
ABSTRACT
Gynecologic lesions are largely ignored public health problems. The study seeks to establish the histologic pattern of gynecologic morbidities in Delta State. This is a descriptive retrospective study in Delta State University Teaching Hospital DELSUTH, Nigeria. The age and diagnosis of gynecological lesions diagnosed from 2014 to 2019 were extracted from the histopathology records, analyzed using Microsoft Excel 2007 Spreadsheet and summarized in tables. Gynecological lesions accounted for 16.4% of surgical biopsies. The age-groups of 20-29, 30-39, 40-49, 50-59 and 60-69 years accounted for 9.1, 36.3, 26.7, 15.4 and 7.1% of the cases respectively. Diseases of the myometrium, ovary, uterine cervix, endometrium, vagina, fallopian tube and vulva accounted for 42.6, 24.6, 19.5, 6.6, 1.9, 1.7 and 1.4% of the cases respectively. Benign neoplasms, malignant neoplasms, cystic non-neoplastic diseases, intraepithelial lesions, inflammatory and pregnancy-related disorders accounted for 53.3, 20.4, 9.3, 7.1, 6.0 and 2.8% of the cases respectively. Cervical lesions include cancer (59.2%), endocervical polyp (15.5%), intraepithelial neoplasm (15.5%), cervicitis (5.6%) and leiomyoma (4.2%). Myometrium lesions include leiomyoma (98.7%), adenomyoma (0.6%) and gangrenous uterus (0.6%). Endometritis (16.7%), hyperplasia (62.5%), and cancer (20.9%) occurred in the endometrium. Hydrosalpinx (6.3%), salpingitis (37.5%) and tubal pregnancy (56.3%) were the tubal lesions. Ovarian lesions included inflammatory disorders (11.6%), non-neoplastic cysts (34.9%), surface epithelial (24.2%), germ cell (18.6%) and sex cord stromal tumours (9.3%). Benign disorders are more common than malignancies with leiomyoma and cervical cancer representing the most common benign and malignant tumours respectively.
Key words: Gynecology, morbidity, cancer, females.
INTRODUCTION
While men and women have some common health challenges, some diseases are unique to women. These diseases are either related to pregnancy and childbirth; or to structural and functional disorders of the female reproductive organs (Zurayk et al., 1993). While the former has continued to receive adequate attention, and has been integrated into Primary Health Care since 1978 Alma-Ata declaration, the latter, which are referred to as gynecologic morbidities has been largely ignored in most developing countries (Declaration of Alma-Ata International Conference on Primary Health Care, Alma-Ata, USSR World Health Organization, 1978).
This may probably be due to lack of awareness of the burden of these morbidities.
Nevertheless, these gynecologic disorders account for a substantial portion of the workload in most histopathology centers (Wright et al., 2004). They are common cause of morbidity and mortality among women, and have negatively impacted on the quality of their lives with socioeconomic implication on the larger society (Anibue and Onyeka, 2014). In general, these gynecological disorders include infections, tumours and hormonally induced abnormalities of the female reproductive tract (Ellenson and Pirog, 2015).
Epidemiologic surveillance can be either community-based or hospital-based. While community-based approach is considered the gold-standard for research on gynecologic morbidities (Sadana, 2000), the convenience of engaging in hospital-based investigators is the main reason behind the choice of hospital-based studies despite its potential limitation.
Within these hospitals, correct diagnosis is the key to understanding the disease pattern, which is achieved through medical history evaluation, clinical examination, laboratory and radiological investigation. Of all these diagnostic modalities, histopathology evaluation remains the gold standard whenever post-operative specimens are available (Attunueci et al., 2004).
To the best knowledge, no earlier study has been done on this subject in Delta State, Nigeria. This paper therefore seeks to establish a novel database on the pattern of gynecologic morbidities in Delta State, using hospital-based histopathologic evaluation as the study tool. This will not only contribute to literature, but will also be of potential beneficial in policy advocacy, development and healthcare intervention.
PATIENTS AND METHOD
This descriptive retrospective study includes all gynecologic specimens that were received and examined in the department of histopathology of Delta State University Teaching Hospital (DELSUTH) from January 1st 2014 to October 31st 2019. Being one of the few centers that has the capacity to process and report histopathology specimens, it also serves as a referral center for other hospitals within and around the state. These specimens were received in 10% neutral buffered formalin solution, processed using automatic tissue processor, paraffin embedded, micotomed into 2-3µm thin sections and stained using haematoxylin and eosin stains. Special histologic stains were also applied where necessary and results interpreted with light microscope by the hospital pathologists. Information such as age and histologic diagnosis were extracted from the laboratory request forms and histopathology reports and analyzed using 2007 excel spread sheet. The results of these analyses were presented in Tables.
RESULTS
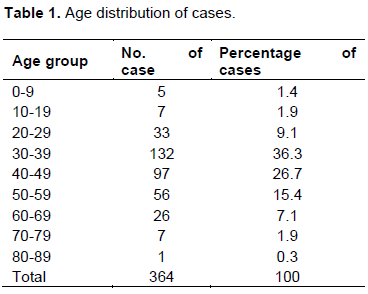
A total of 364 gynecologic specimens were included in the study, accounting for 16.4% of surgical specimens received in the department during the study period. The age range and mean age of the patients were 3-82 and 41.26 years respectively. The age-groups of 20-29, 30-39, 40-49, 50-59 and 60-69 years accounted for 9.1, 36.3, 26.7, 15.4 and 7.1% of the cases respectively. The details of the age distribution were depicted in Table 1.
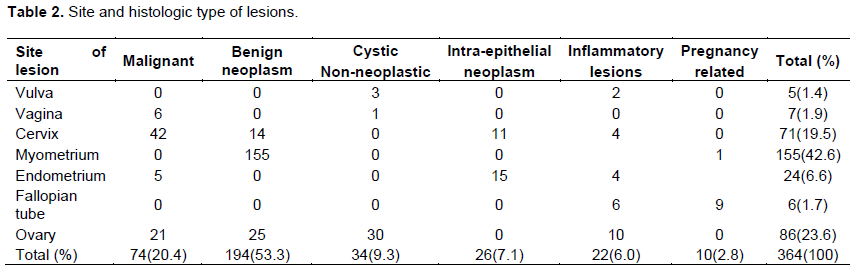
The regional distributions of the various histologic types of lesions encountered were shown in Table 2. Diseases of the myometrium, ovary, uterine cervix, endometrium, vagina, fallopian tube and vulva accounted for 42.6, 24.6, 19.5, 6.6, 1.9, 1.7 and 1.4% of the cases respectively. Benign neoplastic diseases, malignant neoplastic disease, cystic non-neoplastic diseases, intraepithelial lesions, inflammatory and early pregnancy-related disorders accounted for 53.3, 20.4, 9.3, 7.1, 6.0 and 2.8% of the cases respectively.
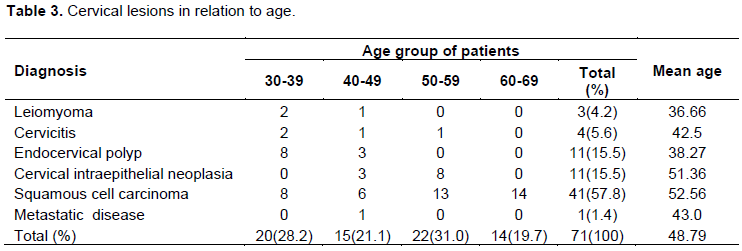
Age-wise distribution of lesions of the cervix was depicted in Table 3. Squamous cell carcinoma (SCC) and metastatic urothelial neoplasm were the cervical cancer encountered in this study, accounting for 57.8 and 1.4% of the diseases of the cervix. Other diseases include endocervical polyp (15.5%), cervical intraepithelial neoplasm (15.5%), cervicitis (5.6%) and cervical leiomyoma (4.2%). The corresponding peak decade for SCC and endocervical polyp was 50-59 and 30-39 years respectively.
Age distributions of diseases of the myometrium were shown in Table 4. Lesions encountered include leiomyoma (98.7%), adenomyoma (0.6%) and gangrenous uterus (0.6%). Cases in the 3rd, 4th, 5th and 6th decades were 7.1, 44.9, 35.3 and 10.3% respectively.

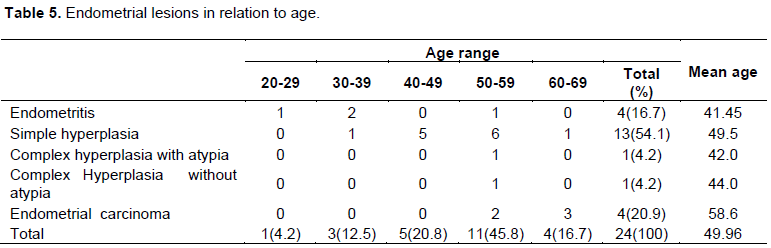
Age-wise distribution of lesions of the endometrium was depicted according in Table 5. Fifty-four-point one percent of endometrial lesions were simple hyperplasia without atypia, mostly within 40-59 years age group. Endometritis, complex hyperplasia, and endometrial cancers accounted for 16.7, 8.4 and 20.9% of the cases respectively.
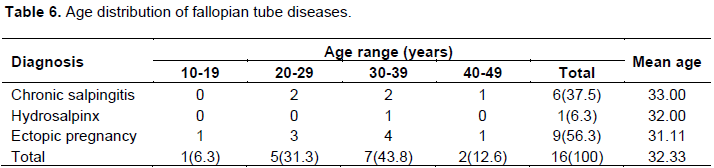
Lesions of the fallopian tube include hydrosalpinx (6.3%), chronic salpingitis (37.5%) and tubal pregnancy (56.3%). The mean age of patients with chronic salpingitis and ruptured tubal pregnancy were 33.0 and 31.1 years respectively. The details are shown in Table 6.
Ovarian disorders encountered in this study are depicted in Table 7. Inflammatory disorders, non-neoplastic cysts, surface epithelial tumours, germ cell tumours and sex cord stromal tumours accounted for 10 (11.6%), 30 (34.9%), 21 (24.4%),16 (18.6%) and 8(9.3%) cases respectively. The peak age group and mean age for patients with ovarian lesions were 30-39 years and 38.58 years respectively.
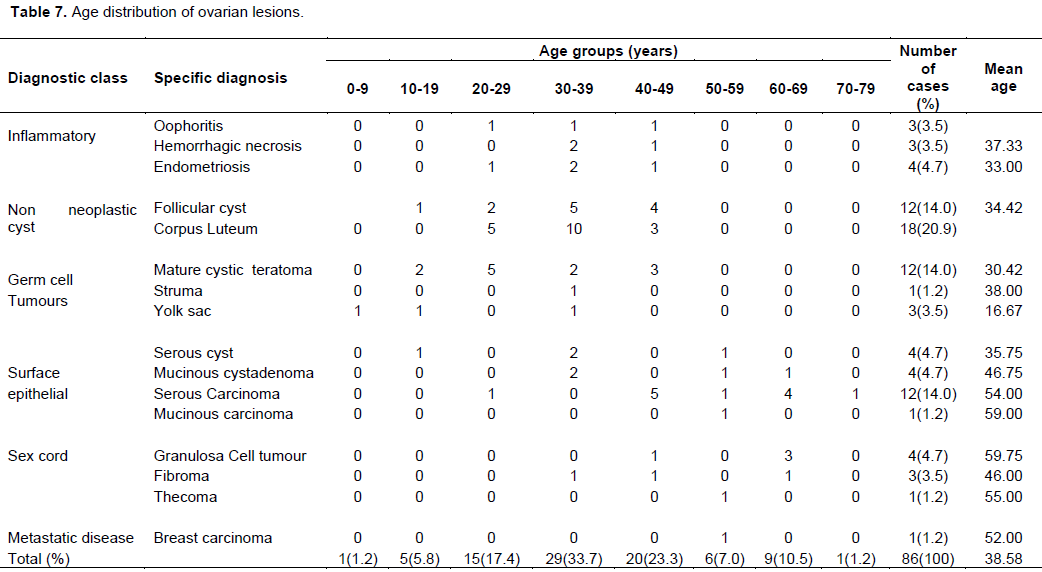
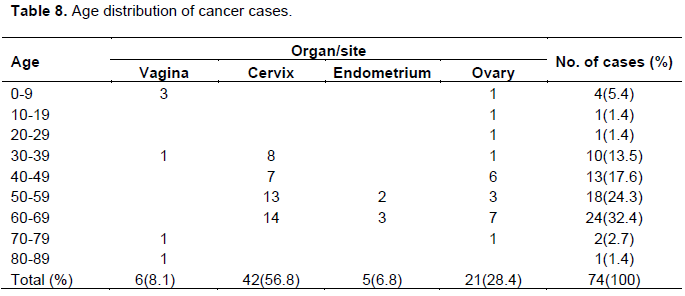
Table 8 shows the age distribution of gynecologic cancers. Cancer of the vagina, cervix, ovary, endometrium and ovary accounted for 8.1, 56.8, 6.8 and 28.4% of gynecologic cancers respectively. The peak age for cervical, endometrial and ovarian cancers were all in the 7th decade while most cases of vagina cancers occurred in the first decade.
DISCUSSION
There is currently no nation-wide report on the magnitude of gynecological morbidities that can be used for policy advocacy in Nigeria. Various researchers have attempted to analyze the burden of gynecologic morbidities in hospitals across the country, with considerable organ and age-specific heterogeneity (Keshinro et al., 2015; Ozumba et al., 2011).
The investigation showed that 16.4% of the surgical specimens were from gynecologic morbidities, which correlates with 14.9% reported in Lagos State, Nigeria (Keshinro et al., 2015). This is likely an under representation because besides the sample selection bias characteristic of facility based studies, the gynecologist may not need surgical biopsy to diagnosis or treat a number of infection and hormonally-induced diseases affecting the female genital tract. Such diseases would not be reflected in this analysis.
The age range, mean age and peak age group of patients with gynecologic morbidities in this study were 3-82 year, 41.58 years and the 4th decade respectively, all of which concur with result of analysis in Lagos (Keshinro et al., 2015). This age trend correlates with the structure of the present Nigerian population, consists predominantly of young population with a life expectancy of 54.5 years (Nigeria Population, 2019).
During the period under review, the most common indication for surgical procedures was benign diseases, representing 79.6% of the cases. This is lower than observation in Lagos (Keshinro et al., 2015) and Enugu (Ozumba et al., 2011) where such benign lesions accounted for 94.1 and 82.6% of all cases respectively. Vaginal lesions showed a marked deviation from the trend with a malignancy: benign ratio of 6:1. This is probably because primary lesions of the vagina are rare, with most of these cases being cancer cases (Ellenson and Pirog, 2015). In this study, Sarcoma botryoides accounted for 50% of the malignant tumours, while the rest of the cases were due to squamous cell carcinomas. Sarcoma butryoides is a variant of rhabdomyosarcoma with predilection for hollow viscus. This tumour is derived from embryonal smooth muscles, and accounts for 5% of all malignancies in children (Koukourakis et al., 2009). In this analysis, vaginal cancers are the 3rd most common gynecological cancer, accounting for 8.1% of all the cases. This is higher than reports from Sokoto, (Nnadi et al., 2014) Kano (Galadanci et al., 2003) and Port Harcourt (Seleye-Fubara et al., 2007) where it accounted for 0.25, 0.75 and 4.36% of gynecological malignancies respectively.
Lesions of the cervix accounted for 20% of gynecologic lesions. Cervicitis accounted for 5.6% of the cases. It is of the opinion that this is an underrepresentation of the magnitude of the problem because these cases are unlikely to be biopsied, as they would be treated with antibiotics. Hospitals offering lower level of care have capacity to manage infection-related disease and only refer more severe conditions such as cancers to tertiary care centers. The net effect is that patients with more severe diseases will present to tertiary care centers. Endocervical polyps accounted for 15.5% of the cases in this investigation with all cases within 30-49 years. The preponderance of this disease within the reproductive age has been demonstrated by other researchers (Keshinro et al., 2015; Ozumba et al., 2011).
Although entirely benign, the clinical significance of endocervical polyp is its tendency to provoke suspicion of more ominous disease (Ellenson and Pirog, 2015).
The uterine cervix was the most common site of female genital tract malignancy in this study. This correlates with 56.1% reported in Lagos (Keshinro et al., 2015) and 57.8% reported in Ghana (Nkyekyer, 2000). The author observation was higher than 48.6% reported in Kano, (Yakasai et al., 2013) but lower than 60.6, 63.1, 67.7 and 77% reported in Abakaliki (Agboeze et al., 2015) Port Harcourt, (Nwosu and Anya, 2004). Sokoto, (Nnadi et al., 2014) and Jos (Mandong and Ujah, 2003) respectively. In general, all Nigerian investigators agree that cervical cancer is the second most common gynecological cancer (Keshinro et al., 2015; Mandong and Ujah, 2003). The mean age of patients with cervical cancer in this study is 52.56 years which is probably because of the population structure in the area of study (Nigeria population, 2019). Cervical cancer is strongly associated with HPV infection and evolves through a pre-malignant phase (Ellenson and Pirog, 2015). Consequently, use of vaccines and cervical screening has greatly reduced its incidence in countries where nation-wide implementation of such preventive strategies were being carried out (Ellenson and Pirog, 2015). Across the globe, the incidence of cervical cancer has been on decline over the last 4 decades in developed countries, while 83% of new cases are encountered in developing countries (Parkin et al., 2005). There is therefore need for policy makers to ensure a community-driven cervical screening for cervical cancer and vaccination against oncogenic HPV to ensure reversal of this trend.
Uterine leiomyoma was the major lesion encountered in the myometrium and accounted for 43.5% the gynecologic lesions in this study. The observation is lower than the 50.5% reported in Lagos but higher than 25.9, 29.3 and 33.8% in Enugu, (Ozumba et al., 2011) Bayelsa (Ekine et al., 2015) and Imo state (Dike and Uzoma, 2017). The mean age of patients with uterine leiomyoma is 39.79 years which is in agreement with the general observation. Studies have also shown that leiomyomas are very common, and presents with more severe symptoms, for any age group among the nigros (Kjerulff et al., 1996). Though a benign lesion, uterine leiomyoma are associated with worrisome complications such as spontaneous abortion, fetal malpresentation, fetal growth restriction, uterine inertia, and postpartum hemorrhage (Ellenson and Pirog, 2015; Ouyang et al., 2006). This may be related to the cluster of most cases within the reproductive age, as is evident in most studies (Keshinro et al., 2015; Ozumba et al., 2011). A case of gangrenous uterus, a complication of septic abortion was reported in this investigation. Clandestine abortion with accompanied high morbidity and mortality is on the rise in the country (Bankole et al., 2015).
Endometrial hyperplasia was the most common endometrial lesions in this study, accounting for 79.2% of the cases. The dreaded complication of endometrial hyperplasia is the progression to adenocarcinoma in some cases (Ellenson and Pirog, 2015). Five cases of endometrial cancers were encountered in this study, representing 6.8% of gynecologic malignancies. This is however lower than 22% reported in Lagos; (Keshinro et al., 2015) but correlates with 5.6% and 6.5% reported in Kano (Yakasai et al., 2013) Jos (Mandong and Ujah, 2003) respectively.
Lesions of the fallopian tube encountered in this study consist mainly of tubal pregnancy and chronic salpingitis accounting for 56.3% and 37.5% of cases respectively. In real life situation, infections are the most common lesion in the fallopian tube, but are highly underrepresented among surgical specimens because a gynecologist will not do salpingectomy for chronic salpingitis except if there is no other option to salvage the tube. Several studies have also linked tubal pregnancy with pelvic infections (Doyle et al., 1991); further implying that there is high rate of tubal infections in this region.
Non-neoplastic ovarian cysts accounted for 34.9% of ovarian lesions encountered in this study. This correlates well with earlier studies that confirmed that non-neoplastic ovarian lesions are relatively common (Keshinro et al., 2015; Forae and Aligbe, 2014). Benign neoplasms accounted for 54.8% of gynecologic lesions. This is however lower than 82.6 and 83% reported in Enugu and Lagos respectively (Keshinro et al., 2015; Ozumba et al., 2011).
Ovarian cancer is the second most common gynecologic malignancy is this study, accounting for 28.4% of the cases. This rate is higher than 10, 14.6, 19 and 25.3% in Port Harcourt, (Nwosu and Anya, 2004) Lagos (Keshinro et al., 2015) Abakaliki (Agboeze et al., 2015) and Ghana, (Nkyekyer, 2000) but lower than 30.5% in Kano (Yakasai et al., 2013). Across the globe, the highest incidence of ovarian cancer is among Scandinavian countries, Isreal and North Amaerica (Ness et al., 2000).
CONCLUSION
Gynecologic lesions are often encountered in surgical pathology practice. Benign lesions are relatively more common than malignant cases. Uterine leiomyoma and cancer of the cervix are the most common benign and malignant gynecologic tumours. While this may be an underestimation of the problem, it will provide a reference baseline data for fellow researchers and policy makers on the morbidity of gynecological diseases.
LIMITATIONS OF THE STUDY
The study may not reflect the morbid trend of the study population because some patients may not attend to their health needs in this hospital and it is not all diseases that require surgical biopsy for diagnosis.
CONFLICT OF INTERESTS
The author has not declared any conflicts of interests.
REFERENCES
|
Agboeze J, Ezeonu PO, Onoh RC, Nwali MI, Agwu MR, Egbuji CC (2015). Frequency and Pattern of Gynecological Cancers in Federal Teaching Hospital, Abakaliki, Nigeria. Journal of Basic and Clinical Reproductive Sciences 4(2):54-57. |
|
|
Anibue UU, Onyeka TC (2014). Ethical, socioeconomic, and cultural considerations in gynecologic cancer care in developing countries. International Journal of Palliative Care 2014:1-6. |
|
|
Attunueci CA, Ball HG, Zweizig SL, Chen AH (2004). Differences in symptoms between patients with benign and malignant ovarian neoplasms. American Journal of Obstetrics and Gynecology 190:1435-1437. |
|
|
Bankole A, Adewole IF, Hussain R, Awolude O, Singh S, Akinyemi JO (2015). The Incidence of Abortion in Nigeria. International Perspectives on Sexual and Reproductive Health 41(4):170-181. |
|
|
Dike EE, Uzoma OI (2017). Histopathological Patterns of Gynecological Lesions at the Imo State University Teaching Hospital, Orlu, Nigeria: A 5 Year Review From 2009 - 2013. Imperial Journal of Interdisciplinary Research 4(3):1494-1497. |
|
|
Doyle MB, DeCherney AH, Diamond MP (1991). Epidemiology and etiology of ectopic pregnancy. Obstetrics and Gynecology Clinics of North America18(1):1-17. |
|
|
Ekine AA, Lawani LO, Iyoke CA, Ibrahim IA (2015). Review of the Clinical Presentation of Uterine Fibroid and the Effect of Therapeutic Intervention on Fertility. American Journal of Clinical Medicine Research 3(1):9-13. |
|
|
Ellenson LH, Pirog EC (2015). The Female Genital Tract. In. Kumar V, Abbas AK, Aster JC (Eds). Robins and Cotran Pathologic Basis of Disease 9th ed. Philadelphia: Elsevier pp. 992-1040. |
|
|
Ellenson LH, Pirog EC (2015). The Female Genital Tract. In: Kumar V, Abba AK, Aster JC (eds).Robins and Cotran Pathologic Basis of Diseases. Philadelphia: Saunders publishers pp. 1012-1013. |
|
|
Forae GD, Aligbe JU (2014). A histopathological overview of ovarian lesions in Benin City, Nigeria: How common are the functional cysts? International Journal of Medicine and Public Health 4(3):265-268. |
|
|
Galadanci HS, Mohammed AZ, Uzoho C, Jido TA, Ochicha O (2003). Gynecological malignancies in a tertiary health facility in Kano, Northern Nigeria. Tropical Journal of Obstetrics and Gynaecolology 20(2):105-108. |
|
|
Keshinro SO, Nwafor CC, Oshun P (2015). Histologic analysis of gynaecologic lesions in Nigerians. East African Medical Journal 92(5):245-253. |
|
|
Kjerulff KH, Langenberg P, Seidman JD, Stolley PD, Guzinski GM (1996). Uterine leiomyomas: Racial differences in severity, symptoms and age at diagnosis. Journal of Reproductive Medicine, Gynaecology and Obstetrics 41(7):483-490. |
|
|
Koukourakis GV, Kouloulias V, Zacharias G (2009). Embryonalrhabdomyosarcoma of the uterine cervix. Clinical and Translational Oncology 11(6):399-402. |
|
|
Mandong BM, Ujah AD (2003). Ten-year Review of Gynaecological Malignancies in Nigeria. Sahel Medical Journal 6(2):49-52. |
|
|
Ness RB, Grisso JA, Klapper J (2000). Racial differences in ovarian cancer risk. Journal of the National Medical Association 92:176-182. |
|
|
Nigeria Population (2019). Available at http://worldpopulationreview.com/countries/nigeria-population. |
|
|
Nkyekyer K (2000). Pattern of gynaecological cancers in Ghana. East African Medical Journal 77(10):534-538. |
|
|
Nnadi DC, Singh S, Ahmed Y, Siddique S, Bilal S (2014). Histopathological Features of Genital Tract Malignancies as Seen in a Tertiary Health Center in North-Western Nigeria: A 10-year Review. Annals of Medical and Health Science Research 4(3):213-217. |
|
|
Nwosu SO, Anya SE (2004). Malignancies of the female genital tract at the University of Port Harcourt Teaching Hospital: a ten year review - 1990-1999. Nigerian Postgraduate Medical Journal 11(2):107-109. |
|
|
Ouyang DW, Economy KE, Norwitz ER (2006). Obstetric complications of fibroids. Obstetrics and Gynecology Clinics of North America 33(1):153-169. |
|
|
Ozumba BC, Nzegwu MA, Anyikam A (2011). Histological patterns of gynaecological lesions in Enugu, Nigeria. A five-year review from January 1, 2000 to December 31st 2004. Advanced Biomedical Research 2(2):132-136. |
|
|
Parkin DM, Freddie B, Ferlay J, Paola P (2005). Global cancer statistics 2002. CA: A cancer Journal for Clinicians 55(2):74-108. https://acsjournals.onlinelibrary.wiley.com/journal/15424863 |
|
|
Sadana R (2000). Measuring reproductive health: review of community-based approaches to assessing morbidity. Bulletin of World Health Organization 78(5):640-654. |
|
|
Seleye-Fubara D, Uzoigwe SA, Akani CI (2007). Pathology of vaginal cancers in Port Harcourt, Nigeria. A 14-year study. Nigerian Journal of Clinical Practice 10(4):330-334. |
|
|
USSR World Health Organization (1978). Declaration of Alma-Ata International Conference on Primary Health Care, Alma-Ata, USSR. World Health Organization, 1978. |
|
|
Wright CT, Kurman JR, Ferenczy A (2004). In Wright CT, Kurman JR, Ferenczy A (Eds), Blaustein's pathology of the female genital tract 5th edition. New Delhi: Thomson press P 1203. |
|
|
Yakasai IA, Ugwa EA, Otubu J (2013). Gynaecological malignancies in |
|
|
Aminu Kano Teaching Hospital Kano: A 3 year review. Nigerian Journal of Clinical Practice 16(1):63-66. |
|
|
Zurayk H, Hind K, Nabil Y, Mawaheb El-M, Mohamed F (1993). Concepts and measures of reproductive morbidity. Health Transition Review 3(1):17-40. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


