Full Length Research Paper

ABSTRACT
Immunization is the most cost effective of public health intervention geared towards reducing childhood morbidity and mortality. There has been a global increase in the rate of immunization coverage with its attendant decline in vaccine preventable deaths. The immunization coverage in developing countries like Nigeria has however been challenging due to some reasons. Therefore, this study determined the immunization status and the factors affecting the vaccination status of under five children in Nasarawa State. Cross sectional descriptive studies of under five children in Nasarawa State using a multi staged sampling technique. Interviewer administered questionnaire was used for the recruited participants across the three senatorial zones of the state. Data collection was done using both the immunization cards and oral interview of care-givers. Data analysis was withanalyzed using the Statistical Package for Social Sciences (SPSS). Univariates, bivariates and multivariates analyses were done with significant value set at p < 0.05. A total of 55,036 of the target population of 74,775 (4% of the total population of Nasarawa State) received (Baccille, Calmette and Guerin BCG) vaccine in the state in the year 2018, giving a 73.6% immunization coverage for Nasarawa State in the year 2018. Immunization drop - out rate for pentavalent vaccine was 31.6%. The location of Primary Healthcare Centre, antenatal care attendance, distance to healthcare centre and numbers of children in a household are strong determinants of the immunization status across Nasarawa State. There is high immunization coverage in the present study. Incomplete immunization is influenced by Ignorance, mother’s travelling, fathers’ refusal, child’s small stature and or illness as well as distance to the health facilities.
Key words: Coverage, determinants, immunization, status, under five.
INTRODUCTION
Immunization coverage is the proportion of a given population that has been immunized in a particular time (Adebayo et al., 2012)). It is developed and targeted at the prevention of infectious diseases among children as well as other vulnerable member of the society (Ophori et al., 2014). Immunization is the most cost effective public health intervention geared towards reducing childhood morbidity and mortality (Abdou et al., 2017; Mallika et al., 2014). There has been global increase in the rate of immunization coverage with its attendant decline in vaccine preventable deaths (Awoh and Plugge, 2016). The immunization coverage in developing countries like Nigeria, has however being challenging for many reasons. It varies from place to place even within the same locality (Phadnis et al., 2015). It is an essential component of Primary Health Care (PHC) and involves routine immunization which is often provided across all tiers of Government (be it public or private) but mostly at the public PHC’s (Jamo, 2017).
According to the National Program on Immunization (NPI), routine immunization includes; Baccille Calmette and Guerin (BCG) give at birth, Oral Polio Vaccine (OPV) giving at birth, 6, 10 and 14 weeks. Also, Hepatitis B vaccine at birth, Pentavalent (Diphtheria, Pertussis, Tetanus, Hepatitis B and Haemophilus Influenza type B) vaccine at 6, 10 and 14 weeks. While Yellow fever and Measles vaccine are given at 9 months (Ophori et al,. 2014). The need to improving immunization status as well as ensuring that it is timely done has been earlier alluded to (Sood et al., 2015). Reasons for low and delay immunization coverage range from cultural, religious, socio-economic status, place of residence and issues relating to health facility (Ophori et al., 2014; Jamo, 2017; Illias et al., 2018). A study by Meleko et al. (2017) in Ethiopia among under five children revealed 42.2, 49.4 and 8.4% were fully immunized, partially immunized and not immunized at all respectively. Similarly, an urban slum study in India found 64.8, 31.5 and 3.7% fully immunized, partially immunized and not immunized at all respectively. A similar finding was reported from Sudan, with more urban than rural dwellers completing immunization (Tibin et al., 2014). Also, Sanou et al. (2009) in Burkina Faso reported 50.2% total immunization coverage while a drop-out rate of 2.1% was reported in another study (Tibin et al., 2014). A study in Senegal reported that 72.3% of their respondents had immunization within the recommended time schedule (Abdou et al., 2017).
There is dearth of evidence from Nasarawa State on the level of immunization coverage. The National Primary Health Care Development Agency (NPHCDA) in conjunction with other partners carried out a population survey on immunization coverage across nine Northern states (excluding Nasarawa State) and reported a low coverage of < 50% (Gunnala et al., 2016). This abysmally low coverage prompted this study which was therefore set out to address these knowledge gap through determineing the immunization status ofamong under five children under five and to evaluate the factors affectingssociated with the vaccinationimmunization status of the under five children in Nasarawa State Nigeria.
MATERIALS AND METHODS
Study design
This was a cross sectional descriptive study. An interviewer administered questionnaire was used and variables such as place of delivery, mother’s marital status, parent socio-economic status, numbers of children in the household, immunization status and reasons for non-vaccination and or incomplete immunization etc. They were also told to present their immunization cards for sighting and cross checking (if available) as evidence of vaccination.
Study site
The study was conducted at the immunization units of the selected Primary Health Care (PHC). The immunization units are manned by either Junior Community Health Extension Workers, Community Health Extension workers or Community Health Officers trained on vaccination. There are 760 public PHCs in Nasarawa State.
Nasarawa State is one of the States created in October 1st 1996 by the Late General Sani Abacha. The state is one of the six North Central States. It has boundaries with the Federal Capital Territory (FCT) Abuja in the West, Kaduna State in the North, Plateau and Taraba States in the East, Benue and Kogi States in the South. The State is made up of thirteen Local Government Areas (LGA) and eighteen Development Areas (DA).
Its capital is in Lafia, the state has a landmass of 27,117km2 (10,470 sq m). The state’s total population according to the 2006 National Population Census was 1,869,377. The target population is 74,775 (4% of the total population of Nasarawa State). The immunization coverage for Nasrawa State in the year 2018 is the numbers of children immunized in 2018 divided by the target population and multiply by a hundred. Immunization drop – out rate is the number of children that received Penta1 minus the number of children that received Penta3 divided by the number of children that had Penta1 multiply by a hundred.
Nasarawa State’s mainstay of economy is Agriculture and has some mineral resources such as salt. It is known as the State of solid minerals. The State has a Federal University, Nasarawa State Polytechnic, a College of Agriculture and a School of Nursing all in Lafia. It has Federal Polytechnic in Nasarawa, Nasarawa State University in Keffi and College of Education at Akwanga. The State has diverse ethnicity with some of the major tribes being Alago, Eggon, Mada, Kanuri, Hausa-Fulani, Koro (Migili), Gwandara, Afo, Ebira e.t.c. There are three Senatorial Zones namely; Nasarawa West, Nasarawa North and Nasarawa South respectively.
Study population
The study was targeted and done among children under – five years of age across Nasarawa State Nigeria. The target population is 74,775 (4% of the total population of Nasarawa State). The immunization coverage for Nasarawa State in the year 2018 is calculated as the number of immunized children (55,036) divided by the target population (74,775) multiply by 100. Immunization drop – out rate is calculated as the number of children that had Penta1 minus the number of children that had Penta3 divided by the number of children that had Penta1 multiply by hundred, which is  x 100.
x 100.
Sample size
The minimum sample size calculated using the Yamane formula 
n is the minimum calculated sample size, N is the population size (74,775 at 4% of the state population), e is the margin of error / precision (0.05).


n of 398 represent the minimum sample size that is acceptable for a study result to be statistically significant. The higher the sample size the better reliable the result and its conclusions. A total of 550 participants were therefore recruited for this study.
Sampling technique
A multi stage sampling technique was used. The State was divided into the three Senatorial Zones. Nasarawa West, North and South senatorial zones are made up of five, three and five Local Government Areas respectively. The population of Nasarawa West is 716,802, Nasarawa North is 335, 453 and Nasarawa South is 811,020 respectively. In view of this disparity in population and LGA, both the Western and Southern senatorial zones which are at least twice the size of the Northern senatorial zone, have health facilities selected according sampling proportionate to size in ratio 2:1:2.
With the list of PHC per senatorial zone gotten from the Nasarawa State Primary Health Care Development Agency (NPHCDA), the PHC’s will be arranged alphabetically. The LGAs in each senatorial zone were categorized into urban and rural, same for the PHCs in the LGAs. Two urban PHCs and two rural PHCs each were selected from Nasarawa South and Western senatorial zones while one urban and one rural PHC was selected from the Nasarawa North senatorial zone. Hence, a total of ten PHCs were recruited with four each from the Western and Southern Zones, while two were selected from the Northern senatorial zone. The PHC’s were selected using simple random sampling.
At least fifty five children were selected from each of the selected PHCs using a convenient sampling technique. They were recruited as they present for immunization. Interviewer administered questionnaire was used to derive information such as their biodata and other information relevant to immunization as well as its timing. Their immunization cards were also reviewed if available and if not, the mothers or care – givers words were taken. Secondary data of the 2018 register of immunization were used to retrieve variables such as age, gender, and numbers of those that receive each vaccine antigen per Local Government Areas across the state.
Inclusion criteria
1) All children less than five years old whose mother presented to the health facility either for the child’s or siblings immunization, for family planning or for visitation.
2) All children within the age bracket within the community whose parents gave consent.
Data analysis
The data variables were coded and entered into an excel spreadsheet before exporting to Statistical Package for Social Sciences (SPSS) version 20. Categorical variables were summarized with frequency and percentages. Association between two categorical variables was determined using chi square test. Correlation and regression analysis were done to assess factors responsible for immunization coverage. Significant level was set at p < 0.05.
Ethical consideration and confidentiality
Ethical approval was sought and obtained from the State Research Ethics Committee. Approval to conduct the research was obtained from the Nasarawa State Primary Health Care Development. Following this, immunization status and determinants of immunization coverage in Nasarawa State was obtained.
Confidentiality of patient identity and other information was strictly adhered to. Codes were used rather than names. The results based on locality isresults based on locality are only known to the researchers as de-identifiers were employed. Thus, there are no riskis no risk to the participants.
RESULTS
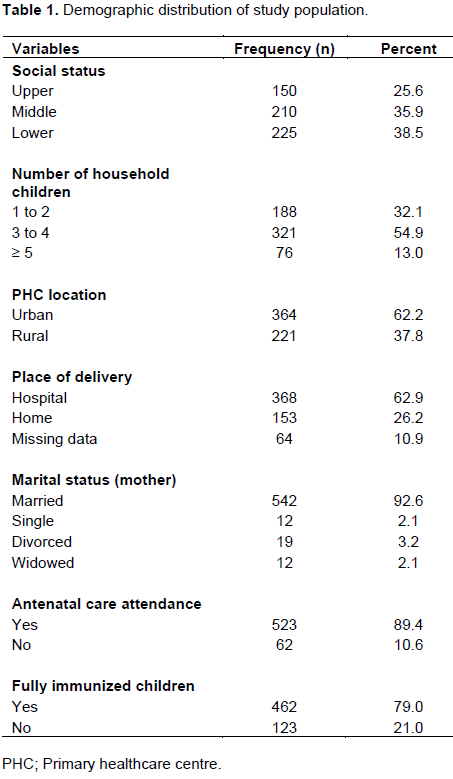
Of the 585 subjects recruited for this study, males were 295 (50.4%) while females were 290 (49.6%) with a male to female ratio of 1:1. Approximately three quarter of the study population was from either the middle or lower socio-economic class. One fourth of the respondent delivered at home with the traditional birth attendants, with the antenatal attendance outweighing hospital supervised deliveries. This implies that many women attend antenatal services in the Hospital but had their deliveries at home with the traditional births attendants. Seventy nine percent of these study population were fully immunized (Table 1).
A total of 55,036 infants received (Baccille, Calmette and Guerin BCG) vaccine in the state in the year 2018. The target population is 74,775 (4% of the total population of Nasarawa State). The immunization coverage for Nasarawa State in the year 2018 is 73.6%. Immunization drop – out rate for pentavalent vaccine was 31.6%.
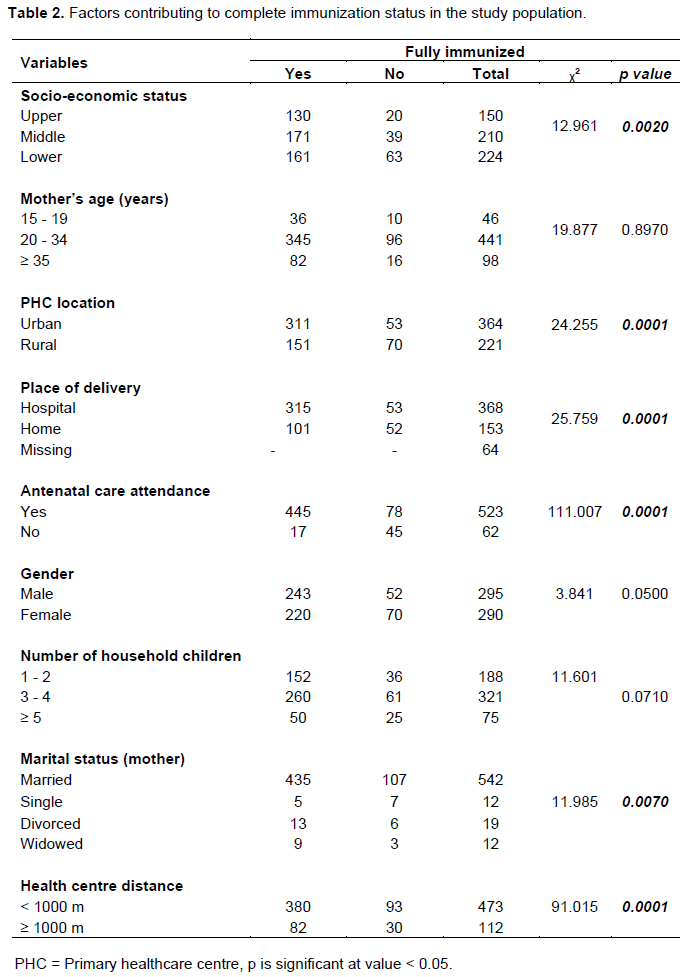
Factors contributing to complete Immunization status in the study population
Socio-economic status, primary healthcare centre location, place of delivery, antenatal care attendance, marital status and healthcare centre distance are all statistically significant factors to achieving complete immunization (Table 22).
Correlation between immunization status and some contributing factors
There is a significant positive correlation between the location of primary healthcare centre, antenatal care attendance, socio-economic status, distance of healthcare centre and number of children in a household as shown in Table 33.

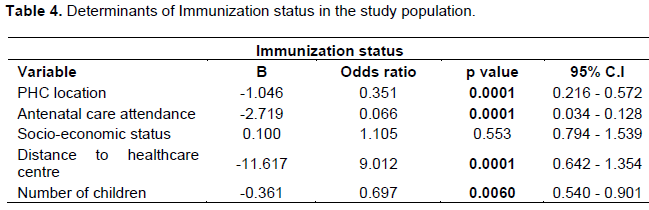
Determinants of immunization status in the study population
Using a multinomial logistic regression analysis showed that location of PHC, antenatal care attendance, distance to healthcare centres and numbers of children in a household wereare strong determinants of the immunization status of Nasarawa State under five children (Table 44).
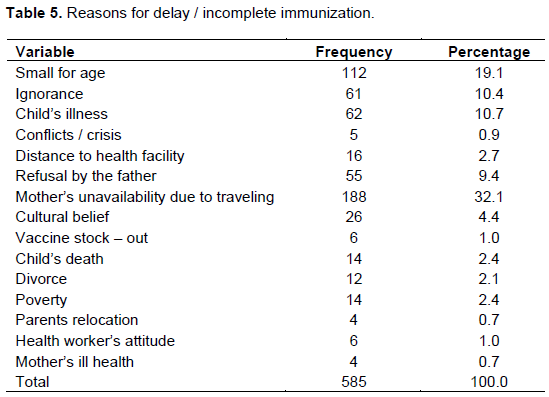
Reasons for delay / incomplete immunization
The mother’s unavailability due to traveling (mostly for social reasons of visitation, felicitation and condolences with families and friends), perceived child’s small size (some mothers believed that a newborn irrespective of gestational age, is too tiny / young for multiple injections in whatever guise), the fathers refusal, child’s ill health (when a child became febrile, crying excessively or throwing up after receiving a dose of vaccine [common with pentavalent], and the mothers are usually told not to give any medication), ignorance and cultural beliefs / myths were among the major reasons for the delay or incomplete immunization (Table 5).
DISCUSSION
Approximately three – quarter of this study population were from either the middle or lower socio-economic class. More than 90% of the mothers in this study are married.
In the current study, the proportion of under – five children that are fully immunized(is 79%). This is comparable to the WHO norm of 80%. It is higher than the 42.2% reported by Meleko et al. (2017) in south west Ethiopia. This is also greater than the 64.8% found by Phadnis et al. (2015) in Karnataka India. The observed difference with the present study may be due to the intense efforts being put in place by the Governments and partners such as Rotary international, United Nation Children Emergency Fund (UNICEF) etc to strengthening routine immunization and supplementary immunization activities. The higher sample size used in the current study may make it more précised compared with the Ethiopia and India studies above.
The proportion of fully immunized children in the current study is higher than the abysmally lower; less than 10% obtained in some Northern States by Abdulkarim et al. (2011) in 2011. The high (three quarter) of this study population having children between 1 to 4, mostly residing in urban areas and having a higher to mid socio-economic status which implies a probably better education, enlightened citizens with improved purchasing power. All these, might explain the improved immunization status noticed. The observed improvement may have in part resulted from renewed commitment in recent years by the Nigerian Government and her partners towards improving childhood immunization. Additionally, Nasarawa State has been largely peaceful without interruption of social services unlike some Northern States (especially the North-Eastern States) that has witnessed several insurgency attacks in recent years. The difference may also be temporal (almost ten years apart) and geo-graphical (core North (North West and East) compared with the current study here in Nasarawa State which is in North Central Nigeria and with close proximity to the Federal Capital Territory FCT). These may have improved the delivery of vaccines to eligible children resulting in the observed marked improvement.
The proportion of fully immunized children was highest among the upper socio-economic class and this is consistent with earlier reports (Jamo, 2017;Bello, 2014).Perhaps, the higher educational status could have aided the understanding of the benefits of immunization and hence drive their demand for it. Also, delivery in the hospital and antenatal attendance were associated with full immunization status. This is in consonant with other reports and it is plausible that mothers had received vital information about the benefits of immunization during their interaction with the health facilities which may have impacted positively on the uptake of immunization. Furthermore, children were more likely to be fully immunized if the designated primary health care centre is closer and is located in the urban area. Basic social amenities such as road networks and educational facilities are often lacking in most rural communities, perhaps poor accessibility of health centers in the rural communities as well as poor awareness may have been responsible for the poor immunization status of children in the rural communities. This is similar to the findings in some selected Local Government Areas in North-western Nigeria (Jamo, 2017;Bello, 2014).
The immunization coverage of 73.6% from this study is higher than the 50.2% reported by Sanou et al. (2009) in Burkina Faso. A high drop – out rate of 31.6% found in this study is however, higher than the 20.5% reported in a study in Ethiopia. Tessema Higher than the 1% reported by Chinawa in Enugu South East Nigeria. Chinawa The finding in the current study is lower than the report from other Northern States of Yobe, Jigawa, Kano, Zamfara and Katsina with more than 50% rates (Ophori et al., 2014). The reason for this unacceptably high attrition may not be unconnected with the various reasons given for either delay or incomplete immunization which includes; Ignorance, Travelling by the mother, Father’s refusal, child’s ill health, the assumption that some children are too small for multiple injections as well as cultural beliefs.
CONCLUSION
1) The immunization coverage in this study is 73.6%.
2) There is a significant relationship between immunization status and socio-economic status, antenatal attendance, number of children in a household, location and distance to health facilities.
3) Incomplete immunization is influenced by Ignorance; mother’s travelling for social reasons, fathers’ refusal, child’s perceived small stature and or illness after receiving a dose of a multi-dose vaccine as well as distance to the health facilities.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The following people were acknowledged for their contributions and assistance towards getting the study done; Pharmacist Sunday Iliya (the Nasarawa State Immunization officer), the immunization officers at PHC Keffi, Kokona, Akwanga, Lafia and Obi Local Government Areas and Miss Francisca Uba who assisted in administering questionnaires.
REFERENCES
|
Abdou M, Mbengue S, Mboup A (2017). Vaccination coverage and immunization timeliness among children aged 12-23 months in Senegal?: a Kaplan-Meier and Cox regression analysis approach. Pan African Medical Journal 27(4):1-7. |
|
|
Abdulkarim A, Ibrahim R, Fawi A, Adebayo OA, Johnson A'WBR (2011). Vaccines and immunization?: The past, present and future in Nigeria. Nigerian Journal of Paediatrics 38(4):186-194. |
|
|
Adebayo BE, Oladokun RE, Akinbami FO (2012). Immunization coverage in a rural community in Southwestern Nigeria. Journal of Vaccines and Vaccination 3(4):1-3. |
|
|
Awoh AB, Plugge E (2016). Immunisation coverage in rural - urban migrant children in low and middle-income countries (LMIC): a systematic review and meta-analysis. Journal of Epidemiology and Community Health 70(4):305-311. |
|
|
Bello A (2014). Health Personnel and the Successes of Immunization in Nigeria?: A study of selected Local Governments Areas of Kaduna State. Review of Public Administration and Management, 2(6):10-20. |
|
|
Gunnala R, Ogbuanu IU, Adegoke OJ (2016). Routine Vaccination Coverage in Northern Nigeria?: Results from 40 District-Level Cluster Surveys. PLoS One 11(3):14-27. |
|
|
Illias KS, Firoz S, Kurlikar PR (2018). Status and determinants of child immunisation coverage in three South Asian countries, India, Bangladesh and Nepal: Evidence from the Demographic and Health Survey. Sri Lanka Journal of Child Health 47(13):56-63. |
|
|
Jamo IA (2017). Socio-cultural factors and the Successes of Immunization in selected Local Governments areas of Kaduna State, Nigeria. Journal of Research in National Development 15(1):8-15. |
|
|
Mallika CV, Siva S, Ranga MK (2014). A Survey on Immunization Coverage among Children of rural South Kerala. Journal of Evolutionary Medicine and Dentistry Science 3(2):9113-9123. |
|
|
Meleko A, Geremew M, Birhanu F (2017). Assessment of Child Immunization Coverage and Associated Factors with Full Vaccination among Children Aged 12 - 23 Months at Mizan Aman Town, Bench Maji Zone, Southwest Ethiopia. International Journal of Pediatrics 3(1):1-12. |
|
|
Ophori EA, Tula MY, Azih AV, Okojie R, Ikpo PE (2014). Current Trends of Immunization in Nigeria?: Prospect and Challenges. Tropical Medical Health 42(3):67-77. |
|
|
Phadnis S, Khadka S, Pattanshetty S (2015). Assessment of immunization coverage among under-five year old children residing in slum settlements in an urban area in coastal Karnataka. Global Journal of Medicine and Public Health 4(2):1-7. |
|
|
Sanou A, Simboro S, Kouyaté B (2009). Assessment of factors associated with complete immunization coverage in children aged 12-23 months?: a cross-sectional study in Nouna district, Burkina Faso. BMC International Health and Human Rights 9(4):1-15. |
|
|
Sood RK, Sood A, Bharti OK (2015). High Immunization Coverage but Delayed Immunization Reflects Gaps in Health Management Information System (HMIS) in District Kangra, Himachal Pradesh, India - An Immunization Evaluation. World Journal of Vaccine 5(3):69-78. |
|
|
Tibin IA, El-tayeb EM, Omer FA (2014). Assessment of Routine Immunization Coverage in Nyala Locality, Reasons behind Incomplete Immunization in South Darfur State, Sudan. Asian Journal of Medical Science 6(2):1-8. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


