Full Length Research Paper

ABSTRACT
The study assessed the level of antimalarial drug utilization amongst Staffers of three Health facilities in Rivers State. It was a cross sectional questionnaire based study. The study assessed the knowledge, attitude and malaria treatment and preventive practices of one hundred and five respondents gotten from amongst health workers at Terabor and Ahoada General Hospitals as well as College of Health Science and Management Technology, Health Centre in Port Harcourt. SPSS version 20 was used for the analysis. Chi squared test was used to assess relationships. The study revealed that majority of the Staff respondents were within 18 to 35 age bracket and have had tertiary education. Different frequencies of malaria treatment were also noted ranging from monthly to once a year. 86.6% of the staff reported having used Artemether-Lumefantrine as their drug of first choice for malaria treatment. Dihydroartemisinin/Piperaquine had 6.7% usage while 2.8% and 1.9% were for Artesunate/Amodiaquine and Artesunate/ Sulphadoxine-Pyrimethamine respectively. Non-ACT usage stood at 1.9%. Only 20% of the staff tests all the time before treatment. Most of the Staff also had good knowledge of symptoms of malaria and got their treatment recommendations from qualified personnels such as Doctors and Pharmacists. Six (5.7%) of the Staff still do not complete the treatment regimen either for reasons of feeling better half way or due to unpleasant odour/taste. The major malaria preventive practices prevalent among the staff are covering home windows with net (85.7%) and sleeping under Insecticide treated nets. Artemisinine-based Combination Therapies (ACTs) are the most predominantly used antimalarial amongst staffers of the three Health facilities.
Key words: Antimalarial, drug utilization pattern, Artemisinine-based Combination Therapies (ACTs).
INTRODUCTION
Malaria is still a major public health problem caused by plasmodium parasite species transmitted to human through the bite of infected female Anopheles mosquito. There are five parasite species that cause malaria in humans, namely Plasmodium falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi. Two of these species P. falciparum and P. vivax pose the greatest threat. Malaria is preventable and curable (World Health Organisation, 2019). Although all of the former species may cause significant illness, P. falciparum is responsible for the majority of serious complications and deaths. Drug resistance is an important therapeutic problem, most notably with P. falciparum (Borimas and Nicholas, 2016).
Irrational use of anti-malarial medication is one of the major challenges affecting the prevention, treatment and cure of malaria. This has led to the spread of parasite resistance to most commonly used anti-malarial drugs.
Assessment of drug use patterns with World Health Organization (WHO) drug use indicators is becoming increasingly necessary toward promoting rational drug use in developing countries. Inappropriate drug prescribing is still a global problem (Enwere et al., 2007). Misuse of drugs occurs in all countries and irrational practices are especially common and costly in developing countries (Ghimire et al., 2009). Some studies in Nigeria have revealed that appreciable gaps in knowledge exist with respect to rational drug use among health care professionals (Chukwuani et al., 2002; Okoh, 2012).
Aim of the study
The aim of the study is to assess the antimalarial drug utilization pattern amongst staff of three Health facilities in Rivers State.
Specific objectives
i) To assess the range of antimalarial drugs used by the staffers of the three Health facilities in the study.
ii) To identify the most frequently used anti-malarial drug(s) amongst staff of the three Health facilities.
iii) To find out their level of adherence to national guideline and policy on the diagnosis and treatment of malaria.
iv) To assess the preventive measures used by the study group for malaria control.
MATERIALS AND METHODS
Study design
The study adopted a cross sectional design with the use of questionnaire to obtain the desired information. The population for this study included health workers in the General Hospitals of Ahoada and Terabor and that of the Health Centre of Rivers State College of Health Science and Management Technology, Port Harcourt who consented to participating in the study. A total population of 105 respondents was drawn from the Staff of the Health facilities.
Sample size determination
The sample size of this research was calculated using the Taro Yamane (Yamane, 1973) formula with 95% confidence level.
The calculation formula of Taro Yamane is given as follows:

Where: n = sample size required; N = number of people in the population; e = allowable error (%).
Substituting the numbers into the formula, we have; N = 44, 38 and 33 respectively; e = 5% (0.05). This translates to n = 40, 35 and 30 respectively for General Hospitals Ahoada and Terabor and College of Health Science and Management Technology Health Centre, Port Harcourt.
Data collection technique
The technique of data collection involves the administration of specially adapted and structured questionnaires adopted in the study. The questionnaire consists of three sections; the first section consists of demographic information of the respondents. The second part consists of knowledge based questions as regards signs and symptoms malaria and antimalarial drug utilization while the third section consists of questions on preventive measures and practices against malaria.
Statistical analysis
Data was compiled, presented and analyzed using Statistical Package for Social Sciences (SPSS) software version 20. Chi Square Test was used to determine correlation between variables, and p-value set at 0.05 significant levels.
RESULTS
A total of 130 questionnaires were distributed and 105 was completed correctly and returned. Of these, 35 was from Terabor, 40 from Ahoada and 30 from College of Health Science and Management Technology Health Centre. The results are presented in Tables 1 to 9.








Choice of malarial prophylaxis
About 32.4% (34) of the respondents reported to have been using malaria preventive medications of which 10 do use Proguanil, 7 do use Pyrimethamine , 14 for Sulphadoxine/Pyrimethamine while 3 reported the use of Chloroquine
Cross tabulation between health facility with preferred choice of antimalarial drug and level of adherence.
As shown in Table 10, there is no statistically significant relationship between the health facility and the preferred choice of antimalarial or the level of adherence to national guidelines on malaria treatment.

Cross tabulation between health facility and choice of antimalarial drug switched to after first treatment
Table 11 reveals that there is no statistical significance between the health facilities and the choice of antimalarial drugs.

Cross tabulation between health facility and reasons for switching antimalarial and medication recommendation
In Table 12, there is no statistical significance between the health facilities and reasons for switching antimalarial drug. However, there is strong statistical evidence between health facilities and who recommends the medication, as the respondents are more likely to get prescriptions from a doctor or a pharmacist.

Cross tabulation between health facility and characteristics of antimalarial therapy
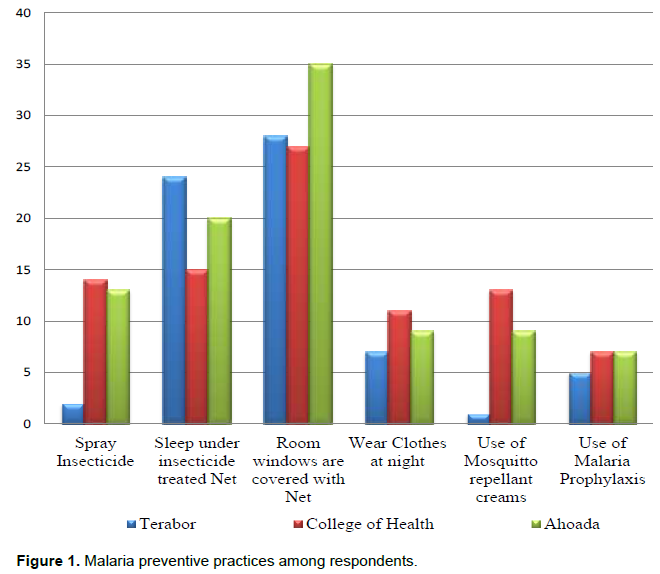
Table 13 shows that there is no statistical significance between the health facilities and testing before treatment, time duration between drug usage and reasons for second dose. Figure 1 describes the malaria preventive practices among respondents.

DISCUSSION
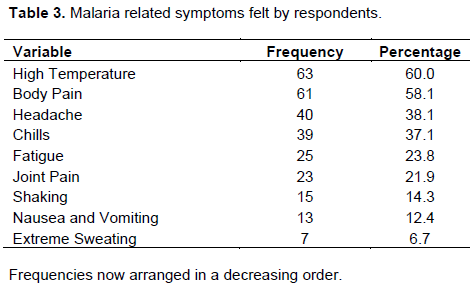
Antimalarial drug utilization pattern can serve as a means to identify causes/origins of drug resistance which increases malaria prevalence and also to evaluate the level of compliance to approved Malaria Treatment Guidelines. The respondents had good knowledge about the signs and symptoms of malaria in this study of which the most reported symptoms included high temperature (69.5%), body pain (47.6%), headache (49.5%), chills (35.2%), nausea and vomiting. These findings are consistent with studies from Ghana and Tanzania as well as that by Modupe et al. (2013) in which knowledge on symptoms of malaria was similar.
ACTs especially Artemeter-Lumefantrine (86.6%) was reported mostly as the drug of first choice for the treatment of malaria infections by the respondents. This is in line with National and WHO Guidelines for the treatment of uncomplicated malarial. From the study generally, 98% utilization was reported as antimalarial drug of first choice. This corresponds with a study carried out by Dodoo et al. (2009) where 90.8% of the respondents used artemisinin-based compound in their treatment regimen. And also that carried out by Ezenduka et al. (2014) where the ACTs recorded 72.7% usage.
On prevalence of malaria, 65.7% of the respondents reportedly develop malaria symptoms within 2 - 6 months. This is quite consistent with a study that revealed that 64.9% of respondents fall ill within 6 months also. 14.3% of the respondents developed symptoms once a year while only 1% rarely develops symptoms. This could be due to a number of reasons such as adequate self-preventive practices amongst others. This is in line with another study conducted in university of Ibadan that concluded that about a third of the volunteers suffered malaria attacks once a year, though a few claimed never to have malaria. This was attributed to the fact that they all had good knowledge of the disease and has developed individual methods of self-management of their malaria attacks (Anumudu et al., 2006). Mosquitoes breed more in the rainy season and hence the prevalence of malaria is always higher in the rainy season (Chigozie et al., 2018).
Health workers in the survey showed good knowledge about the malaria symptoms, demonstrated in their report of high body temperature, headache, fatigue and chills amongst others as symptoms of malaria. This is consistent with other studies that demonstrated knowledge of malaria symptoms such as that carried out by Modupe et al. (2013). Although fever is a symptom of malaria, it is also a symptom of other non-malarial illnesses, hence the need for appropriate diagnosis before treatment as recommended by WHO.
Self-prescribing is still a problem as about 11.4% claim to prescribe drugs for themselves. This is in agreement with the study by Ezenduka et al. (2014) study, who stated that self-medication resulting in the use of monotherapy remains significant with increasing risk of undermining treatment policy, and suggested that additional measures be put in place to directly target consumers and providers in the sector for improved use of anti-malarial drugs in Nigeria. Self-prescribing could mitigate the effort aimed at ensuring rational antimalarial drug use, and as well may cause recrudescence and contribute to malaria resistance, therefore should be discouraged.
Treatment success does not only depend on the use of recommended treatment guidelines but encompasses the correct use of the drug by the patient. In this study, 94.3% of the respondents reported having always completed the recommended doses and their nature of work and work environment may be contributory to this. Switching of medication was also reported among the study group with reasons ranging mostly from treatment failure to cost and side effects of medication. However, it would be interesting to note that artesunate-amodiaquine was the drug about 44% of persons switched to, followed by Dihydroartemisinine/ Piperaquine (31.7%) which are all within WHO antimalarial recommendations. Only about 4.7% still switched to non-ACT monotherapies like Mefloquine, Quinine and Chloroquine which should not be expected from such a study group again.
The use of insecticide treated nets constitutes one of insecticide treated nets while 27.6% agreed to spraying insecticides. This is closely related to a study carried out in the University of Lagos which showed that more than half of the students possessed long lasting insecticide treated nets (LLIN), but not up to half of the students regularly sleep under the treated nets (Olusegun-Joseph et al., 2016). This also agrees with a study that revealed that more than three-quarter of the students (78.1%) knew that LLIN was an effective form of malaria control; however only 55.3% actually reportedly use LLIN in their homes (Chigozie et al., 2018). Few respondents reported their use of malaria prophylaxis. This may not have been necessary if other preventive measures were adopted; however, it agrees with a study carried out in the University of Ibadan which reported that the most used form of preventive measure were the use of Metakelfin (quinine + sulphalene-pyrimethamine), Daraprim (pyrimethamine) and Fansidar (sulphadoxin-pyrimethamine) in addition to bed nests and insecticides (Anumudu et al., 2006). It should be noted that malaria prophylaxis is generally not necessary in persons living in a malarious area because of the risk of lowering one’s resistance to the disease; however, it is required in sickle-cell anaemia patients and non-immune visitors (Federal Ministry of Health, 2005). 95.2% and 96.2% of the respondents reported knowledge of their blood group and genotype respectively. However, of the 101 respondents who reported knowledge of their genotype, 70.3 and 28.7% were respectively AA and AS. Only 1% was SS. Blood group and genotype may be important as it is also related to individual’s malaria susceptibility.
CONCLUSION
The antimalarial most frequently used among staff of the three health facilities were the ACTs with Artemether-Lumefantrine having the highest frequency. They also had adequate knowledge of malaria symptoms and adherence to WHO recommendations was good. However, strict adherence to National guidelines for the treatment of uncomplicated malaria was poor. Not all the preventive strategies for malaria were thoroughly in practice; however, having their home windows covered with nets, sleeping under insecticide treated nets and wearing clothes at night with insecticide spraying were the most utilized methods of malaria prevention among the study group.
RECOMMENDATIONS
1) Concerted efforts should be made towards ensuring strict adherence to National Treatment Guidelines, as well as putting a stop to self-prescribing.
2) Health workers need to take up more responsibilities regarding proper choice of antimalarial medication so that their patients also, can have appropriate recommendations.
3) More campaigns should be channelled towards the adoption of good preventive practices against malaria as this could reduce the incidence rate and consequent drug pressure.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Anumudu CI, Adepoju A, Adediran M, Adeoye O, Kassim A, Oyewole I, Nwuba RI (2006). Malaria Prevalence and Treatment Seeking Behaviour of Young Nigerian Adults. Annals of African Medicine 5(2):82-88. |
|
|
Atif SH, Farzana M, Naila S, Abdul FD (2009). Incidence and pattern of malarial infection at a tertiary care Hospital of Hyderabad. World Journal of Medical Sciences 4:9-12. |
|
|
Borimas H, Nicholas JW (2016). The threat of antimalarial drug resistance. Tropical Diseases, Travel Medicine and Vaccines (2016) 2:10 |
|
|
Chigozie GA, Abdulmuminu I, Deborah OA, Amuche LE (2018). Knowledge and practice of malaria prevention and management among non-medical students of university of Nsukka. The International Journal of Community Medicine and Public Health 5(2):461-465 |
|
|
Chukwuani CM, Onifade M, Sumonu K (2002). Survey of drug use practices and antibiotic prescribing pattern at a general hospital in Nigeria. Pharmacy World and Science 24:188-95. |
|
|
Dodoo C, Fogg A, Asiimwe E, Nartey T, Kodua A (2009). Pattern of drug utilization for treatment of uncomplicated malaria in urban Ghana following national treatment policy change to artemisinin-combination therapy. Malaria Journal 8(1):1-8. |
|
|
Enwere OO, Falade CO, Salako BL. Drug Prescribing Pattern at the Medical Outpatient Clinic of a Tertiary Hospital in South-west Nigeria. Pharmacoepidemiology and drug safety 16(11):1244-1249. |
|
|
Ezenduka CC, Ogbonna BO, Ekwunife OI, Okonta MJ (2014). Drug use Pattern for uncomplicated malaria in Medicine Retail Outlets in Enugu urban, South East Nigeria: Implications for Malaria Treatment Policy. Malaria Journal 13(1):1-10. |
|
|
Federal Ministry of Health (2005). National Malaria and Vector Control Division Abuja-Nigeria February, National antimalarial treatment policy. |
|
|
Ghimire S, Nepal S, Bhandari S, Nepal P, Palaian S (2009). A prospective surveillance of drug prescribing and dispensing in a teaching hospital in western Nepal. The Journal of the Pakistan Medical Association 59(10):726. |
|
|
Modupe IB, Ogbole E, Peter JY (2013): Assessment of Antimalarial Drug Use among the Patients in a Tertiary Hospital in Northern Part of Nigeria. International Journal of Tropical Disease and Health 3(4):283-291. |
|
|
Okoh A (2012). An assessment of rational drug use in public tertiary hospital in Edo state. Nigeria. Geneva Health Forum, GHF, Research Project; 2012. |
|
|
Olusegun-Joseph TS, Oboh MA, Uduak MU (2016). A survey of malaria prevalence and antimalarial preventive measures amongst students of university of lagos, nigeria. African Journal of Clinical and Experimental Microbiology 17(4):267-273. |
|
|
World Health Organisation (WHO) (2019). Factsheet. |
|
|
World Health Organization (WHO) (2015) World Malaria Report. WHO Global Malaria Programme 280 p. |
|
|
Yamane T (1973). Statistics: an introductory analysis. New York: Harper and Row. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


