Full Length Research Paper

ABSTRACT
Dietary supplements, particularly nutraceuticals, are an expanding sector on the South African market, especially since the beginning of the COVID-19 pandemic. However, regulatory authorities do not regulate nutraceuticals and concern arose regarding safety, quality and efficacy of the product reaching the end-user. The aim of the study was to evaluate the pharmaceutical quality, specifically the physical and the in-vitro release properties of two commonly marketed L-lysine products in South Africa. An experimental design was used. Two L-lysine products, a tablet and a capsule, available on the South African market were evaluated for pharmaceutical quality. Tests performed were: Weight variation test, dimensions test, friability test, hardness test, assay, and drug release studies. The quality of products was compared to official USP standards. Tablets were of consistent diameter, length and thickness. Not more than 2 tablets had weights outside the 5% deviation range for each sample. Tablets had an average friability of 17.56%, although their hardness was greater than the acceptable range. All tablets disintegrated within the 15 min. Two out of three samples had amount of lysine below the acceptable range. Tablets sampled released just about 70% of the contained L-lysine by 45 min. Capsules had inconsistent powder weight and contained an amount of L-lysine less than the label claim. Capsules disintegrated within 4 min and released just over 75% of drug by 45 min. There seems to be inconsistences in the characteristics of L-lysine products and their quality cannot be guaranteed. More investigations on other marketed L-lysine products are suggested, to further advice on the necessity of a relook of their quality assurance procedures and labelling.
Key words: Nutraceuticals, pharmaceutical quality, L-lysine.
INTRODUCTION
The range of dietary supplements now available on the South African market accessible to the consumer has increased particularly since the beginning of the COVID-19 pandemic. Nutraceuticals in particular, are an expanding sector to this market. Nutraceuticals are defined as forms of raw materials derived from food sources, which are then formulated into dosage forms such as tablets, capsules or powders which claim physiological benefits (Sarris et al., 2016; Banach et al., 2018). Both pharmaceutical companies, small and big, and consumer food companies are increasingly moving into the area, either by expansion or acquisition of nutraceutical suppliers. Two of the most popular products, and subjects of a number of investigations, are chondroitin and glucosamine. Chondroitin, as a sulphate, is a natural substance and an essential component of cartilage that plays an important role in the elasticity and function of articular cartilage where it is mainly attached covalently to core proteins in the form of proteoglycans. It is usually manufactured from animal sources, such as shark and cow cartilage (Gupta and Yadav, 2022). It can also be made in a lab. Some chondroitin sulfate products are not labeled accurately (Russell et al., 2002). Glucosamine is a natural sugar that exists in the fluid around the joints, as well as in animal bones, bone marrow, shellfish, and fungi. The glucosamine in supplements usually comes from the shells of shellfish, though there is also a synthetic form. These products have been shown to have variable compliance with labelled contents, probably caused by the use of a range of sources of starting materials and the chemical forms used (Lockwood, 2015). This may explain the reason why standardized global regulations are difficult to develop for such products. A few individual nutraceuticals, such L-lysine, may be classified as medicines in certain countries, and as such subject to medicine regulations. For example, in the US, they are largely unregulated as they exist in the same category as dietary supplements and food additives by the FDA, under the authority of the Federal, Drug, and Cosmetic Act (FDA, 2016; Kaplan, 2019). Bioavailability of nutraceuticals of L-lysine is dependent on a number of factors, including solubility of raw material. In South Africa L-lysine is available in two pharmaceutically styled formulations, namely tablets and capsules whose pharmaceutical quality the consumer is never quite certain about.
Quality entails that a product is free of defects, thus it delivers the properties claimed. In other words, there is a consistent and safe delivery of the active ingredient. Pharmaceutical quality system assures that the desired product quality is routinely met, suitable process performance is achieved, the set of controls are appropriate, improvement opportunities are identified and evaluated, and that the body of knowledge is continually expanded (Iser, 2015). In addition to all this, there is the concept of Quality by Design (QbD) which all regulatory agents must see to it that it is well understood by manufacturers. QbD is a scientific proof of commitment in accurate use of required limits from the initial step in production of pharmaceutical product to final product in packaging. It contributes to characteristics, namely dosing, safety and efficacy of any pharmaceutical product which includes supplements/nutraceuticals like L-lysine. Dietary supplements, particularly nutraceuticals, are an expanding sector on the South African market, especially since the beginning of the COVID-19 pandemic. However, regulatory authorities do not regulate nutraceuticals and a concern arises regarding safety, quality and efficacy of the product reaching the end-user. The present study was carried out with the aim of evaluating the pharmaceutical quality, specifically the physical and the in-vitro release properties of two commonly marketed L-lysine products in South Africa.
MATERIALS AND METHODS
L-lysine tablets, L-lysine capsules were purchased from two pharmacies in South Africa. Vernier calliper (Fragram, South Africa); Hardness tester (Schleuniger, Switzerland); Friabilator (Roche, USA); Disintergrator (Pharma Test, Germany); Weighing balance (College B154, Mettler Toledo, South Africa); Dissolution tester (Hanson Research SR8-Plus, USA); and UV spectrophotometer (Biobase, China). The products (dosage forms) were evaluated in terms of the following physical properties.
Dimensions
Tablet dimensions (thickness, length and diameter) were determined using a Vernier calliper. Ten tablets were selected and the respective thickness, diameter, and length were measured.
Weight variation test
Twenty tablets were selected randomly and weighed individually. For capsules, the contents of 20 capsules were weighed individually. The average weights and standard deviations (SD) of tablets and of the capsules were calculated. The individual weights of tablets were compared to the average weight of tablets, and the individual weights of capsules were compared to the average weight of contents of capsules. Dosage units pass the weight variation test if not more than two dosage units fall outside the percentage limit and if no dosage unit differs by more than two times the percentage limit (USP, 2019: 492). For tablets or capsule weight of less than 0.3g, a 7.5% deviation range is allowed whilst for tablets or capsules of 0.3g and more, a 5% deviation limit is allowed.
Hardness test
Hardness of ten individual tablets was measured by a hardness tester (USP, 2019). The average hardness of the ten tablets was calculated and a 5% deviation from the average was calculated. To pass the hardness test, not more than 2 tablets from the sample were supposed to be outside the 5% deviation range.
Friability test
Twenty tablets randomly selected were weighed and their weight recorded. The tablets were placed in a Roche friabilator and rotated at the speed of 25 rpm for 100 revolutions. The tablets were then removed from the friabilator, dusted off the fines and weighed again (Dubey and Arora, 2012). Percentage loss was calculated according to the following equation:

Tablets pass friability test if the percentage friability is less than 1%.
Quantity of L-lysine in dosage units
The quantity of lysine in tablets and capsules was assessed as per method described by (Shahidi, 2012). Firstly, one tablet was crushed and dissolved in a 100ml volumetric flask, then labelled stock solution A. For capsules, the powder contents of one capsule were emptied and dissolved in a 100ml volumetric flask, then labelled stock solution A. 5 ml was withdrawn from the stock solution with a syringe, filtered and placed into a 100ml volumetric flask. The volumetric flask was then filled to the mark with distilled water and labelled as sample A. Absorbance was measured at 270 nm. The same procedure of withdrawing 5ml samples from the stock solution and diluting was repeated to make sample B and sample C. Standard solutions were prepared by weighing 500mg of lysine, dissolving in 1000 ml of distilled water and labelling the solution as solution A. 10ml was taken from solution A, diluted to 1000 ml with distilled water and labelled as stock solution A. 10ml was withdrawn from the stock solution, added to a 100ml volumetric flask and filled to the mark. The solution was then labelled as Standard solution A. 20 ml was then withdrawn from the stock solution, added into 100ml volumetric flask and filled to the mark. The solution was labelled as Standard Solution B. 40 ml was withdrawn from the stock solution, added into a 100 ml volumetric flask and labelled as stock solution C. 5 ml was withdrawn from the prepared standard solution separately using a syringe and filtered into 100ml volumetric flask using 0.45 μm filter. It was then filled to the mark using distilled water and the absorbance was measured at 270 nm wavelength, used the distilled water as a blank. The amount of lysine contained in the dosage forms was then calculated. To pass the Assay test, dosage forms should contain between 95 to 105% of the stated amount of the active ingredient.
Disintegration test
Disintegration test was performed as per method described by Chartuvedi et al, 2017. A Pharma Test® disintegration tester was used which had 5 glass tubes (77.5 ± 2.5 mm long and 21.5 mm internal diameter) with a 10 number mash at the bottom. The dosage forms (tablets or capsules) were placed in the glass tubes and placed in a medium simulated to the disintegration environment which was maintained at 37 ± 2ºC in a one litre vessel. This method was made to move up and down through a distance of 5 to 6cm at a frequency of 30 cycles per minute. Dosage forms remained 2.5 cm below the surface of liquid on their upward movement and not closer than 2.5 from the bottom of the beaker in their downward movement. The time taken for each dosage form to disintegrate was noted.
Drug release profile
Dissolution testing determines the rate of drug release from dosage forms and dissolves in a particular dissolution medium. Lysine release from the tablets and capsules was examined separately, using six (6) randomly selected units from each formulation. A SR8® dissolution apparatus 2 was used with 900 ml sterile water at 37 ºC ± 0.5 ºC as medium. Rotation speed of paddle was 75 rpm was used. Samples (5 ml) were taken from the dissolution apparatus at set time intervals (15 30 45 and 60 min), and the medium was replaced with an equal volume of fresh medium at each time interval. The samples taken were filtered using a 0.45 μm and absorbance was measured (Charturved et al, 2017). Percentage drug release was then calculated.
RESULTS AND DISCUSSION
Tablet dimensions
The results of measurements of tablet dimensions (length, width and thickness) are depicted in Figures 1 to 3, respectively. As indicated in the method the average thickness, length and diameter of the sample were calculated and allowable 5% deviation range from the average was also determined. The results obtained were as follows:
Length = 2.29 mm ± 5% = 2.18 - 2.40 mm
Width = 0.991 mm ± 5% = 0.94 mm - 1.04 mm
Thickness = 0.673 mm ± 5% = 0.64 mm - 0.71 mm
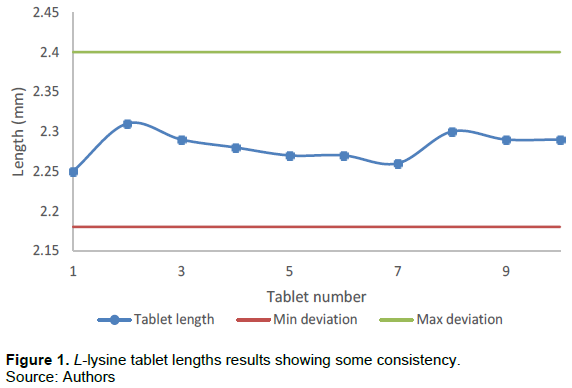
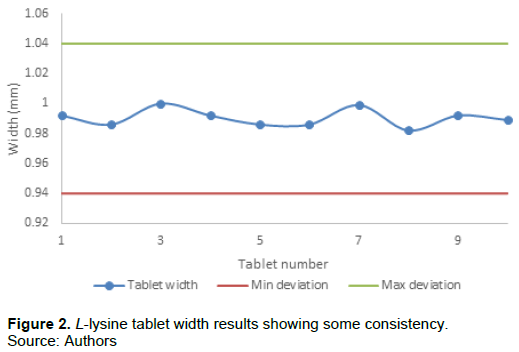
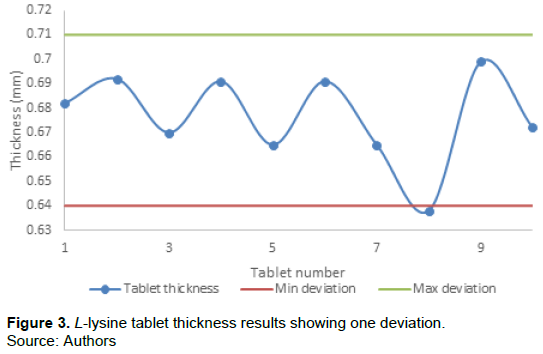
Average tablet length, width and thickness were 2.28 ± 0.1 mm, 0.99 ± 0.1 mm and 0.67 ± 0.2 mm, respectively. None of the deviations of the L-lysine tablet length and width exceeded ± 5%. However, only one tablet thickness measurement exceeded the 5% deviation. Therefore, tablets passed the dimension test. Since there appeared, generally, to be consistency in the length, width and thickness of tablets, it was reasonable to conclude that tablets were of acceptable quality according USP standards. The standards do not accept more than two tablets to be outside the deviation range. The thickness, length and diameter/width of tablets are important for uniformity of tablet size. Uniformity of tablet size amongst tablets of the same batch indicates reproducibility and consistence of quality in the manufacturing process. Consistency in quality gives the end an enlightened user confidence in the formulation and comfortable with the lysine manufacturer. As can be seen in Fig. 3 it is important, however, to note that tablet thickness can vary with no change in weight due to either difference in the density of the granulation, the pressure applied to the tablets or the speed of tablet compression. Tablet thickness is important in reproducing tablets identical in appearance but also to ensure that every production lot will fit in selected packaging components. If the tablets are thicker than specified, a given number may no longer be contained in the volume of a given size bottle. Tablet thickness also becomes an important characteristic when counting tablets using filling equipment. All this, fortunately, is not important to consumer of lysine that he or she purchases from the shelf.
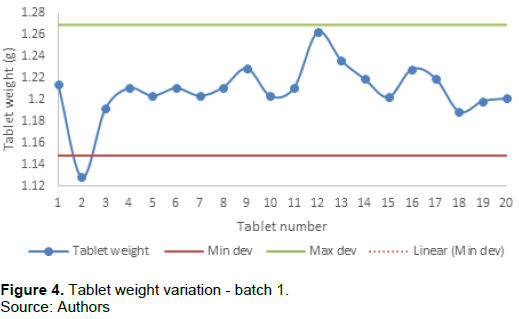
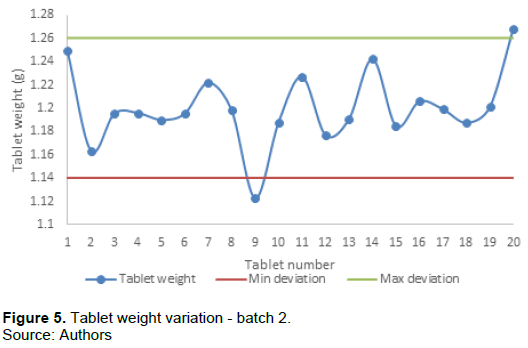
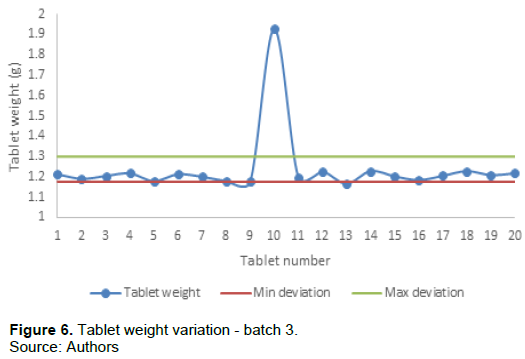
Weight variation of tablets
Uniformity of weight is an in-process test parameter which ensures consistency of dosage units during compression of tablets. In the present study 3 batches of 20 L-lysine tablets were weighed and all appeared to have passed the test, Figures 4 to 6 respectively. The average tablet weight for batch 1, 2 and 3 was 1.2086 ± 0.006 mm, 1.2002 ± 0.008 mm and 1.2381 ± 0.005 mm, respectively. In other words, almost all tablets were within the acceptable range of ± 5% of the average weight, with the exception of 1 tablet from the first sample, Figure 4 and 2 tablets from the second sample, Figure 5 and 1 tablet from the third sample, and Figure 6 indicated in red. However, not more than 2 tablets had weights outside the deviation range for each sample. It can be concluded that tablets were of the same weight. In essence, tablet weight is mainly affected by factors such as tooling of the compression machine, head pressure, machine speed and flow properties of the powder during production of any tablets. Inconsistent powder or granulate density and particle size distribution are common sources of weight variation during compression.
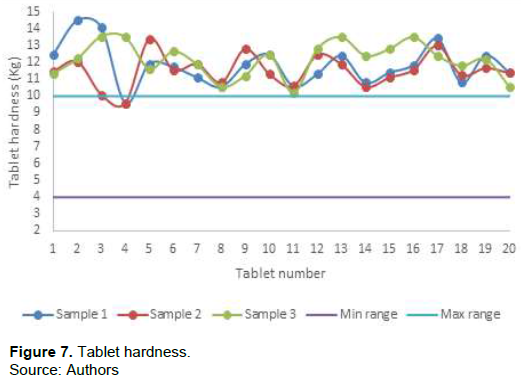
Tablet hardness
The results of measurement of tablet hardness are depicted in Figure 7. Normal tablet hardness ranges from 4 kg to 6kg. One kg is equal 10 Newton. Only one tablet from sample 1 and one tablet from sample 2 had hardness within the range 4 kg to 10 kg. The rest of the tablets from all three samples had hardness greater than 10 kg, with averages 11.9 ± 1.2 kg, 11.6 kg ± 1.0 and 11,7 ± 1.2 kg, respectively for the samples. Tablet hardness testers measure the degree of force required to break a tablet across the diameter. Hardness relates to both tablet disintegration and drug dissolution. The strength of tablets predicts the resistance of tablets to breakage under conditions of storage, transportation and handling before use. In other words, tablet hardness tests provide a meaningful picture as to the amount of force required to fracture the solid-dose tablet. If tablets are too hard, they may not disintegrate within the required period of time which is why disintegrants are added as excipients in some formulation. Disintegrants are substances or a mixture of substances incorporated to the drug formulations, which assist dispersion or breakup of tablets and contents of capsules into smaller fragments for rapid dissolution (Rawat et al., 2014). The L-lysine tablets studied appeared to have no form of disintegrant.
Tablet disintegration
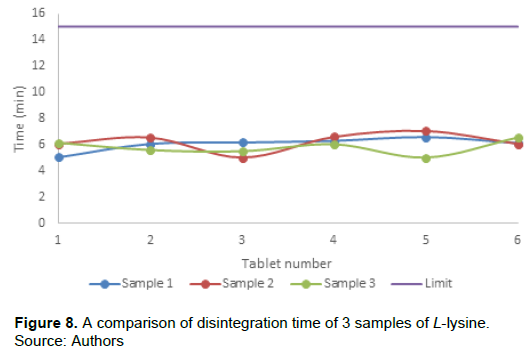
From the results obtained the average disintegration time of the L-lysine tablets were 6.04 ± 0.61 min, 6.22 ± 0.53 min, and 5.81 ± 0.72 min for sample 1, sample 2 and sample 3 respectively. They appeared to be no significant difference among the batches (Figure 8). All tablets disintegrated within the 15 min limit for uncoated immediate release tablets. What this meant was that the purchased tablets were expected to break and release the powder containing the lysine in the stomach without any delay or difficulties.
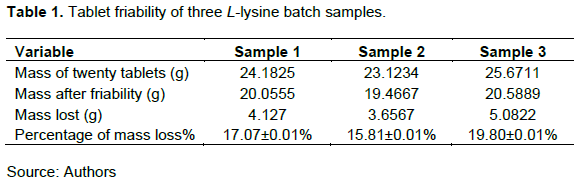
Tablet friability
Friability is also known as the attrition resistance method, imitates the kind of forces (sliding and collision) to which the tablet will be subjected during handling. In such situations, tablets tend to chip and cap ultimately forming crumbles. Failing friability test suggests that tablets may be prone to breaking, chipping and capping during any form of locomotion such as transportation, packing and moving. This may lead to loss of tablet content and also affect its appearance. Table 1 shows results for friability test for 3 batches that were tested. Percentage weight loss from the three samples was 17.07, 15.81 and 19.80% respectively. Weight loss was more than the 1% limit, and therefore the tablets failed friability test. Friability is also known as the attrition resistance method, imitates the kind of forces (sliding and collision) to which the tablet will be subjected during handling. In such situations, tablets tend to chip and cap ultimately forming crumbles. Failing friability test suggests that tablets may be prone to breaking, chipping, and capping during any form of locomotion such as transportation, packing, and moving. This may lead to loss of tablet content and also affect its appearance. It is said that conventional compressed tablets that lose less than 0.5 to 1% of weight are considered acceptable. L-lysine tablets studied appeared to have failed the test. There are several reasons that could explain the failure of the lysine tablets. These include poor punches that could have been used by the manufacturer; internal factors like moisture content of the tablet granules. Moisture at low and acceptable levels is said to act as a binder (Saleem et al., 2014). This may lead to loss in the quantity of the active ingredient as indicated in label.
Quantity of L-lysine in tablets
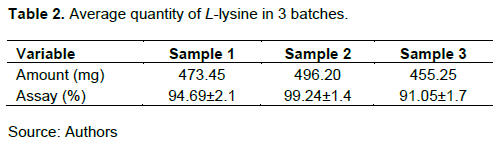
The labels of the different batches of L-lysine indicated that there was 500 mg of L-lysine which appeared not to be so as shown in Table 2. The US Pharmacopoeia specifies that L-lysine tablets should contain not less than 95% and not more than 105% of the labelled amount. The results of the study showed that only one sample had amount of L-lysine within the acceptable range. The other two samples had amount of lysine outside the acceptable range. It would, therefore, be reasonable to conclude that there was no consistency in the quantity of L-lysine in the tablets, a fact unknown to the consumer. This raises an alarm that the tablets may not contain the quantity of L-lysine on the label claim.
L-lysine release profile from tablets
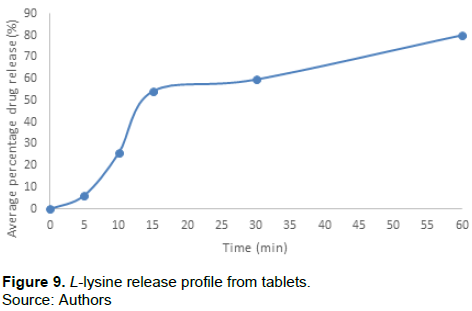
The average percentage drug release reached 80.08% at 60 min as shown in Figure 9. For immediate release dosage units, tablets must release at least 75% of the drug within 45 min. Tablets sampled released just about 70% of the contained L-lysine by 45 min, which is less than the limit. It would be reasonable to assume that L-lysine tablets studied were manufactured for immediate release. Immediate release tablets are invented to disintegrate and release their dosage form with no special rate controlling features, such as special coatings and other techniques. Immediate release tablets are those which disintegrate swiftly and get dissolved to release the active ingredient. Therefore, the oral bioavailability of the ingredient is dependent on disintegration, dissolution and various physiological factors. An immediate release dosage form helps a manufacturer to diversify market and simultaneously offering patients a convenient dosage form or dosage regimen (Verma et al., 2014).
Capsules
Powder weight variation of capsules
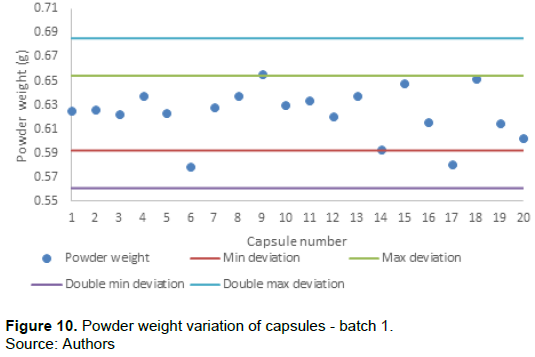
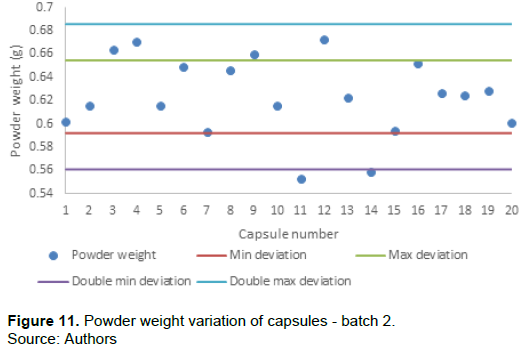
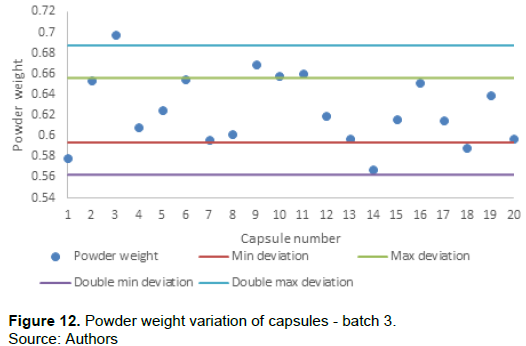
Dosage units pass the weight variation test if not more than two dosage units fall outside the percentage limit and if no dosage unit differs by more than two times the percentage limit. The average weights of the L-lysine powder obtained from the hard uncoated capsules of the three batch samples were 0.6233 ± 0.004g, 0.6234 ± 0.005g and 0.6248 ± 0.008g respectively. As can be seen in Figure 10 only two capsule powder weights of batch 1 were outside the 5% deviation but none were beyond the 10% deviation range. The batch passed the weight variation test. The second and the third batch samples, Figures 11 and 12 both failed the weight variation test. For both batch samples more than 2 capsule weights were outside the 5% deviation range and at least one capsule weight was outside the 10% deviation range. The conclusion is that L-lysine capsules from three batches failed weight variation test. The capsules powder had inconsistent weights unlike the batches of tablets. Tablets have a longer shelf life and come in a variety of forms. They can also accommodate a higher dose of an active ingredient than a capsule. They tend to be slower acting and, in some cases, may disintegrate unevenly in your body. Capsules act quickly and most, if not all, of the drug are absorbed.
Capsule disintegration
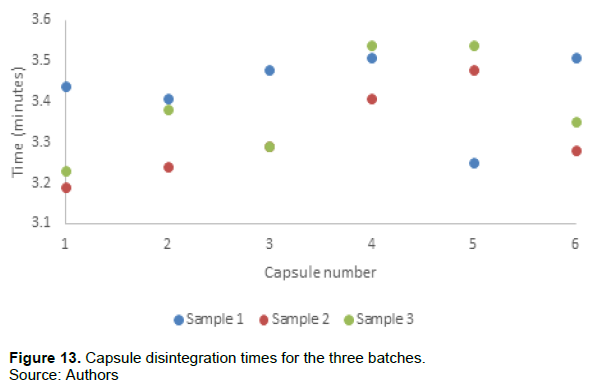
The average capsule disintegration times for the three samples were 3.43 ± 0.38 min, 3.32 ± 0.67 min and 3.39 ± 0.56 min for sample 1, sample 2 and 3 sample respectively (Figure 13). All capsules disintegrated within the 15 min’ limit for uncoated hard gelatin capsules. Therefore, the capsules’ hard shells were expected to dissolve and release the L-lysine in the stomach without any delay or difficulties. Disintegration time of capsule was much shorter compared to the tablet. This was, however, to be expected according to what has been reported in other studies (Melia and Davis, 1989).
Quantity of L-lysine in capsules
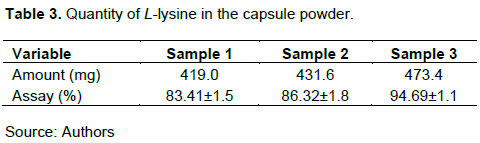
Unfortunately as shown in Table 3 the amount of L-lysine in the capsule powder was lower than what was written on the container label and in the package insert of the capsule product. The average amount of lysine in the capsules was 83.41, 86.32, and 94.69% for the three batch samples, respectively. All these amounts were below the general acceptable range of 95 to 105% as stated in the USP. There are several reasons that can be suggested as to why there were lower L-lysine quantities which agreed with variations in powder weight (Figure 11). One of the reasons for lower quantities could be the mixing methods used during manufacturing. Improper handling of powder materials during manufacture may cause powder segregation leading to non-uniformity of dosage units. Mixing particles that differ in size, shape and density; poor flow properties of powder materials in hoppers and subjecting mixed particles to excessive vibrations are some of the causes of segregation. The other reason for lower quantities could be the type of equipment used was not good at mixing the powder to ensure homogeneity. This obviously has therapeutic consequences given the fact that L-lysine is promoted as a nutritional supplement that supports good health and that it may assist to reduce the recurrence, severity and healing time of herpes simplex viral virus infections (cold sores). If each capsule is said to contain 500mg, under normal regulatory specifications, it then assumed that anything below that amount would be sub-therapeutic. The product would obviously not be given marketing authorization.
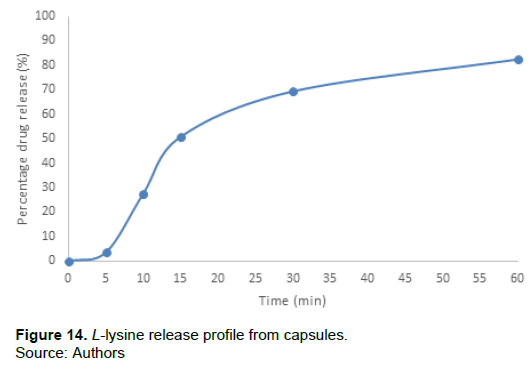
L-lysine release profile from capsules
Figure 14 depicts the drug release profile from capsules. The average percentage drug release reached 82.46% at 60 min. Just over 75% of drug had been released by 45 min. Therefore, no problems with drug release are to be expected from the capsules in the gastro-intestinal tract in the body. The test is the most important under controlled condition, mimicking the conditions in human stomach. With this test, the bio-availability and factors affecting it can be determined.
CONCLUSION
In summary, there are inconsistences in the characteristics of the L-lysine products and their pharmaceutical quality may not be guaranteed. From the result obtained in general, it would appear that clients would best be advised to purchase L-lysine in capsular formulation than tablets. However, from the consumers’ point of view, the price would obviously be the main determinant of the purchase of the L-lysine products. From the manufacturer’s side, there are many reasons to choose between formulating L-lysine into a tablet or a capsule. For example, tablets are cheaper to manufacture, tablets are more stable and typically have a longer shelf life than capsules. In comparison, capsules are less likely to have an unpleasant taste or odour, capsules disintegrate quickly and have a higher bioavailability which means that more of the drug is likely to enter into the bloodstream. Overall, whether L-lysine is marketed as either tablets or capsules, if good and acceptable pharmaceutical quality standards are met, this assures that the contained active ingredient would be delivered to the body and that the intended effect would be achieved. This would ultimately give the consumer confidence that they are receiving value for their money. The use of nutritional supplements is increasing annually and is becoming a big market. More investigations on other marketed L-lysine products are suggested. Accordingly, a relook of their quality assurance procedures and labelling by whoever gives the market authorization may be necessary.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors acknowledge the University of Limpopo for resources and facilities.
REFERENCES
|
Banach M, Patti AM, Giglio RV, Cicero AFG, Bajraktari G, Brucker E, Descamps O, Djuric D, Ezhov M, Fras Z, von Haehling S (2018). The role of nutraceuticals in statin intolerant patients. Journal of the America College of Cardiology 72(1):96-118 |
|
|
Food and Drug Administration (FDA) (2016). Labeling and Nutrition. Food and Drug Administration, US Department of Health and Human Services. 5 October 2016. Retrieved 21 Nov 2020 |
|
|
Gupta S, Yadav AK (2022). Emerging trend of chondroitin sulfate in nanoparticles preparation, targeting, and pharmaceutical applications. Polysaccharide Nanoparticles pp. 65-90. |
|
|
Kaplan S (2019). Supplement makers touting cures for Alzheimer's and other diseases get FDA warning. New York Times, 11 February 2019. Retrieved 21 Nov 2020 |
|
|
Lockwood GB (2015). Quality evaluation and safety of commercially available nutraceutical and formulated products. In: Nutraceutical and Functional Processing Technology (pp. 113-150). |
|
|
Melia CD, Davis SS (1989). Mechanisms of drug release from tablets and capsules. I: disintegration. Alimentary Pharmacology and Therapeutics 3(3):223-232. |
|
|
Rawat S, Derle DV, Fukte SR, Shinde PR, Parve BS (2014). Superdisintegrants: an overview. World Journal of Pharmacy and Pharmaceutical Sciences 3(5):263-278. |
|
|
Russell AS, Aghazadeh-Habash, A, Jamali F (2002). Active ingredient consistency of commercially available glucosamine sulfate products. The Journal of Rheumatology 29(11):2407-2409. |
|
|
Sarris J, Murphy J, Mischoulon D, Papakostas GI, Fava M, Berk M, Ng CH (2016). Adjunctive nutraceuticals for depression: A systematic review and meta-nalysis. American Journal of Psychiatry 173(6):575-587. |
|
|
Verma K, Sharma PK, Dudhe R, Patro ASK (2014). Formulation, design and development of Mifepristone immediate release tablet. International Journal of Pharma Sciences and Research 5(11):760-769. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


