ABSTRACT
Patients undergo nutritional therapy so as to prevent malnutrition or worsening of the condition. When they are unable to receive oral nutrition, the most common form of physiological and nutritional therapy is through enteral nutrition (EN). The drug-nutrient interaction is described as occurring changes in the kinetics or dynamics of the drug or nutrient administered. The purpose of this study is to describe drug-nutrient interactions in prescriptions required for enteral nutrition in patients at the Intensive Care Unit of a General Hospital of the Federal District. A descriptive-exploratory study was undertaken with data collected from January 2011 to December 2012 at the Intensive Care Unit (ICU) of the North Wing Regional Hospital (Hospital Regional da Asa Norte – HRAN). The investigation for interactions in prescriptions was conducted using Micromedex ® software and Spearman correlation was used for the statistical analysis of variables. In the 101 prescriptions analyzed, 1190 drugs were found. The minimum amount of drugs found per patient was 7 and the maximum was 18, at an average of 12 drugs. Regarding enteral drug-nutrition interaction, the incidence was 15.94%, while drug-drug interaction occurred in 84.06% of all observed interactions. The most frequent interactions were moderate, in 44.57% of the incidences, followed by major interactions at 32.33%, and minor interactions at 13.16%, and lastly the contraindications in 9.93% of prescriptions analyzed. There was a high incidence of moderate degree drug interactions in patients under enteral nutrition therapy.
Key words: Enteral nutrition, drug-drug interactions, drug-nutrient interaction.
Patients in Intensive Care Units (ICU) are more likely to evolve in drug interactions and drug-nutrient interaction due to the high number of different medications prescribed concomitantly. These interactions take place when pharmacological effects increase to toxic levels, hence altering the benefits of drug therapy prescribed to the patient. Chances of interactions increase in elderly patients if associated with risk factors such as surgical procedures with concurrent use of drugs (polypharmacy), severity of illness and organ failure (Carvalho et al., 2013; Santos et al., 2011; Varallo et al., 2013; Lima and Cassiani, 2009). As part of treatment, patients undergo nutritional therapy to avoid malnutrition onset. When patients are unable to receive oral nutrition, the most common and physiological route for nutritional therapy is enteral nutrition (EN), characterized by diet administration through tube or ostomy, depending on delivery to the appropriate position in the gastrointestinal tract. However, through the same feeding tube, drugs are administered which may bring about interactions altering nutritional and pharmacological factors, thereby jeopardizing the expected results of treatment and prognosis in ICU patients (Lopes et al., 2010; Silva et al., 2010; Zaban and Novaes, 2009).
The drug-nutrient interaction is described as occurring changes in kinetics or dynamics in the administration of a drug or nutrient. Possible consequences of these interactions are formation of other substances, reduced bioavailability of drug into the circulation, and impaired absorption of nutrients through changes that may occur in the intestinal mucosa. Such results lead to malnutrition, extend time and hospitalization costs, pose damage to the patient's health, therefore increasing the amount of drugs used for the treatment of chronic characteristics (Lopes et al., 2010; Silva et al., 2010).
As the changes occur, there may be interference with the proposed therapy to the patient, since many drugs have pharmaceutical forms that are gradually released into the body or drugs that disintegrate and metabolize in different positions in the digestive system. Some drugs can alter nutrient uptake, even inhibiting the metabolic process of the latter. Therefore, interactions may arise in the administration of food along with medicine during digestion, distribution or elimination of drugs (Zaban and Novaes, 2009; do Ouro Reis et al., 2010; Heldt and Loss, 2013).
The purpose of this study was to describe interactions between drugs and nutrients in enteral nutrition required for patients at the Intensive Care Unit of a General Hospital of the Federal District.
An exploratory descriptive study, with data collected from January 2011 to December 2012, was conducted at the IUC of the North Wing Regional Hospital (Hospital Regional da Asa Norte, HRAN), a general, school hospital in the Federal District. The sample consisted of patients in critical conditions from the ICU showing imbalance of one or more organic systems due to surgeries, infections or other conditions that require intensive support. As inclusion criteria, we considered patients older than 15 years hospitalized for more than 24 hours, undergoing enteral nutrition therapy. As exclusion criteria we considered those who were hospitalized for less than 24 hours or not undergoing enteral nutrition therapy.
The research project was approved by the Research Ethics Committee from the Health Sciences Teaching and Research Foundation (Fundação de Ensino e Pesquisa em Ciências da Saúde), of the State Health Department in Brasilia, Federal District (CEP/FEPECS) under protocol 462/2011. Data were collected from medical records authorized by the director of the hospital and the head of the unit upon signing the authorization recommended by Resolution 196/96 for research involving humans.
Each patient had only one prescription analyzed, chosen from between the second to before the last day of hospitalization. Data were collected on patient records after leaving the ICU due to discharge, transfer or death. The following variables were analyzed: socio-demographic aspect (age, origin); primary and secondary diagnoses; dosage of drugs prescribed concomitantly with enteral nutrition; standard and non-standard drugs listed at the State Health Department of the Federal District (Secretaria de Estado de Saúde do Distrito Federal, SES/DF), approved (or not) by the National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária, ANVISA), indication, composition, venous access, duration and complications of enteral nutrition (clinical, metabolic, infectious and mechanical), time of patient stay at the ICU, prognosis, clinical outcomes, presence of other reactions that may be related to possible drug and/or nutrient interactions causing any changes in the prescription of nutritional or drug therapy.
The search for interactions in prescriptions was obtained using the Micromedex ® (Thomson Reuters 2011) software. Interactions were classified according to degree of severity: contraindicated, high-grade, moderate grade and low grade. High degree interactions are those which threaten the patient's life and/or require medical intervention to minimize or prevent serious adverse effects. Moderate interactions can aggravate the patient's condition and/or require changes in therapy. Low degree interactions have limited effects whose manifestations may include increase in frequency or severity of adverse effects that usually do not require changes in the pharmacotherapy. Contraindication is when concomitant administration of drugs should be avoided or performed according to the World Health Organization (WHO).
The Spearman correlation was used for statistical analysis and the results were analyzed using Statistical Analysis Software (SAS) version 9.3 and Microsoft Excel 2010.
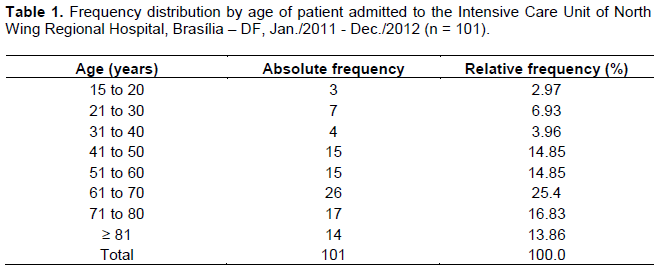
The frequency distribution of the 101 patients who received enteral nutrition grouped according to age is shown in Table 1. The age group with the greatest number of patients was 61 to 70 years old (25.74%). Observation noted that ages were concentrated between 41 to 80 years old, of which the cumulative frequency was 72.28%. Regarding age, a 78 year span (15 minimum and 93 maximum) and a mean age of 60 years old was observed. In the 1st quartile, results showed that in 25% of younger patients, age ranges up to 48 years; as for the median age, 50% of patients, age ranges up to 63 years old; finally, in the 3rd quartile 75% of patients, age ranges up to 74 years.
The distribution of patients according to gender was well balanced, with a difference of only 1%. Among the 101 patients, 51 (50.50%) were male and 50 (49.50%) were female. Most of the patients investigated (70 or 69.31%) died, while 29 (28.71%) were discharged from the ICU and only 2 (1.98%) were transferred to another unit.
The highest hospitalization frequency was: 0 to 15 days with 50 (49.50%) patients, 16 to 30 days with 17 (16.83%) patients, 31 to 45 days with 10 (9.90%), 46 to 60 days with 8 (7.92%) and a total of 16 (15.84%) who stayed longer than 61 days. Observation also showed that the time range for the highest hospitalization frequency spanned between 6 and 10 days (18.81%), followed by 11 and 15 days (17.82%). The minimum and maximum hospital stay was 2 and 153 days, respectively, with a total average of approximately 31 days. In the 1st quartile, 25% of these patients remained hospitalized for about 8 days; with the median, 50% of these patients stayed up to 16 days at the IUC. And finally, the 3rd quartile shows that 75% remained up to 43 days in hospital.
The administration of enteral nutrition was made by probes which differ according to the position in which they are located. A gastrostomy (GTT), which is based on a probe inserted directly into the stomach through an abdominal port, was found in 2 (1.98%) patients; a nasoenteral tube (NE) which is inserted nasally or orally (in specific cases) in a post pyloric location, was present in 87 (86.14%) cases; and, finally, the nasogastric (NG), which is also inserted nasally or orally located in the stomach, was used in 12 patients (11.88%) patients.
For admissions in ICUs of the Federal District, physicians needed to register the patient requiring a ICU bed at the Hospital Bed Regulation Center in accordance with Ordinance 41 SES/DF dated August 30, 2006 which regulates hospital beds in establishments linked to the Health Care System of the Federal District (Sistema Único de Saúde [SUS], 2010). Patients admitted came from: 52(51.49%) from other units of the same hospital; 46 (45.54%) from other public hospitals in the Federal District; 2 (1.98%) from private hospitals; and 1 (0.99%) from hospitals outside the Federal District.
Enteral nutrition as therapeutic indication for all 101 patients was caused by the need for energy intake and inability to swallow. All drugs used were listed by the SES/DF and accredited at the National Health Surveillance Agency (ANVISA). Concerning the clinical condition of patients undergoing enteral nutrition, 63 (62.38%) were hemodynamically stable, 21 (20.79%) were anuric, 20 (19.80%) were on hemodialysis and 1 (0.99%) developed acute pulmonary edema.
Severe hydro-electrolyte or metabolic disorders were found in 35 (34.65%) patients. Of the metabolic disorders identified, the most frequent were: hyperkalemia in 11 (12%) patients, hypernatremia in 7 (8%), hypokalemia in 7 (8%) and metabolic acidosis in 5 (6%) patients. Other metabolic or electrolyte disorders showed relative frequency (%) equal to or less than 4%. Different types of disorders such as secretion drainage for bleeding or bruising were found in only 7 cases.
Concomitantly, other complications, which could be related to the use of enteral nutrition or medications, were also recorded. Local, systemic or secondary infection due to the use of central venous access was observed in only 16 (15.84%) patients. No patient had significant hydro-electrolyte loss, hypertriglyceridemia, hepatic steatosis or cholestasis. Changes in the capillary glucose of the hyperglycemia type were found in 32 (32%) patients, hypoglycemia in 5 (5%), changes of the two types in 9 (9%) and 55 (54%) showed no change in capillary glucose.
Other complications related to the use of enteral nutrition were registered as gastric residue in 24 (24%), constipation in 24 (24%), at least one episode of diarrhea in 14 (14%), abdominal distension 9 (9%) and vomiting in 5 (5%) patients.The minimum and maximum number of medical diagnosis per patient was 1 and 9, respectively, with an average of 5. In the 1st quartile, 25% of patients had up to 4 diagnoses; in the median, 50% had up to 5 diagnoses; finally, in the 3rd quartile, 75% had up to 6 diagnoses.
With respect to the amount of drugs used by these patients, 44 (43.56%) received 10 to 12 different drugs, followed by 32 (31.68%) who received 13 to 15 drugs, 18 (17.82%) received 7 to 9 drugs, and the group that received the greatest number of drugs, 16 to 18, consisted of 7 (6.93%) patients.
The minimum and maximum amount of drugs per patient was 7 and 18, respectively, with an average of 12. In the 1st quartile, 25% of patients received up to 10 drugs; in the median, 50% of received up to 12 drugs; finally, in the 3rd quartile, 75% received up to 14 drugs.
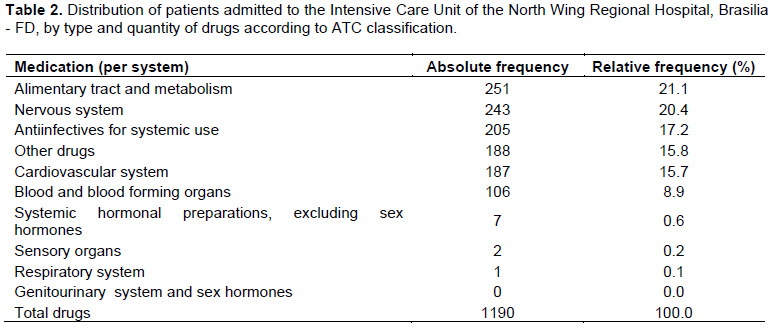
All patients fell within the concept of polypharmacy (five or more medications). The amount of drugs found in the prescription was classified according to Anatomical Therapeutic Chemical (ATC) (Cardinal et al., 2012), the international standard for studies on drug use. The ATC is divided into different groups according to the organ or system in which they act and their chemical, pharmacological and therapeutic properties (Table 2).
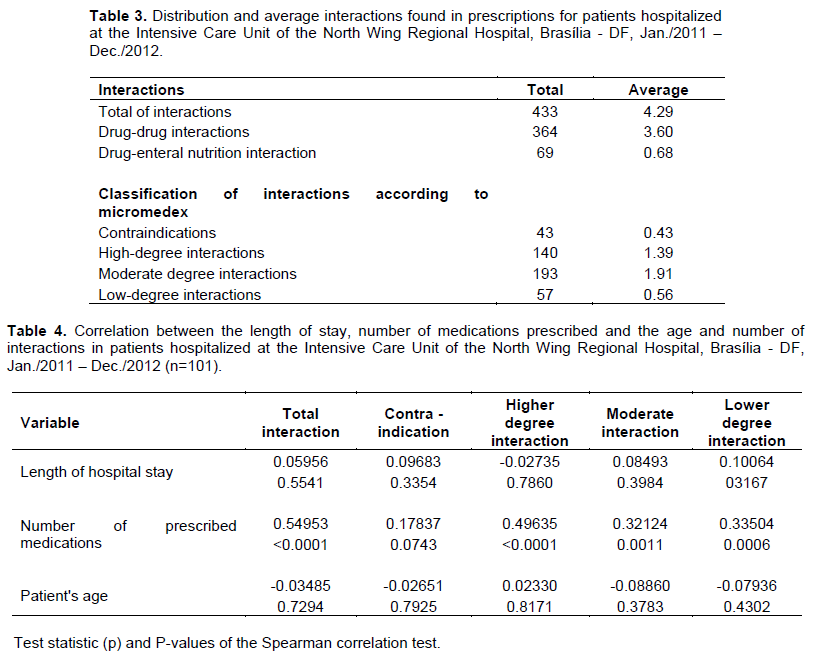
In 101 prescriptions analyzed, 1190 drugs were found. For the "other drugs" classification, medications that are classified into subgroups were grouped and not in the specified groups (Table 3). The drugs for the gastrointestinal tract are most frequent, possibly due to daily use of proton pump inhibitors in order to protect the patient's stomach from the large amount of drug intake, including laxative agents because of reduced intestinal motility which may occur in some cases. Major interactions are described in Tables 3 and 4.
Results also showed that drug-enteral nutrition interactions had an incidence of 15.94%, while drug-drug interactions account for 84.06% of the cases observed. The most frequent drug-drug and drug-enteral nutrition interactions were moderate degree with incidences at 44.57%, followed by high-degree interactions at 32.33%, low-degree interactions at 13.16% and lastly, contra-indications with 9.93% of all prescriptions analyzed.
To assess whether there was a correlation between (a) the time of admission, (b) number of prescribed medications, and (c) the patient's age and the number of interactions found, Spearman correlation was used (Table 4).
As the P-value observed is less than the 5% significance level for the 'number of interactions', 'higher interaction', 'moderate interaction', 'lower interaction' and variables in relation to the 'number of prescribed drugs', there is evidence that leads us to conclude that the number of drugs prescribed and these variables are correlated.
The test statistic (p) reveals that the 'number of prescription drugs' have a moderately strong correlation with the 'number of interactions'. However, the variables 'higher interaction', 'moderate interaction', and 'lower interaction' with the 'number of prescribed drugs' have a moderately weak correlation. Furthermore, since the test statistic (p) is positive in these cases, one concludes that in a moderate way, the greater the number of prescribed drugs, the greater will be the number of interactions (Table 5).
A study by Carvalho et al., 2013, found at least one drug interaction in 793 of the 1124 patients studied. Given that only 320 (28.5%) patients were using enteral nutrition, that study revealed only 3 drug-enteral nutrition cases and 2 drug-drug interactions classified as contraindicated among 2299 interactions found in the first 24 h of hospitalization. After 120 h of admission, those numbers rose to 4 and 5, respectively, out of the 2619 interactions listed. In comparison, the current study shows a much higher frequency of interactions: 69 drug-enteral nutrition interactions and 43 drug-drug interactions classified as contraindicated, out of 433 total interactions found in 101 prescriptions, all of which concerning patients using enteral nutrition, as detailed in Table 3. Although, patients selected in the present study were relatively older (median age of 60 years, against 52.5 years in the reference study) and stayed more time in the hospital ICU (mean hospital stay of 31 days, against 19.4 days in the reference study), the average number of medications used by the patients was very similar: 12 medications against 13.6 in the referred study (Carvalho et al., 2013).
Another study described a high percentage of females (58.4%), similar to this study (49.5%), which had an even gender distribution of patients. However, the percentage of patients who died was only 38%, while reaching 69.31% in this study. The study also showed a list of the most common medications prescribed to be administered by nasoenteric probe (NEP): dimethicone, dipyrone, paracetamol, folic acid, pyrimethamine and sulfadiazine. In comparison, the only medication found in this study in common with the referred study was paracetamol (do Ouro Reis et al., 2010).
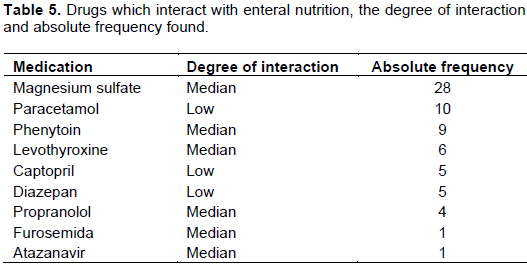
Martins et al., (2013), analyzed 572 prescriptions containing 5283 drugs. He identified medications that should not be administered by nasoenteric tube due to changes that occur when in contact with enteral nutrition. These medications were amiodarone tablets, atenolol, bisacodyl, carbidopa + levodopa, phenytoin, phenobarbital, hydrochlorothiazide, hydroxyurea, retard nifedipine, nimodipine and warfarin. The solubility, absorption and plasma concentration of these medications can be reduced by the presence of enteral nutrition. In the present study, the only medication that
met this criterion was phenytoin, which was present in 9 prescriptions (Martins et al., 2013).
Another study in which most of the 65 patients who entered the study were female (61.5%), 23 (35%) were older than 60. All patients were using some kind of enteral access device; 55.4% were using nasoenteral tube and 44.6% were using nasogastric tube, with median of 8 drugs per patient. The most frequent complications were obstruction and removal, each with frequency of 18.5%. Of the 65 prescriptions, 62 presented interactions (95%). Analysis showed which drugs were involved in potential interactions with enteral nutrition: captopril, omeprazole, KCL syrup, baclofen, phenytoin, valproate and ciprofloxacin. In the present study, 86% of patients were using NE tube and 12% NG tube, 84.6% of the prescriptions presented potential interations, and two drugs that also interact with enteral nutrition in the referred study were present: captopril and phenitoyn (Carvalho et al., 2010).
From the cases included in the study by Silva et al., 2011, were selected 330 prescriptions given to 29 patients using a feeding tube. Of the 29 patients, 26 received enteral medications, of which 55.1% used a nasoenteral tube and 44.9% used a nasogastric tube. The groups of drugs prescribed the most were: antihypertensives (30.9%), anticonvulsants (10%) and antiulcer (7%). Of the 49 medications prescribed to be delivered via enteral access in solid form, 17 were also prescribed in liquid dosage form, which can reduce the risk of tube obstruction. In the present study, drug groups “alimentary tract and metabolism”, including antiulcer (21%) and “nervous system”, including anticunvulsants (20%), surpassed “cardiovascular system”, including antihypertensives (16%), as detailed in Table 2 (Silva et al., 2011).
In a study conducted by Cardinal et al., 2012, 844 prescriptions for 72 patients were analyzed. The median age ranged from 59.04 ± 21.80 years, of which 54.92% were female, with a total presence of 12,052 prescribed drugs, and a median of 14.28 ± 6.31 drugs per prescription, after being classified into 13 therapeutic groups and 55 subgroups according to the Anatomical Therapeutic Chemical. Among the subgroups, the drugs prescribed most were: antibiotics for systemic use, for obstructive diseases of the respiratory tract and analgesics, unlike the present study where the most prescribed drugs were for the digestive tract and metabolism (Cardinal et al., 2012).
No articles were found about research on organic complications that enteral nutrition can cause as incidence of diarrhea, gastric residuals, abdominal distention or vomiting so that we could correlate them.
Knowledge about drug interactions is very important for all health practitioners, especially those prescribing medications in as much as this facilitates the monitoring of effects when the combination is unavoidable. Several authors recommend that medications be administered 1 h before or 2 h after meals. Enteral nutrition, whenever the case, should be interrupted for drug administration, but the infusion procedure should be reinitiated right afterwards and adjusted to meet nutritional needs (Carvalho et al., 2013; Martins et al., 2013; Lopes et al., 2013).
This study was limited with respect to drug-enteral nutrition interactions due to the lack of literature on the topic.
Patients over 60 years outnumbered younger patients, gender distribution was even, over 50% were from other hospital units, complications in consequence of enteral nutrition were alterations in blood glucose (hyperglycemia or hypoglycemia), gastric residue, constipation, diarrhea, abdominal distension and vomiting.
The researchers found 1190 medications in 101 prescriptions. Outcomes revealed a significant number of drug-interactions with an average of 3.60, and drug-enteral nutrition interactions with an average of 0.68; almost one per prescription analyzed.
The statistical analysis showed that the greater the number of medications prescribed, the greater the likelihood of interactions patients will be exposed to. Drug-nutrient interaction is poorly known and occurs in nearly all prescriptions, even when not contraindicated. Furthermore, the expected results of drug absorption are reduced owing to the presence of nutrients. Interactions are closely related to the number of drugs prescribed in addition to risk factors such as age and increase in adverse events.
The authors have not declared any conflict of interests.
REFERENCES
|
Cardinal LSM, Matos VTG, Resende GMMS, Toffoli-Kadri MC (2012). Caracterização das prescrições medicamentosas em unidade de terapia intensiva adulto. Rev. Bras. Ter Intensiva 24(2):151-156.
Crossref
|
|
|
|
Carvalho AMR, Oliveira DC, Neto JEH, Martins BC, Vieira VMSF, Silva LIMM, Ponciano MAS, Fonteles MMF (2010). Analysis of the prescription of patients using enteral catheter in a university hospital of Ceará. Rev. Bras. Farm. Hosp. Serv. Health 1(1):17-21.
|
|
|
|
|
Carvalho REFL, Reis AMM, Faria LMP, Zago KSA, Cassiani SHB (2013). Prevalência de interações medicamentosas em unidades de terapia intensiva no Brasil. Acta Paul Enferm. 26(2):150-157.
Crossref
|
|
|
|
|
do Ouro Reis VG, Ferreira Candido M, Passos de Jesús R, Simões Mendes-Netto R (2010). Perfil de utilización de medicamentos administrados por sonda enteral en el hospital universitario. Rev. Chilena Nutr. 37(3):293-301.
Crossref
|
|
|
|
|
Heldt T, Loss SH (2013). Interação fármaco-nutriente em unidade de terapia intensiva: revisão da literatura e recomendações atuais. Rev. Bras. Ter Intensiva 25(2):162-167.
Crossref
|
|
|
|
|
Lima REF, Cassiani SHDB (2009). Interações medicamentosas potenciais em pacientes de unidade de terapia intensiva de um hospital universitário. Rev. Latino-Am. Enferm. 17(2):222-227.
Crossref
|
|
|
|
|
Lopes EM, Carvalho RBN, Freitas RM (2010). Análise das possíveis interações entre medicamentos e alimento/nutrientes em pacientes hospitalizados. Einstein 8(3):298-302.
Crossref
|
|
|
|
|
Lopes EM, Oliveira EAR, Lima LHO, Formiga LMF, Freitas RM (2013). Interações fármaco-alimento/nutriente potenciais e pacientes pediátricos hospitalizados. Rev. Ciênc. Farm. Básica Apl. 34(1):131-135.
|
|
|
|
|
Martins MR, Soares AQ, Modesto ACF, Carvalho RF, Melo VV, Duarte IP (2013). Análise de medicamentos administrados por sonda em unidades de terapia intensiva em hospital de ensino. Rev. Eletr. Enferm. 15(1):191-196.
Crossref
|
|
|
|
|
Santos L, Martinbiancho J, Tadiotto AL, Kreutz LM (2011). Perfil das interações medicamentosas solicitadas ao centro de informações sobre medicamentos de hospital universitário. Rev. HCPA 31(3):326-335.
|
|
|
|
|
Secretaria de Estado de Saúde do Distrito Federal (BR) (2006). Central de Regulação de Internação Hospitalar da SES/DF. Portaria nËš 41, de 30 de agosto de 2006. Brasília, DF.
|
|
|
|
|
Silva LD, Schutz V, Praça BFM, Santos MER (2010). Interações fármaco-nutrição enteral: uma revisão para fundamentar o cuidado prestado pelo enfermeiro. Rev. enferm. UERJ. 18(2):304-310.
|
|
|
|
|
Silva MJS, Cava CEM, Pedroso PK, Futuro DO (2011). Evaluation of the profile of drug therapy administered through enteral feeding tube in a general hospital in Rio de Janeiro. Braz. J. Pharm. Sci. 47(2):331-337.
Crossref
|
|
|
|
|
Varallo FR, Costa MA, Mastroianni PC (2013). Potenciais interações medicamentosas responsáveis por internações hospitalares. Rev. Ciênc. Farm. Básica Apl. 34(1):79-85.
|
|
|
|
|
Zaban ALRS, Novaes MRCG (2009). Perfil epidemiológico e aspectos econômicos da nutrição enteral domiciliar no Distrito Federal: uma análise histórica de 2000 a 2005. Comun. ciênc. saúde 143-150.
|
|