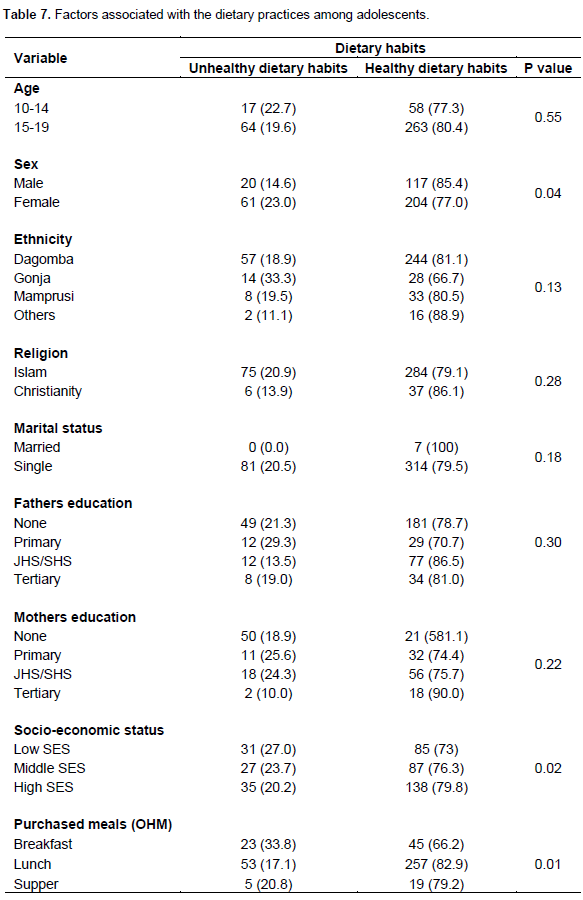
Factors associated with dietary habits among adolescents
Results from the study showed that 21.6% of persons from average socio-economic status compared to 44.8% from high socioeconomic status and 13.4% of low socioeconomic status had good dietary habits. Also 29.1% of males compared to 50.7% of females had good dietary habits. Socio-economic status (p=0.02), gender (p=0.04) and purchased meals (p=0.01) (out of home eating) were significant factors associated with the dietary habits of adolescents in Tamale metropolis (Table 7).
Predictors of dietary habits among adolescents
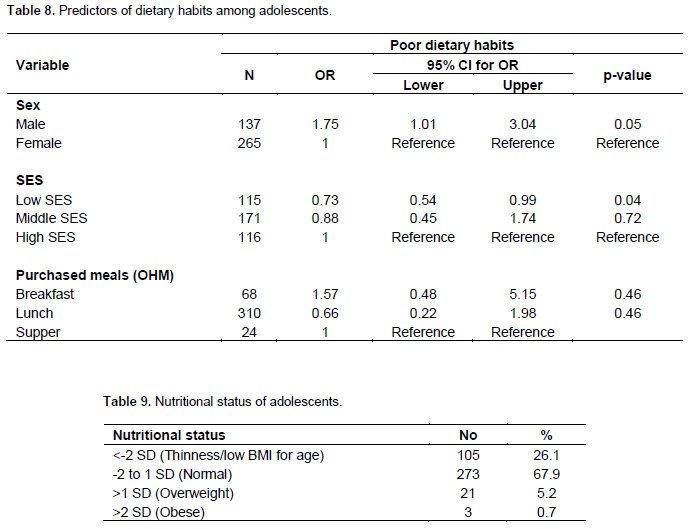
Low socio-economic status was a significant predictor of dietary habits. Adolescents with caregivers/parents of low socio-economic status were 27% less likely to practice unhealthy dietary habits compared to those with parents/caregivers of high socio-economic status (OR=0.73; 95%CI: 0.54-0.99; P=0.04) (Table 8).
Nutritional status of adolescents
Approximately, 26.1% of the adolescents in Tamale metropolis were underweight, 67.9% normal, 5.2% overweight and 0.7% obese (Table 9).
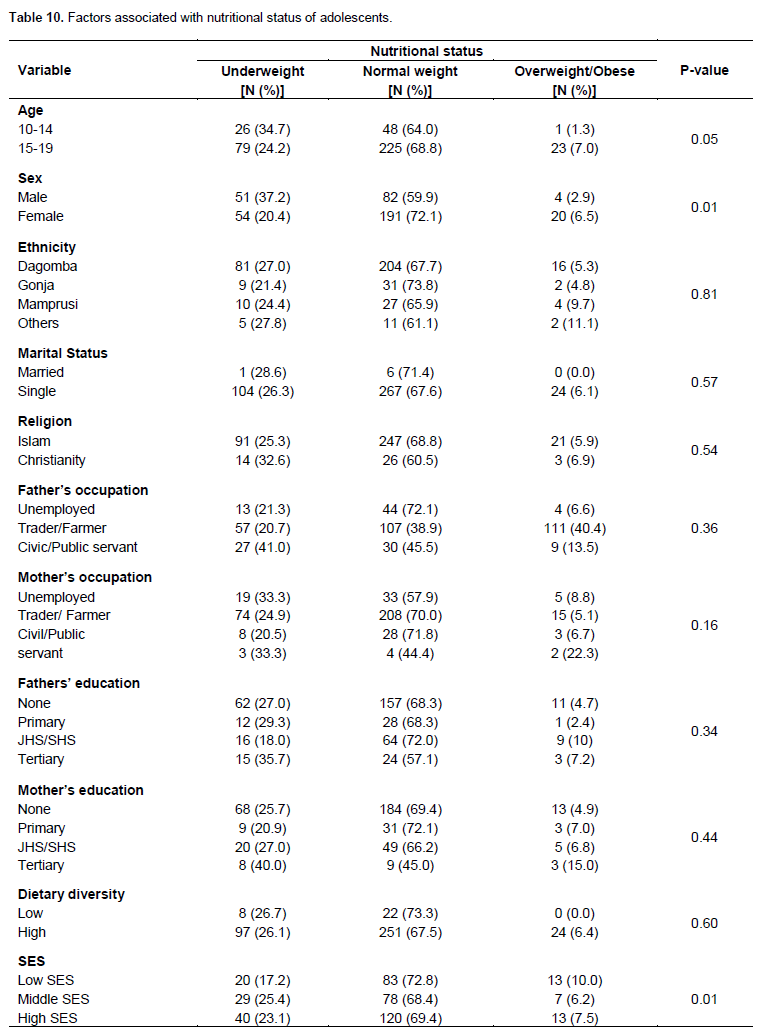
Factors associated with nutritional status of adolescents
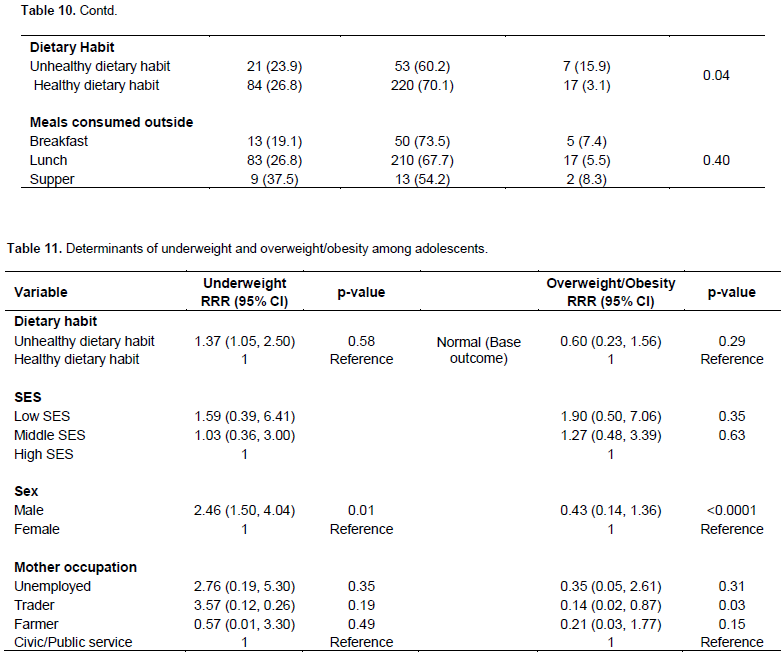
Results from this study showed that the sex of adolescent (p=0.01), household socio-economic status (p=0.01) and dietary habits (p=0.04) were statistically and significantly associated with the nutritional status of the adolescents. It was observed that 37.2% of the adolescents (males) were underweight compared to 20% of the females; whereas, 6.5% of the adolescent females were overweight/obese compared to 2.9% of males. Also, 25.4% of the adolescents from the middle socio-economic households were underweight compared to 23.1 and 17.2% of the adolescents from the middle and low socio-economic households, respectively; while 10.0% of the adolescents from low socio-economic households were overweight/obese compared to 6.2 and 7.5% of those in middle and high socio-economic households, respectively. Lastly, 26.8% of the adolescents who had healthy dietary habits were underweight compared to 23.9% of those who practiced unhealthy dietary habits; 15.95 of the adolescents who practiced unhealthy dietary habits were overweight compared to 3.1% of those who practiced healthy dietary habits (Table 10).
Determinants of underweight and overweight/obesity
The risk of adolescents being underweight as against normal in males was 2.46 times higher (RRR=2.46; 95% CI: 1.50-4.04; P=0.001) compared to the risk of being underweight in females; whereas, the risk of being overweight or obese as against normal was 57% lower (RRR=0.43; 95% CI: 0.14-1.36; P=<0.001) in males compared to the risk of being overweight or obese in females. Moreover, the risk of being overweight/obese as against normal in adolescents whose mothers were traders was 86% lower (RRR=0.14; 95% CI: 0.02-0.87; P=0.03) compared to the risk of being overweight or obese in adolescents whose mothers were employed as civil or public servants (Table 11).
DISCUSSION
Usual meal frequency and purchased meals (out of home eating)
More than 50% of adolescents reported eating 3 times a day during a typical day. According to FAO (2004a), school children and adolescents’ daily meals should be composed of 3 meals and some snacks. This result is consistent with that of the findings of Kotecha et al. (2013) who found, in their study on determining the dietary pattern of school going adolescents in urban Baroda, that majority (55%) of adolescents consumed three meals daily. However, Hoffmann et al. (2012)’s study on the dietary behaviors of adolescents, from urban and rural areas in the district of Szamotuly, Poland revealed that 39.7% adolescents ate 3 times daily.
In spite of breakfast being an important meal, it was interesting to note that adolescents always eat both lunch (38.6%) and supper (57.7%) more than breakfast (31.1%). Similar finding was made by Agnieszka et al. (2016) who showed that adolescents eat lunch and dinner more often than breakfast. Also, Pendergast et al. (2016) found that more adolescents skipped breakfast (62.8%) than lunch (40.2%) or supper (35.1%).
Purchased meals (out of home eating) were part of the measures of the dietary habits of the adolescents. Majority of the adolescents indicated they eat from home, mostly lunch. During the afternoons, adolescents are mostly found in school or left behind at home by their parents. As a result, adolescents mostly eat foods outside their home. The type and quantity of food eaten by an individual has an effect on his/her well-being and hence eating properly at meal times at this stage of life is very vital in achieving optimum growth (Stang and Story, 2005). Eating out of home frequently has been associated with lower intake of fruits and vegetables (Seguin et al., 2016). Similar to this finding, a study conducted by Feeley et al. (2012), on the changes in dietary habits and eating practices of adolescents living in urban South Africa revealed that, out of the 655 participants almost all participants eat more than one fast-food item per week (95 and 92.2% for males and females, respectively).
Meal skipping and snacking habits
The results also revealed that majority of the adolescents skipped breakfast and the least skipped meal was supper, which is consistent with the findings of Akman et al. (2010). Breakfast skipping and meals in general is a typical habit of adolescents. According to other researchers, this habit increases as the adolescents get older (Monzani et al., 2019). Similarly, a study conducted by Aganah (2014)on the dietary practices and nutritional status of adolescent girls in Ko Senior High Boarding School in the Upper West Region of Ghana revealed that 50.6% of adolescent girls skipped breakfast. Also, a study conducted by Badrasawi et al. (2021), on reasons for skipping breakfast among adolescents in Palestinia also showed that breakfast was often skipped by adolescents. In addition, Onyiriuka et al. (2013) revealed that meal skipping particularly breakfast, eating of fast foods, soft drinks and low consumption of fruits and vegetables were the key eating habits showed among adolescent girls in Nigerian urban secondary school.
Several studies consistently relate consumption of breakfast to improvements in academics. For example, Adolphus et al. (2013) found that increased frequency of habitual breakfast was consistently positively associated with academic performance and task behavior in the classroom. Breakfast consumption is associated with positive outcomes for diet quality, micronutrient intake, weight status and lifestyle factors (Adolphus et al., 2013). An individual who skips breakfast misses some very important dietary needs that are not usually compensated for in other meals. In fact, adolescents who skip breakfast have significantly lower vitamin and mineral intake compared to those that regularly eat breakfast (Matsumoto et al., 2020).
In this study, snacking was also reported by majority of the adolescents as part of their eating habits. This finding of the present study is similar to a study done by Przyslawski et al. (2011), which was conducted on female adolescents from the Great Poland Region. The study found that nearly half of the adolescents (46%) reported that they snacked between main meals.
When asked about their snack intake during a typical week, majority of the adolescents indicated that they consumed carbonated soft drinks, followed by pastries and toffees. These food items are high-caloric, energy-dense foods containing high quantities of sugar and fats which increase the risk of becoming overweight and obese or risk of chronic disease like diabetes, later on in life. Only a few adolescents consumed fruits and vegetables (Monzani et al., 2019). The findings of this study suggested that, parents may not be providing fruits and vegetables often at home. Evidence available showed that, among adolescents, taste is a main reason for not liking fruits and vegetables, especially vegetables (Zeinstra et al., 2007). Among the reasons mentioned by the adolescents for snacking, appetite for snack was the major reason for snacking. It has also been reported that most adolescents choose their diet on the basis of taste rather than nutrition (Lassi et al., 2017).
The study shows that the participants skipped breakfast more than any other meal, which is found to be unhealthy behavior with consequences. For example, studies have shown that skipping breakfast is associated to unhealthy behaviors, poorer diets, and lower physical activity and also with a higher metabolic risk, that is, higher body mass index (BMI), larger waist circumference, higher fasting insulin and increased cholesterol and LDL levels (Ruxton and Kirk, 1997; Song et al., 2005; Timlin et al., 2008; Van der Heijden et al., 2007).
Nutritional status of adolescents in Tamale metropolis
BMI for age Z-score (BAZ) gave an indication of the long-term impact of nutrition on the growth of children and adolescents. The results reveal that most adolescents had a normal BMI for age. This indicated that majority of the adolescents in Tamale metropolis are within -2 to 1 SD, according to WHO criteria (WHO, 1995; de Onis et al., 2007). Also, about a handful of the adolescents were underweight, while only a few were overweight and
obese.
The prevalence of underweight in this study is similar to others found elsewhere. For instance, Yohannes et al. (2015) reported that the underweight prevalence of 26.1% among adolescent students in Northern Ethiopia. However, the magnitude of underweight in this study is lower than the 28% reported in India (Bhargava et al., 2020). The discrepancy might be due to the implementation of a battery of interventions such as the school health programme in Ghana.
Evidence available showed that between 1975 and 2016, globally obesity prevalence increased from 0.7 to 5.6% in girls and from 0.9 to 7.8% in boys (Di Cesare et al., 2019). The global proportions of obesity are similar to the one (5.9%) found in the present study, which confirmed the double burden of malnutrition currently experienced in low and middle in-come countries.
However, the prevalence found in the present study is relatively low compared to the one found (12.9%) in the study conducted in Ethiopia (12.9%) (Gebrie et al., 2018), but higher than that of Abiba et al. (2012) who found 4% prevalence of overweight among upper primary school children (adolescents) in Tamale metropolis, Ghana. Moreover, Otuneye et al. (2017) established that there is 2.8% prevalence rate of obesity among adolescents in Abuja municipal area council of Nigeria.
Predictors of overweight/obesity among adolescents in Tamale metropolis
The present study found sex of adolescents and adolescents’ mothers’ occupation (trading vs. civil or public servants) as the main predictors of adolescents’ nutritional status. The finding in the present study is consistent with the findings of a meta-analysis conducted by Gebrie et al. (2018) who showed that sex of adolescents was associated with overweight or obesity. Similarly, a study conducted by Worku et al. (2021), among adolescent in Ethiopia showed that adolescents whose mothers are employed by government were almost 6.5 times more likely to be overweight and obese.
CONCLUSION
Based on the findings of this study, it can be concluded that meal skipping particularly breakfast was the main unhealthy eating habit observed among adolescents in Tamale metropolis, with majority of adolescents within the Tamale metropolis practicing a healthy dietary habit.
Moreover, the 24-h recall conducted in the study showed that majority of the adolescents consumed a diversified diet with only less than a tenth consuming a less diversified diet.
Finally, this study again indicated that most socio-demographic characteristics did not predict significantly dietary habits except socio-economic status. Conversely, dietary habit, socio-economic status, and sex were statistically and significantly associated with the nutritional status of adolescents in Tamale metropolis.
However, only sex and maternal occupation (trading vs public/civil servant) was the only predictors of the adolescents’ nutrition status.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abiba A, Grace ANK, Kubreziga KC (2012). Effects of dietary patterns on the nutritional status of upper primary school children in Tamale metropolis. Pakistan Journal of Nutrition 11(7):591-609. |
|
|
Abizari AR, Ali Z (2019). Dietary patterns and associated factors of schooling Ghanaian adolescents. Journal of Health, Population, and Nutrition 38(1):5. |
|
|
Abrahams Z, McHiza Z, Steyn NP (2011). Diet and mortality rates in Sub-Saharan Africa: Stages in the nutrition transition. BMC Public Health 11(1):801. |
|
|
Adolphus K, Lawton CL, Dye L (2013). The effects of breakfast on behavior and academic performance in children and adolescents. Frontiers in Human Neuroscience 7:425. |
|
|
Aganah CA (2014). Dietary Practices And Nutritional Status Of Adolescent Girls In Ko Senior HighBoarding.[MPHIL Thesis, University of Ghana]. |
|
|
Akman M, Akan H, ?zbirak G, Tanr?över Ö, Tilev SM, Y?ld?z A, Tekta? S, Vitrinel A, Hayran O (2010). Eating patterns of Turkish adolescents: a cross-sectional survey. Nutrition Journal 9:67. |
|
|
Akseer N, Al-Gashm S, Mehta S, Mokdad A, Bhutta ZA (2017). Global and regional trends in the nutritional status of young people: a critical and neglected age group. Annals of the New York Academy of Sciences 1393(1):3-20. |
|
|
Badrasawi M, Anabtawi O, Al-Zain Y (2021). Breakfast characteristics, perception, and reasons of skipping among 8th and 9th-grade students at governmental schools, Jenin governance, West Bank. BMC Nutrition 7:42. |
|
|
Bhargava M, Bhargava A, Ghate SD, Rao R (2020). Nutritional status of Indian adolescents (15-19 years) from National Family Health Surveys 3 and 4: Revised estimates using WHO 2007 Growth reference. PloS One 15(6):e0234570. |
|
|
Buxton CNA (2014). Ghanaian Junior High School Adolescents Dietary Practices and Food Preferences: Implications for Public Health Concern. Journal of Nutrition and Food Sciences 4:5. |
|
|
Cochran WG (1977). Sampling Techniques. 3rd Edition. John Wiley & Sons, New York. |
|
|
De Onis M, Onyango AW, Borghi E, Siyam, A., Nishida, C., & Siekmann J (2007). Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization 85(9):660-667. |
|
|
Di Cesare M, Sori? M, Bovet P. Miranda JJ, Bhutta Z, Stevens GA, Laxmaiah A, Kengne AP, Bentham J (2019). The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action. BMC Medicine 17:212. |
|
|
Feeley A, Musenge E, Pettifor JM, Norris SA (2012). Changes in dietary habits and eating practices in adolescents living in urban South Africa: the birth to twenty cohort. Nutrition (Burbank, Los Angeles County, Calif.) 28(7-8):e1-e6. |
|
|
Food and Agricultural Organization (FAO) (2021). Minimum dietary diversity for women. Rome. |
|
|
Food and Agricultural Organization (FAO) (2004a). Human Energy Requirements Report of a Joint Expert Consultation. Food and Agricultural Organization, Rome Available at: |
|
|
Gebrie A, Alebel A, Zegeye A (2018). Prevalence and associated factors of overweight/ obesity among children and adolescents in Ethiopia: a systematic review and meta-analysis. BMC Obesity 5(1):1-2. |
|
|
George SM, Ballard-Barbash R, Manson JE, Reedy J, Shikany JM, Subar AF, Tinker LF, Vitolins M, Neuhouser ML (2014). Comparing indices of diet quality with chronic disease mortality risk in postmenopausal women in the women's health initiative observational study: evidence to inform national dietary guidance. American Journal of Epidemiology 180(6):616-625. |
|
|
Ghana Statistical Service (GSS) (2014a) District Analytical Report-2010 Population and Housing Census. Ghana Statistical Service. |
|
|
Ghana Statistical Service (GSS) (2014b). Ghana Health Service (GHS), and ICF Macro. Ghana Demographic and Health Survey 2014. Accra, Ghana: GSS, GHS, and ICF Macro; 2014. |
|
|
Ghana Demographic and Health Survey (GDHS) (2014). Accra, Ghana: GSS, GHS, and ICF Macro; 2014. |
|
|
Goody J, Goody E (1995). Food and Identities: Changing Patterns of Consumption in Ghana. Journal of Cambridge Anthropology 18:1-14. |
|
|
Harmon BE, Boushey CJ, Shvetsov YB, Ettienne R, Reedy J, Wilkens LR, Le Marchand L, Henderson BE, Kolonel LN (2015). Associations of key diet-quality indexes with mortality in the Multiethnic Cohort: the Dietary Patterns Methods Project. The American Journal of Clinical Nutrition (3):587-597. |
|
|
Hoffmann K, Bryl W, Marcinkowski JT, Rzeso? A, Wojty?a E, Pupek-Musialik D (2012). Dietary behaviours of adolescents from urban and rural areas in the district of Szamotu?y--a preliminary study. Annals of Agricultural and Environmental Medicine 19(1):103-107. |
|
|
Przyslawski J, Stelmach M, Grygiel-Górniak B, Mardas M, Walkowiak J (2011). Dietary habits and nutritional status of female adolescents from the Great Poland Region. Polish Journal of Food and Nutrition Sciences 61(1):73-78. |
|
|
Kedir H, Berhane Y, Worku A (2016). Magnitude and determinants of malnutrition among pregnant women in eastern Ethiopia: evidence from rural, community-based setting. Maternal and Child Nutrition12:51-63. |
|
|
Kotecha PV, Patel SV, Baxi RK, Mazumdar VS, Shobha M, Mehta KG, Mansi D, Ekta M (2013). Dietary pattern of school going adolescents in urban Baroda, India. Journal of Health, Population, and Nutrition 31(4):490-496. |
|
|
Lassi Z, Moin A, Bhutta Z (2017). Nutrition in Middle Childhood and Adolescence. In: Bundy DAP, Silva Nd, Horton S, (ed s). Child and Adolescent Health and Development. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 20. Chapter 11. |
|
|
Matsumoto M, Hatamoto Y, Sakamoto A, Masumoto A, Ikemoto S (2020). Breakfast skipping is related to inadequacy of vitamin and mineral intakes among Japanese female junior high school students: a cross-sectional study. Journal of Nutritional Science 9:e9. |
|
|
Monzani A, Ricotti R, Caputo M, Solito A, Archero F, Bellone S, Prodam F (2019). A systematic review of the association of skipping breakfast with weight and cardiometabolic risk factors in children and adolescents. What should we better investigate in the future? Nutrients 11(2):387. |
|
|
Nikoi E, Anthamatten P (2012). An examination of environmental correlates with childhood height-for-age An examination of environmental correlates with childhood height-for-age in Ghana. Journal of Public Health Nutrition 16(1):46-53. |
|
|
Nsiah-Asamoah C (2017). Healthy eating and its barriers: Perceptions and practices of adolescents in Ghana. Journal of Advances in Nutrition and Food Science 2(1):1-10. |
|
|
Ochola S, Masibo PK (2014). Dietary intake of schoolchildren and adolescents in developing countries. Annals of Nutrition and Metabolism 64(Suppl 2):24-40 |
|
|
Onyiriuka AN, Ibeawuchi AN, Onyiriuka RC (2013). Assessment of eating habits among adolescent Nigerian urban secondary schoolgirls. Sri Lanka Journal of Child Health 42(1):20-26. |
|
|
Otuneye AT, Ahmed PA, Abdulkarim AA, Aluko OO, Shatima DR (2017). Relationship between dietary habits and nutritional status among adolescents in Abuja municipal area council of Nigeria. Nigerian Journal of Paediatrics 44(3):128-135. |
|
|
Pendergast FJ, Livingstone KM, Worsley A, McNaughton SA (2016). Correlates of meal skipping in young adults: a systematic review. The International Journal of Behavioral Nutrition and Physical Activity 13(1):125. |
|
|
Reedy J, Krebs-Smith SM, Miller PE, Liese AD, Kahle LL, Park Y, Subar AF (2014). Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. Journal of Nutrition 144(6):881-889. |
|
|
Ruxton CH, Kirk TR (1997). Breakfast: A review of associations with measures of dietary intake, physiology and biochemistry. British Journal of Nutrition 78(2):199-213. |
|
|
Seguin RA, Aggarwal A, Vermeylen F, Drewnowski A (2016). Consumption frequency of foods away from home linked with higher body mass index and lower fruit and vegetable intake among adults: A cross-sectional study. Journal of Environmental and Public Health 2016(6):1-12. |
|
|
Song WO, Chun OK, Obayashi S, Cho S, Chung CE (2005). Is consumption of breakfast associated with body mass index in US adults? Journal of the American Dietetic Association 105:1373-1382. |
|
|
Stang J, Story M (2005). Chapter 1: Adolescent growth and development. Guidelines for adolescent nutrition services. Minneapolis." MN Center for Leadership, Education and training in maternal and child nutrition, Division of epidemiology and community health, school of public health, university of Minnesota. |
|
|
Timlin MT, Pereira MA, Story M, Neumark-Sztainer D (2008). Breakfast eating and weight change in a 5-year prospective analysis of adolescents: Project EAT (eating among teens). Pediatrics 121:e638-e645. |
|
|
United States Department of Agriculture (USDA) (2020). Dietary Guidelines Advisory Committee. 2020. Scientific Report of the 2020 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services. U.S. Department of Agriculture, Agricultural Research Service, Washington, DC. |
|
|
Van der Heijden AA, Hu FB, Rimm EB, van Dam RM. (2007). A prospective study of breakfast consumption and weight gain among U.S. men. Obesity 15(10):2463-2469. |
|
|
World Health Organization (WHO) (1995). Physical status: the use and interpretation of anthropometry. Geneva: WHO; 1995. WHO Technical Report Series no 854. |
|
|
World Health Organization (WHO) (2003). Diet, nutrition and the prevention of chronic diseases: report of a Joint WHO/FAO Expert Consultation. WHO Technical Report Series, No. 916. Geneva: |
|
|
Worku M, Gizaw Z, Kassahun Belew A, Wagnew A, Hunegnaw MT. (2021). Prevalence and associated factors of overweight and obesity among high school adolescents in Bahir Dar City, Northwest, Ethiopia: A cross sectional study. Journal of Obesity (1):1-8. |
|
|
Zeinstra GG, Koelen MA, Kok FJ, Graaf C De (2007). Cognitive development and children's perceptions of fruit and vegetables; A qualitative study. International Journal of Behavioral Nutrition and Physical Activity 4:30. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


