Full Length Research Paper

ABSTRACT
Multidrug-resistant tuberculosis is involved in multiple haematological manifestations, including anaemia. The objective was to determine the prevalence of anaemia and associated factors in patients with drug-resistant TB. This was a 3-year longitudinal cohort study of patients affected by multidrug-resistant tuberculosis followed up monthly for 9 months by the WHO standardized short treatment regimen in three large multidrug-resistant tuberculosis centres in Conakry. Data were collected using a drug-resistant TB registry form. frequencies were used, means (standard deviation) for data description, and multivariate logistic regression to find factors associated with anaemia. A total of 218 patients were included, mostly men (68.3%), the mean age was 34 years, living mainly in urban areas (77.5%). 23% were seropositive for HIV, 82.6% of patients had already been infected. Anaemia was noted in 71% of patients. In multivariate analysis, HIV-positive patients were more likely to have anaemia (p_value <0.001) as well as vomiting (p_value = 0.049). The results of the biology showed an influence of the leukocyte level (p_value = 0.006) and the platelet count (p_value = 0.043). Anaemia is frequent in multidrug-resistant tuberculosis, serological status, antecedents of antituberculosis treatment, functional and laboratory signs were the factors associated with anaemia.
Key words: Anaemia, TBMR, Guinea.
INTRODUCTION
Tuberculosis (TB) is a major public health problem affecting nearly 10 million people worldwide and causing approximately two million deaths per year (WHO, 2017). In addition, it is involved in multiple haematological manifestations, including anaemia (Metanat et al., 2020). Tuberculosis is present in all regions of the world. In 2019, it affected 5.6 million men, 3.2 million women, and 1.2 million children. The WHO Region with the highest number of new TB cases was South-East Asia (44% of all new cases), followed by the African Region (25%) and the Western Pacific Region (18%) (Rapport 2019; de lRapp sur la tuberculose, n.d.).
As for anaemia, it is estimated that about a quarter of the world's population has lower than normal haemoglobin levels. Its occurrence during certain infectious diseases such as HIV infection would promote their development or increase mortality (Lee et al., 2006; Isanaka et al., 2012). This multifactorial problem includes inhibiting erythropoiesis by pro-inflammatory cytokines, nutritional deficiencies, iron use defects, and bone marrow aplasia (Metanat et al., 2020).
The anaemia seen in tuberculosis can manifest itself in several forms. Although it is moderate in the vast majority of cases, sometimes it can resemble pernicious anaemia (Jonsson., 2009). In addition, cases of hemolytic anaemia are reported, which may be infectious, toxic, or autoimmune (Eschapasse et al., 2017).
In a 2018 study in India, the authors reported a 71.83% prevalence of anaemia in tuberculosis patients (Mukherjee et al., 2019). In Brazil, this prevalence was of the order of 85.6% and is believed to be due to the association of an HIV infection, particularly those who had a weight loss, a collapsed CD4 count, a high viral load, and ARV treatment. pre-TB (Demitto et al., 2020). In Guinea, it is assumed that the prevalence of anaemia is also high during tuberculosis infection, whether or not associated with HIV. However, to our knowledge, few studies have been interested in the question, which motivated the realization of this present work. The objective was to determine the prevalence of anaemia in tuberculosis patients in the service and identify its factors.
METHODS
Study setting and population
Surveillance data were analyzed from 218 patients with drug-resistant TB recruited between 2016 and 2018 in a multicentre longitudinal cohort study conducted at Guinea's main multidrug-resistant tuberculosis treatment centers. According to the WHO standardized regimen, all patients were seen initially and followed monthly for 9 months (WHO treatment guidelines for drug-resistant tuberculosis, 2016 update, n.d.). Patients under 18 years were excluded from the analysis.
The authors collected concerned socio-demographic and clinical characteristics, laboratory test results (sputum smear and blood count) and x-rays for all registered patients in treatment centers. Additional details were gathered from records and results reports. The following clinical, paraclinical, and demographic data were extracted: age, sex, place of residence, comorbidity, HIV status, history of tuberculosis due to previously treated tuberculosis, presence of cavities on the chest x-ray, determined by the principal radiologist, data reference on weight, height for the calculation of the BMI.
Definitions of anaemia
The following World Health Organization (WHO) criteria were used to rank the severity of anaemia:
1. No anaemia (haemoglobin [Hb]> 13.0 g / dL for men, 12.0 g / dL for women),
2. Mild anaemia (11.0-12.9 g / dL for men, 11.0-11.9 g / dL for women),
3. Moderate anaemia (8.0-10.9 g / dL for men and women)
4. Severe anaemia (<8.0 g / dL for men and women).
Potential predictors of anaemia are socio-demographic (sex, age); clinical (cough, dyspnoea, chest pain, night sweats, nausea, vomiting, HIV status, history of antituberculosis treatment, depression, adherence, results of treatment) and paraclinical (number of colonies per initial smear, the initial number of colonies count smear, initial culture, radiography).
Statistical analysis
Frequencies (percent) or means (standard deviation; SD) describe categorical and continuous variables. Univariate and multivariate logistic regression was used to identify predictors of anaemia among DR-TB patients; all variables with a p-value less than 0.1 were considered for multivariate regression. Odds ratios (OR) with 95% intervals (95% CI) were used as association parameters, and the level of significance was p less than 5%. The hypothesis of proportionality and log-linearity risk has been verified.
RESULTS
A total of 218 patients were included. The patients were mainly men (68.3%) and women (31.6%). The mean age of the patients was 33.7± 11 years; most lived in urban areas (77.5%). Fifty-one patients (23%) were HIV positive, 36 of whom (72%) had a BMI <18.5 (Table 1).

According to the patient category, 38 patients (17.4%) were new cases of DR-TB, and 180 patients (82.6%) had already been infected. New cases of DR-TB and 180 patients (82.6%) had already received first-line antituberculosis treatment. Among the authors’ patients, they noted 71% anaemia (Table 2).
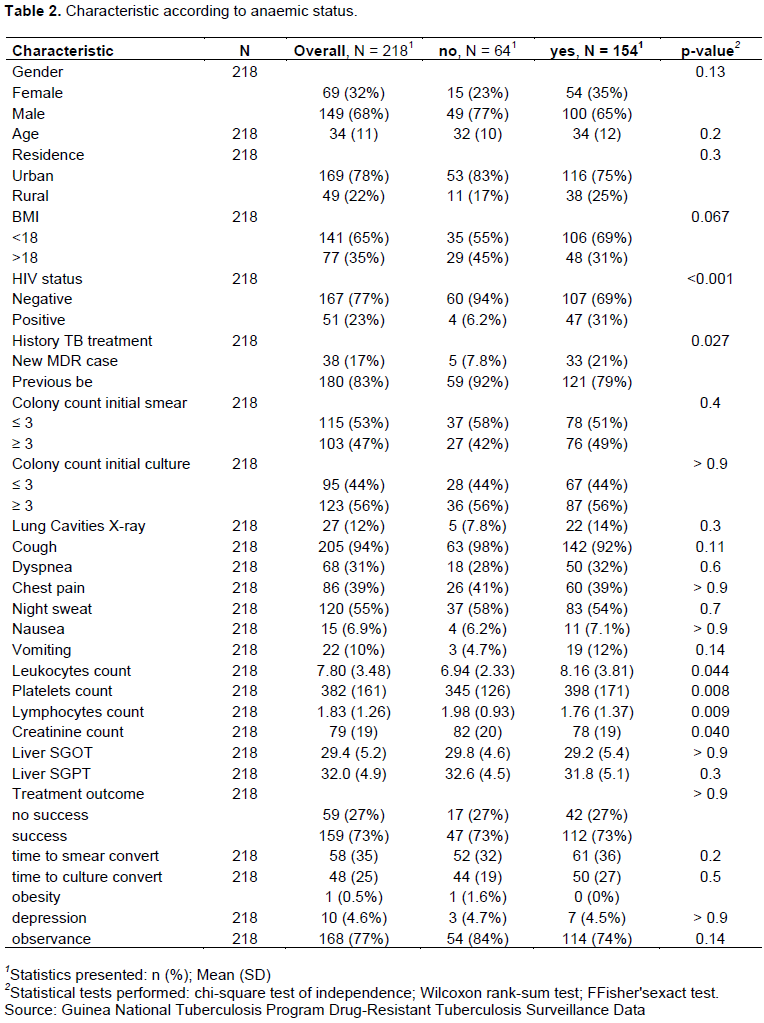
On univariate analysis (Table 3), the occurrence of anemia was associated with serological status (p_value <0.001), history of treatment for TB (p_value = 0.027); biologically, leukocyte count (p_value = 0.04), platelet count (p_value = 0.008, lymphocyte count (p_value = 0.009), and creatinemia (p_value = 0.040) were associated with the occurrence of 'anemia. On multivariate analysis (Table 3), seropositive patients were less likely to have anemia (p_value <0.001) as well as vomiting (p_value = 0.049). The results of the biology showed an influence of the leukocyte level (p_value = 0.006) and the platelet level (p_value = 0.043).


DISCUSSION
The emergence of MDR-TB is a serious global threat to TB control. Treatment of this disease is a challenge because it typically requires longer-treatment regimens using second-line anti-TB drugs that are more toxic than drug-sensitive tuberculosis. The results showed that around three-quarters of patients followed for multidrug-resistant tuberculosis were anaemic. In an earlier study carried out in Iran (Metanat et al., 2020), the authors had reported a frequency of anaemia of the order of 54.5% in tuberculosis patients; the result is close to that reported in Brazil, 89.1% of anaemia (Oliveira et al., 2014). Moreover, in the study by Gil-Santana L et al. (Gil-Santana et al., 2019), Hemoglobin levels did not change substantially with increasing AFB smear grade when all patients were considered. This frequency could be explained by the evolution of certain multiresistant forms that have benefited from a long treatment before developing resistance.
The patients studied had a variable profile. In another study, young adults were the most affected age category (average age of the patients was 33.7 years), consistent with other African series, particularly in Gabon (Kombila et al., 2019), In Congo Brazzaville (RRDDI et al., 2020). For retroviral serology, nearly one in four patients (23%) was seropositive, TBM-R and HIV coinfection was reported in several series. It was 42.3% in that Kombila et al. (Kombila et al., 2019)in Gabon, 18% in Togo (Adambounou et al., 2020). Based on the BMI, 72% were underweight (<18.5); this observation is close to Oliviera et al. (Oliveira et al., 2014), which reported 68.7% underweight patients. Depending on the category of patients, our result is close to that of Régis et al.(RRDDI et al., 2020)in Congo; Brazzaville reported previous tuberculosis in 88.6% of MDR-TB patients moreover in Adambounou et al. (Adambounou et al., 2020)study, 5.2% of retreatment cases and 2% among new cases.
Among the factors associated with anaemia, serological status alone has been documented in the medical literature as a provider of anaemia; it results from a direct action of the virus, opportunistic conditions and/or antiretroviral treatment (Attinsounon et al., 2017; Fall et al., 2017). However, apart from HIV status, vomiting, increased leukocyte, platelet, and lymphocyte levels were significantly associated with the occurrence of anaemia in patients with multidrug-resistant tuberculosis (P-Value <0.005). Unlike ours, the series from Oliveira et al. (Oliveira et al., 2014)reports an association of anaemia with the male gender (p = 0.03) and BMI (p = 0.0004).
REFERENCES
|
Attinsounon CA, Dovonou CA, Alassani CA, Gomina M, Agbodandé KA, Wanvoegbe FA, Zannou DM (2017). Prévalence et facteurs associés à l'anémie chez les adultes infectés par le VIH à l'initiation du traitement antirétroviral. Médecine et Maladies Infectieuses 47(4):S135-S136. |
|
|
Demitto FO, Araújo-Pereira M, Schmaltz CA, Sant'Anna FM, Arriaga MB, Andrade BB, Rolla VC (2020). Impact of persistent anemia on systemic inflammation and tuberculosis outcomes in persons living with HIV. Frontiers in immunology 11:588405. |
|
|
Eschapasse E, Khatchatourian L, Biron C, Brochard J, Raffi F, Lefevre M, Boutoille D (2017). Deux cas d'anémies hémolytiques auto-immunes inaugurales de tuberculose pulmonaire bacillifère. Médecine et Maladies Infectieuses 47(4):S103. |
|
|
Fall S, Djiba B, Diagne N, Ndiaye M, Dieng F, Kyelem EMC, Ndiaye FSD (2017). Profil des manifestations hématologiques de l'infection à VIH chez l'adulte?: Etude monocentrique de 262 observations sénégalaises. Rev. Afr. Médecine Interne 4:33-36. |
|
|
Isanaka S, Mugusi F, Urassa W, Willett WC, Bosch RJ, Villamor E, Fawzi WW (2012). Iron deficiency and anemia predict mortality in patients with tuberculosis. The Journal of nutrition 142(2):350-357. |
|
|
Kombila UD, Toure NO, Nzengue EE, Mounguengui D, Mackanga JR, Ba JI, Boguikouma JB (2019). Comportements et attitudes des élèves sages-femmes de Libreville vis-à-vis du tabagisme. Revue des Maladies Respiratoires 36(3):342-349. |
|
|
Lee SW, Kang YA, Yoon YS, Um SW, Lee SM, Yoo CG, Yim JJ (2006). The prevalence and evolution of anemia associated with tuberculosis. Journal of Korean medical science 21(6):1028-1032. |
|
|
Metanat M, Mashhadi MA, Alavi-Naini R, Rezaie-Kahkhaie L, Sepehri-Rad N, Afshari M (2019). The Prevalence of Absolute and Functional Iron Deficiency Anemia in New Cases of Smear-positive Pulmonary Tuberculosis and Their Sputum Conversion Rate at the End of Intensive Tuberculosis Treatment Phase. Prague medical report 121(1):35-41. |
|
|
Mukherjee A, Kaeley N, Dhar M, Kumar S, Bhushan B (2019). Prevalence, characteristics, and predictors of tuberculosis associated anemia. Journal of Family Medicine and Primary Care 8(7):2445. |
|
|
Oliveira MG, Delogo KN, Oliveira HM de MG de, Ruffino-Netto A, Kritski AL, Oliveira MM (2014). Anemia in hospitalized patients with pulmonary tuberculosis. Jornal Brasileiro de Pneumologia 40:403-410. |
|
|
Rapport (2019) Tuberculose |
|
|
WHO (2017). MOSCOW DECLARATION TO END TB 2017. |
|
|
WHO treatment guidelines for drug-resistant tuberculosis, 2016 update. n.d. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


