Full Length Research Paper

ABSTRACT
Medication administration omission errors (MAOE) are very common and often affect patient outcomes and length of stay in the hospitals. This study was a cross-sectional study in which the frequency and causes of MAOE over four weeks at Ndola University Teaching Hospital (NUTH) was assessed. It involved reviewing patients’ drug charts and observation of nurses during the administration of medications to inpatients to detect the MAOE. A total of 259 drug charts were reviewed using a checklist and administered semi-structured questionnaires to 50 nurses who were involved in medication administration to solicit the cause of MAOE. To assess factors associated with MAOE, multivariate logistic regression was used. In this study, 259 drug charts were reviewed of which 220 (84.9%) had one or more MAOE. Of the 1100 doses prescribed to 259 inpatients, 317 doses were omitted resulting in an overall MAOE frequency of 28.8%. In multivariate regression analysis, increased number of medications that the patient used (AOR: 2.18, CI: 1.62-2.94; p=0.0001), being male (AOR: 2.42, Cl: 1.05-5.53: p=0.036) and surgical wards (AOR: 8.56, CI: 3.04 -24.1; p=0.0001) were significant predictors of MAOE. The most common causes of MAOE were the unavailability of medication on the ward followed by work overload. The most omitted class of medication was anti-infective. Medication omission errors are common and affect adult inpatients at Ndola Teaching. There is a need to highlight the magnitude of this problem to promote awareness so that specific interventions are put in place to address the identified causes.
Key words: Medication omission, administration errors, frequency, medication administration.
INTRODUCTION
Medication administration errors (MAE) are common and affect approximately 19.1% of doses to be administered in hospitals (Keers et al., 2013). A systemic review reported that medication administration omission errors (MAOE) are the biggest cause of MAE (Keers et al., 2013). According to the American Society of Health-System Pharmacists, MAOE are defined as failure to administer an ordered dose to a patient (ASHP, 1993).The problem of medication MAOE is common, varying from insignificant to severe and is likely to affect patient outcome measures and length of stay in hospitals (Green et al., 2009). The medication doses prescribed must be administered as intended because failure to do so, has the potential to lead to patient harm (Shandilya et al., 2015).
The omission of charted doses for inpatients has been an important problem and can lead to harm from lack of therapeutic effect (Coleman et al., 2012). The frequency of MAOE varies across the world (Green et al., 2009; Warne et al., 2010; Leite et al., 2016). A frequency of 12.4% for MAOE was reported in the United Kingdom (UK) (Coleman et al., 2012), 22.0% in France (Quélennec et al., 2013) and 71.1% in Brazil (Bohomol et al., 2009). Differences in the study settings and definition of MAOE have all been attributed to variations of error rates reported worldwide (Assiri et al., 2018). Most studies have reported MAOE based on doses rather than the patients (Rostami et al., 2019).
The cause of MAOE is multifactorial and ranges from patients’ refusal to patients’ inability to take medicine (Shandilya et al., 2015, Hossain-Gholipour et al., 2016). The other major reasons reported for the cause of MAOE are medications not being available in the hospital, pharmacy stocking, and delivery problems (Bohomol et al., 2009). Work overload is another factor that has been reported as the cause of MAOE (Oshikoya et al., 2013). Different classes of drugs have been reported to be omitted. One study cited antimicrobials as the most omitted class of drugs and another reported analgesics as the most omitted medications (Latimer et al., 2011). The omission of antimicrobials can lead to treatment failure and the public health problem of antimicrobial resistance (AMR) (Gamela et al., 2021; Poder and Maltais, 2020).
The frequency of MAE has been documented in Zambia with regard to wrong-time medication administration errors (Kampamba et al., 2020). However, there is currently no published study in Zambia regarding MAOE. This study, therefore, sought to evaluate the frequency, causes, and factors associated with medication omission administration errors in medical and surgical departments at Ndola Teaching Hospital.
METHODOLOGY
Study design
This was a cross-sectional study that was done at Ndola Teaching Hospital in the Copper belt province of Zambia, in the medical and surgical departments over four weeks.
Study population
Hospital inpatients, enrolled nurses who administer medications in the Medical and Surgical Departments were the target population. Nurses study population was stratified into enrolled nurses possessing a certificate in nursing and registered nurses who possess a diploma in nursing.
Sample size
The literature review showed a high prevalence (21.4%) of medication omission (Feleke and Girma, 2010), which was applied to determine the sample size as follows:
N= Z2 P (100-P)/e2,
where N=sample size, P= prevalence (In this case going by the reported prevalence on the subject, P=21.4%), Z= standard value corresponding to a particular confidence level (in this case CL is 95% and Z is 1.96) and e=marginal error = 5% N=1.962*0.214*(1-0.214) / 0.052= 259.
The sample size was divided between the two departments by the use of probability proportional to size. The average number of admission per month in Surgery and Medical departments are about 147 and 283, respectively. Medical department 283/430×259 (total sample size)=171 n=171 patient files were reviewed under the medical departments. Surgery department 146/430×259=88 n=88 patient files were reviewed under the surgery department.
Data collection
Medication administration omission errors were detected by the use of the direct observation method and review of patient’s drug charts and files. The observation method was done on nurses who were selected by convenience sampling as most drugs were administered by a single nurse. This method was selected as it has been shown to be the best error detection method in terms of accuracy (Allan and Barker, 1990). At the start of the observation period, each nurse was given written consent and had the option of accepting or refusing to take part in the study. The study utilized an interviewer-administered structured questionnaire with closed and a few open-end questions to solicit information for the causes of MAOE by nurses who were directly involved in drug administration. A total of 259 drug charts and files of all inpatients aged 18 years and over were randomly selected.
These were screened daily for four weeks from Monday to Sunday in the morning and afternoon for MAOE using the checklist. The screening had verified the eligibility of prescriptions in the medication chart if they were identical to the prescriptions in the medical notes, and examine whether the prescriptions charts were unclear. Patient files and drug charts were used to determine the frequency of MAOE, classes of drugs omitted, and comparing the error rates of MAOE between the two departments of internal medicine and surgery. The basic data in the study was the number of actual errors divided by the total number of opportunities for errors. In this study, both the proportions of dose omissions as well as the proportions of patients with omissions were evaluated. Each treatment chart was counted only once, regardless of how many times it was seen. Failure to defined as MAOE owing to a lack of administrative accountability. If the patient refused the medication, the opportunity for errors was counted provided the nurse responsible for administering the medication tried to give it. Doses that were withheld according to policies calling for withholding of medication doses such as nothing by mouth before surgery or hold until the condition improves were excluded as opportunities for MAOE.
Data analysis instrument and procedure
Numerical data collection in this study was subjected to coding, categorization and then entered into a computer software aided analysis. Tables were developed where relevant. The data was analysed using Statistical Package for Social Science (SPSS) version 20. For categorical variables, data were expressed as numbers and percentages. For parametric continuous variables, we reported the mean and their corresponding standard deviation (SD). For nonparametric continuous variables, median and interquartile ranges (IQR) were reported. A Pearson-Chi-square test was used to compare the MAOE frequencies of categorical variables. To detect the difference between two medians of continuous variables, the Wilcoxon-Mann Whitney rank-sum test was used. Bivariate logistic regression analysis was conducted for each independent variable separately and independent variables with the p-value < 0.2 were included into multivariate logistic regression model. The variables with P-value < 0.05 in the final model were considered as associated factors of MAOE. All statistical tests were two-sided with a p-value ? 0.05 considered statistically significant.
Ethical considerations and approval
Ethical approval and permission was sought from the University of Zambia School of Health Science Research Ethics Committee (UNZAHSREC) protocol ID number (20171226144) to undertake the study. Additionally, permission was also sought from Ndola University Teaching Hospital management. Consent was sort and obtained from the nurses who were the members of staff for their participation in the answering of a questionnaire on the factors causing the medication omission errors. No name or any form of identification of the members of staff was obtained and no patients’ names were recorded on the checklist.
RESULTS
Of 259 patients reviewed, 171 (66%) patients were from the medical wards and 88 (34%) patients from the surgical wards. The patients’ median age was 43 (IQR=34, 54). The majority 104 (40.2%) of patients stayed in the hospital for 3 to 4 days. A total of 50 nurses were involved in the study with a median age of 25 years (IQR=23, 27) and median years of service of 4 (IQR=2, 6). The mean number of patients seen per day by a nurse in the medical wards was 44 (SD= ±7) and in surgical wards, the mean number was 31(SD= ±6) shown in Table 1.

Frequency of medication administration omission errors
In this study, 259 drug charts were reviewed, of which 220 (84.9%) had one or more medication omissions. Of the 1100 doses prescribed to 259 inpatients, 317 doses were not administered to the patients resulting in an overall medication omission error frequency of 28.8% as shown in Figure 1.

Comparison of medication administration omission errors by category
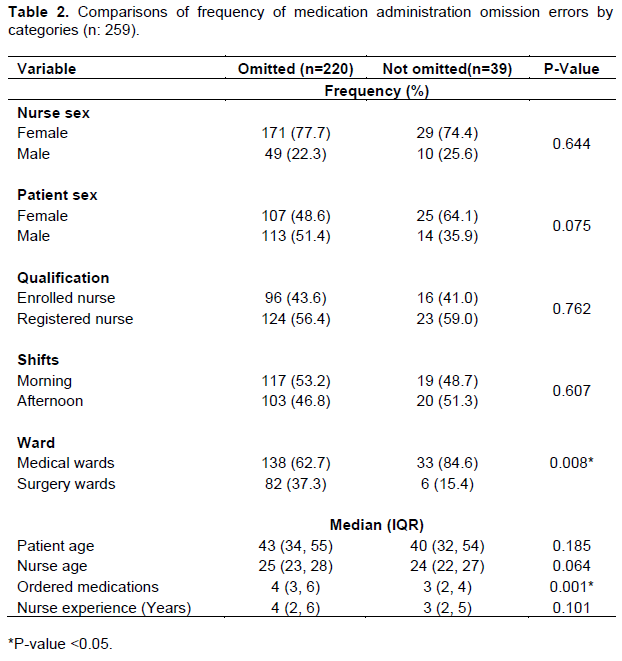
When sex of the patients was compared, there was a high proportion of male patients among the omitted medications than not omitted (51.4% vs. 35.9%, [p=0.075]). Additionally, when the age of the patients was also compared, the medication omissions were more in older patients than in younger patients (median age: 43, IQR [34, 55] vs. median age: 40, IQR [32, 54]: [p=0.185]). Furthermore, when the ordered number of medication was compared, there was significantly more medication omissions in patients prescribed with more number of medications than with less number of medications (median number: 4, IQR [3, 6] vs. median number: 3, IQR [2,4], [p=0. 0.001]). There was a high proportion of female nurses among medication omissions than not omitted (77.7% vs. 74.4%, [p=0.644]). When the age of the nurses was compared, the medication omissions were more in older nurses than in younger nurses (median age: 25, IQR [23, 28] vs. median age: 24, IQR [22, 27]: [p=0.064]). When the qualifications of nurses were compared, there was a high proportion of registered nurses among the omitted medications than not omitted (56.4% vs. 59.0% [p=0.075]). Medication omissions were also more among the nurses with more working experience than those with less working experience (median working experience: 4, IQR [2, 6] vs. median working experience: 3, IQR [2, 5]: [p=0.101]). There was significantly a high proportion of medical wards among the medications omissions than not omitted (62.7% vs. 84.6% [p=0.008]). There was also a high proportion of morning shift among the medications omissions than not omitted (53.2% vs. 48.7% [p=0.607]) shown in Table 2.
The most commonly omitted classes of medication
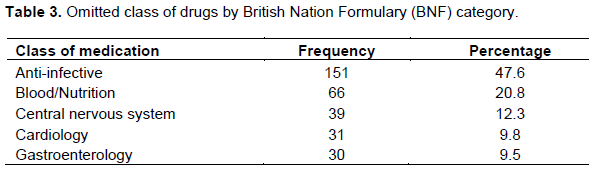
The types of medication omitted were classified according to the British National Formulary classification of which five classes of medications were identified for the treatment of various ailments. The most omitted classes of medication were anti-infective 151 (47.6%), seconded by blood/nutrition 66 (20.8%), and central nervous system 39 (12.3%) shown in Table 3.
Causes of medication administration omission errors
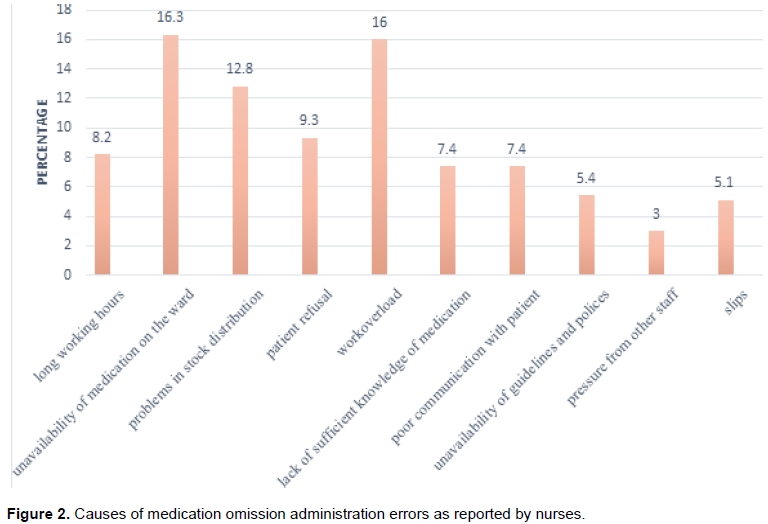
The most common cause of MAOE as reported by the nurse as shown in Figure 2 was the unavailability of medication on the ward represented by 16.3%. The second most common factor was work overload this was the case in 16% of the nurse’s responses. Problems in the stock distribution in the pharmacy (12.8%) was the third followed by patient refusal (9.3 %), unavailability of policies and guidelines (9.0%), long working hours (8.2%), nurse inexperience and lack of sufficient knowledge of medication (7.4%), poor communication with the patient (5.4%), slips (5.1%) and pressure from other staff (3.0%).
Factors Associated with Medication Administration Omissions Errors
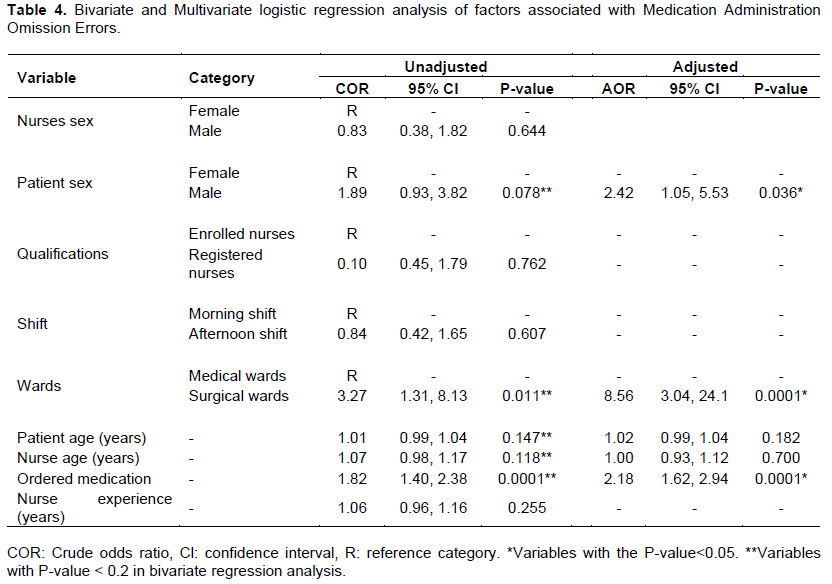
Based on bivariate analysis, surgical wards (COR: 3.27-CI: 1.31-8.13: p=0.011) were significantly associated with higher likelihood of MAOE when compared with medical wards. Being male (AOR: 1.89, Cl: 0.93-3.82; p=0.078) was not significantly associated with MAOE. Additionally, for every one medication added to the list of medicines, there was a significant association with an increase in the chances of MAOE (COR: 1.82, CI: 1.40, 2.38; p=0.0001). In multivariate regression analysis, being male (AOR: 2.42, Cl: 1.05-5.53; p=0.036) and surgical wards (AOR: 8.56, CI: 3.04 -24.1; p=0.0001) were significantly associated with MAOE. For every one medication added to the list of medicine, there was significant association with an increase in the chances of MAOE (AOR: 2.18, CI: 1.62 -2.94; p=0.0001) shown in Table 4.
DISCUSSION
MAOE fall into the wide category of medication administration errors (Latimer et al., 2011). The frequency of MAOE per patient ranges from 26 to 79% and in this study, an omission frequency per patient of 84.9% was found, which was more than what was reported by other studies (Shandilya et al., 2015, Latimer et al., 2011; Warne et al., 2010). The high frequency of MAOE observed in this study could be attributed to the study setting as it has been implicated to influence the difference in the frequency of MAOE reported worldwide (Assiri et al., 2018). Nurses in both surgical and medical wards cited medication unavailability as the most cause of MAOE and this could have hugely contributed to the high frequency of medication omission observed in this study. One study reported medication shortage in the institution as the main contributing driver for the increase in MAOE frequency (Silva et al., 2011). The other reason could have been the failure to sign on the drug chart after administering medication to the inpatients which may partly be a failure to document nursing care owing to interruptions rather than a genuine MAOE.
Additionally, the omission frequency per medication dose was found to be 28.8%, suggesting that 1 in every 4 doses were omitted. This study identified a much higher omission frequency per medication dose than that of 21.4% reported in Ethiopia (Feleke and Girma, 2010), 7.5% in Australia (Munzner et al., 2012), 18.5% in Malaysia (Shitu et al., 2020), 11% in Australia (Latimer et al., 2011), 20% in the UK (Green et al., 2009), 16.6% in Iran (Hossain-Gholipour et al., 2016), 2.63% reported in Brazil (Dalmolin et al., 2013), 7.6% in Australia (Lawler et al., 2004) 1.4% (Rodriguez-Gonzalez et al., 2012) and 21% in Brazil (Leite et al., 2016). The frequency of MAOE per medication dose is higher in this study than those reported in other studies probably due to differences in study settings. Studies have reported a low frequency of medication errors in hospitals with robust healthcare systems where there is the presence of clinical pharmacists working on the wards (De Oliveira Jr et al., 2017; Pevnick et al., 2018; Assiri et al., 2018). Studies have also shown that methodologies employed for error detection can also affect the variation of reported frequency of MAOE (Assiri et al., 2018).
Predictors of medication omission errors such as patient factors, nursing staff, nursing experience, nurse-physician communication, pharmacy processes, and overburdened healthcare system have been reported by several studies (Hammoudi et al., 2018; Härkänen et al., 2015; Rasool et al., 2020). This study reviewed that the increased number of medications that the patient used was a statistically significant predictor of medication omission. This is also supported by other studies (Rostami et al., 2019; Härkänen et al., 2015; Rasool et al., 2020). Polypharmacy is a rising worldwide problem owing to an aging population and the increasing prevalence of multimorbidity (Duerden et al., 2013). Therefore, it is important to identify methods of improving avoidable polypharmacy. In this study, being male was significantly associated with medication omission. This finding was in contrast to what was reported by another study (Latimer et al., 2011). Regarding the wards, surgical wards were significantly associated with MAOE compared to medical wards. This finding is highlighted elsewhere by the other studies (Leite et al., 2016; Rostami et al., 2019).
The most common causes of MAOE in this study as cited by nurses were unavailability of medication on the ward (16.3%) and work overload (16%). Other studies also reported the unavailability of medications as the most cause of MAOE (Green et al., 2009; Munzner et al., 2012). An increase in workload has also been reported by other studies as a major driver MAOE (Oshikoya et al., 2013). This is in agreement with the nurse to patient ratio reported in this study which was one nurse to every forty-four patients (SD=±7) in medical wards and one nurse to every thirty-one patients (SD= ±6) in surgical wards. One study on medication administration errors in Zambia also reported a similar nurse to patient ratio which is way above the World Health Organisation (WHO) recommendations (Kampamba et al., 2020). Therefore, there is a need to increase the workforce in hospitals to curb medications errors in general.
This study observed that the most commonly omitted classes of medication were anti-infective (47.6%) followed by blood/nutrition (20.8%). This was supported by other studies which highlighted anti-infective medications as the most omitted medications (Grissinger, 2017; Munzner et al., 2012; Isaac et al., 2012). One of the reasons in our study for the omission of these antimicrobials could be attributed to the out-of-stock at the pharmacy making them unavailable on the ward. Others studies have found analgesia (Latimer et al., 2011), nervous system (Leite et al., 2016), and gastroenterology (Shandilya et al., 2015) medications as the most omitted medications. The differences in the classes of medication omitted could be due to differences in geographical locations as the prevalence of both communicable and non-communicable diseases may vary according to location which in turn may affect the pattern of prescribing medications (Moreno-Betancur et al., 2018; Boutayeb, 2010). Doctors, nurses, and pharmacist need to be alerted that most of the doses omitted in this study involved anti-infective drugs and highlight the potential effects of the omitted dose such as antimicrobial resistance (AMR) that is now emerging as a global health problem (Gamela et al., 2021).
This study had some limitations. Firstly, it is likely that the Hawthorne effect increased on the nurses who were being observed as they were informed about the study. However, the observation method is one of the accurate methods that have been used to identify medication administration errors (Kampamba et al., 2020). Secondly, this was a facility-based study and we were unable to generalize the findings. Lastly, medications without a signature on the drug charts were presumed to have not reached the patient and maybe in some cases, it could have just been the failure to document the medications that were administered to the inpatients.
CONCLUSION
Medication administration omission error is increasingly becoming an area of concern throughout the inpatients' hospital stay. This study found that a good proportion of patients were affected by omitted medications and the most omitted medications were anti-infective raising serious concerns regarding antimicrobial drug resistance. The main cause of medication omissions in this study was the unavailability of medication on the ward followed by work overload. Therefore, there is a need to direct specific interventions towards the causes of MAOE in order to reduce their occurrence.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors thank the University of Zambia, School of Health Sciences and Pharmacy Department for supporting this study.
REFERENCES
|
Allan EA, Barker KN (1990). Fundamentals of medication error research. American Journal of Hospital Pharmacy 47(3):555-571. |
|
|
ASHP (1993). ASHP guidelines on preventing medication errors in hospitals. American Journal of Hospital Pharmacy 50(2):305-314. |
|
|
Assiri GA, Shebl NA, Mahmoud MA, Aloudah N, Grant E, Aljadhey H, Sheikh A (2018). What is the epidemiology of medication errors, error-related adverse events and risk factors for errors in adults managed in community care contexts? A systematic review of the international literature. British Medical Journal Open 8(5):e019101. |
|
|
Bohomol E, Ramos LH, D'Innocenzo M (2009). Medication errors in an intensive care unit. Journal of Advanced Nursing 65(6):1259-1267. |
|
|
Boutayeb A (2010). The burden of communicable and non-communicable diseases in developing countries. Handbook of disease burdens and quality of life measures P 531. |
|
|
Coleman JJ, McDowell SE, Ferner RE (2012). Dose omissions in hospitalized patients in a UK hospital. Drug Safety 35(8):677-683. |
|
|
Dalmolin GR, Rotta ET, Goldim JR (2013). Medication errors: classification of seriousness, type, and of medications involved in the reports from a University Teaching Hospital. Brazilian Journal of Pharmaceutical Sciences 49:793-802. |
|
|
De Oliveira Jr, Castro-Alves LJ, Kendall MC, McCarthy R (2017). Effectiveness of Pharmacist Intervention to Reduce Medication Errors and Health-Care Resources Utilization After Transitions of Care: A Meta-analysis of Randomized Controlled Trials. Journal of Patient Safety 17(5):375-380. |
|
|
Duerden M, Avery T , Payne R (2013). Polypharmacy and medicines optimisation. Making it safe and sound. London: The King's Fund. |
|
|
Feleke Y, Girma B (2010). Medication administration errors involving paediatric in-patients in a hospital in Ethiopia. Tropical Journal of Pharmaceutical Research 9(4). |
|
|
Gamela D,Hikaambo CN, Mfune RL, Kampamba M. Mufwambi W, Kasanga M, Chileshe M, Daka V, Banda DC. Banda M, Steward M (2021). Antibiotic susceptibility and resistance patterns of diarrhoeagenic Escherichia Coli, Shigella and Salmonella species: A need for antimicrobial stewardship and surveillance programmes. |
|
|
Green C, Du-Pre P, Elahi N, Dunckley P, McIntyre A (2009). Omission after admission: failure in prescribed medications being given to inpatients. Clinical Medicine 9(6):515-518. |
|
|
Grissinger MC (2017). Omission of high-alert medications: a hidden danger. American Journal of Nursing 117(7):66-70. |
|
|
Hammoudi BM, Ismaile S, Abu Yahya O (2018). Factors associated with medication administration errors and why nurses fail to report them. Scandinavian Journal of Caring Sciences 32(3):1038-1046. |
|
|
Härkänen M, Ahonen J, Kervinen M, Turunen H,Vehviläinen?Julkunen K (2015). The factors associated with medication errors in adult medical and surgical inpatients: a direct observation approach with medication record reviews. Scandinavian Journal of Caring Sciences 29(2):297-306. |
|
|
Hossain-Gholipour K, Mashallahi A, Amiri S, Moradi Y (2016). Prevalence and cause of common medication administration errors in nursing. Journal of Chemical and Pharmaceutical Sciences pp. 18-21. |
|
|
Isaac R, Walele F, Cox A (2012). The significance of dose omissions in the paediatric intensive care unit. Archives of Disease in Childhood 97(5):e8-e9. |
|
|
Kampamba M, Mwanza T, Saini K , Hatwiko H , Biete L , Hikaambo CN (2020). Wrong time medication administration errors: Frequency and their causes at Adult University Teaching Hospitals in Zambia. African Journal of Pharmacy and Pharmacology 14(10):362-369. |
|
|
Keers RN, Williams SD, Cooke J, Ashcroft DM (2013). Prevalence and nature of medication administration errors in health care settings: a systematic review of direct observational evidence. Annals of Pharmacotherapy 47(2):237-256. |
|
|
Latimer SL, Chaboyer W, Hall T (2011). Non?therapeutic medication omissions: incidence and predictors at an Australian Hospital. Journal of Pharmacy Practice and Research 41(3):188-191. |
|
|
Lawler C, Welch SA, Brien JE. (2004). Omitted medication doses: frequency and severity. Journal of Pharmacy Practice and Research 34(3):174-177. |
|
|
Leite B, Mistro S, Carvalho C, Mehta SR, Badaro R (2016). Cohort study for evaluation of dose omission without justification in a teaching general hospital in Bahia, Brazil. International Journal for Quality in Health Care 28(3):288-293. |
|
|
Moreno-Betancur M, Koplin JJ, Ponsonby AL, Lynch J, Carlin JB (2018). Measuring the impact of differences in risk factor distributions on cross-population differences in disease occurrence a causal approach. International Journal of Epidemiology 47(1):217-225. |
|
|
Munzner EE, Welch SA, Richardson KL (2012). Measuring and describing dose omissions using an electronic medication management system. Journal of Pharmacy Practice and Research 42(4):264-267. |
|
|
Oshikoya KA, Oreagba IA, Ogunleye OO, Senbanjo IO, MacEbong G, Olayemi SO (2013). Medication administration errors among paediatric nurses in Lagos public hospitals: an opinion survey. International Journal of Risk and Safety in Medicine 25(2):67-78. |
|
|
Pevnick JM, Nguyen C, Jackevicius CA, Palmer KA, Shane R, Cook-Wiens G, Rogatko A, Bear M, Rosen O, Seki D (2018). Improving admission medication reconciliation with pharmacists or pharmacy technicians in the emergency department: a randomised controlled trial. British Medical Journal Quality and Safety 27(7):512-520. |
|
|
Poder TG, Maltais S (2020). Systemic analysis of medication administration omission errors in a tertiary-care hospital in Quebec. Health Information Management Journal 49(2-3):99-107. |
|
|
Quélennec B, Beretz L, Paya D, Blicklé JF, Gourieux B, Andrès E, Michel B (2013). Potential clinical impact of medication discrepancies at hospital admission. European Journal of Internal Medicine 24(6):530-535. |
|
|
Rasool MF, Ur Rehman A, Imran I, Abbas S, Shah S, Abbas G, Khan I, Shakeel S, Hassali MA, Hayat K (2020). Risk Factors Associated With Medication Errors Among Patients Suffering From Chronic Disorders. Frontiers in Public Health 8. |
|
|
Rodriguez-Gonzalez CG, Herranz-Alonso A, Martin-Barbero ML, Duran-Garcia E, Durango-Limarquez MI, Hernández-Sampelayo P, Sanjurjo-Saez M (2012). Prevalence of medication administration errors in two medical units with automated prescription and dispensing. Journal of the American Medical Informatics Association 19(1):72-78. |
|
|
Rostami P, Heal C, Harrison A, Parry G, Ashcroft DM, Tully M P (2019). Prevalence, nature and risk factors for medication administration omissions in English NHS hospital inpatients: a retrospective multicentre study using Medication Safety Thermometer data. British Medical Journal Open 9(6):e028170. |
|
|
Shandilya S, Nizamuddin K, Faisal MW, Noor S, Abraham S (2015). Omitted medications: a continuing problem. Clinical Medicine 15(1):12-14. |
|
|
Shitu Z, Aung MM, Kamauzaman THT (2020). Prevalence and characteristics of medication errors at an emergency department of a teaching hospital in Malaysia. Biomed Central Journal health services research 20(1):1-7. |
|
|
Silva AE, Reis AM, Miasso AI, Santos JO, Cassiani SH (2011). Adverse drug events in a sentinel hospital in the State of Goiás, Brazil. Revista Latino-Americana de Enfermagem 19:378-386. |
|
|
Warne S, Endacott R, Ryan H, Chamberlain W, Hendry J, Boulanger C, Donlin N (2010). Non?therapeutic omission of medications in acutely ill patients. Nursing in Critical Care 15(3):112-117. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


