Full Length Research Paper

ABSTRACT
The prescribing of medicines is critical in the treatment of diseases in general practice. Inappropriate prescribing can negatively influence the goals of treatment, which makes the assessment of the patterns of prescriptions essential. The objective of this study was to assess the medicines prescribing pattern in health facilities in the Northern Ghana, a developing economy in Africa, using the prescribing indicators recommended by the WHO and International Network of Rational Use of Drugs (WHO/INRUD). A prospective observational survey was used to collect data from 600 prescriptions between February and July of 2017 using a specially designed check list. Fifty randomly selected prescriptions each were collected from 12 facilities within the metropolis. Participating facilities were included in the study by systematic sampling that was purposive, convenience and random. Data was analysed in Statistical Package for Social Science (SPSS) version 18. The average number of medicines prescribed was (3.9). Antibiotics and injections were prescribed at a rate of 55 and 14%, respectively; while prescribing by generic name was 53%. Prescribing from the Essential Medicines List (EML) stood at 96%. Public facilities had better indicators compared with private: average number of drugs (3.5 vs 4.3, p < 0.001); percentage injections (13 vs 25, p = 0.002); percentage generic names (62 vs 45, p = 0.003). Percentage antibiotics (54 vs 56) and percentage from the EML (97 vs 94) were not different for public and private facilities. There is inappropriate prescription pattern of medicines, such as polypharmacy and over prescribing of antibiotics and injections. Prescribing by generic name although high was still lower than recommended.
Key words: Patterns prescription, medicines, indicators, adherence, overprescribing.
INTRODUCTION
Medicines are vital in healthcare delivery but for most people in the world, medicines are still unavailable, unaffordable, and unsafe (Ofori-Asenso and Agyeman, 2016; Oguanobi, 2018). It is estimated that around 50% of all medicines are prescribed, dispensed or sold and used inappropriately (WHO, 2002). Inappropriate and irrational use of medicines is wasteful and harmful to both the individual and the population at large. Adverse events following the inappropriate use of medicines are significant cause of morbidity and mortality (Assiri et al., 2016). It has been reported that 5 to 6% of inpatient admissions in the United States of America (USA) are drug related of which adverse drug events (ADEs) alone account for 10% (Krahenbuhl-Melcher et al., 2007).
It is estimated that, as high as 25 to 70% of the entire health budgets of developing countries are spent on medicines, despite the limited budgetary allocations to health in these countries, whereas, about 10% of health expenditure in the developed economies is spent on medicines (Dielman, 2017). In appropriate prescribing and use of antimicrobial agents have led to a swift increase in antibiotic resistance globally, leading to increased significant morbidity and mortality (Li and Webster, 2018). Studies indicate that, the cost of antibiotic resistance per annum is in the range of US$4-5 billion in the USA and $1.01billion in Europe (Washington, 1998; EU, 2017).
In Africa, the excessive use of antibiotics and injections are particularly more problematic in private than public health facilities (Ofori-Asenso and Agyeman, 2015). The indiscriminate use of antibiotics for the treatment of upper respiratory tract infection has been found to be in ascendency in Ghana (Ahiabu et al., 2015). This inevitably is a major source of financial drain to the already overburden National Health Insurance Scheme and more importantly, the reported antibiotic resistance in the country (Ahiabu et al., 2015).
The World Health Organisation (WHO) defines rational use of medicines as: ‘patients receiving medications appropriate to their clinical needs, in doses that meet their own individual requirements, for an adequate period, and at the lowest cost to them and their community’ (WHO, 2001). Unrestricted access to and irrational use of medicines is abundant in many developing countries (Siddiq et al., 2002). The selection and rational use of medicines are accepted as key principles of health service quality management in both the public and private sectors (IRUM/GHS, 2008).
This study attempted to measure the performance of health facilities in the Tamale Metropolis against the WHO/INRUD medicine prescribing indicators as a bench mark.
MATERIALS AND METHODS
Study area and site
The study was conducted in the Tamale Metropolis, which is one of the 26 administrative and political District Assemblies in Northern Region of Ghana. The metropolis has a total population of 223,252 comprising of 112,143 (50.2%) females according to the 2010 population and housing census by the Ghana Statistical Service. With 80.8% of the population living in urban areas, the average life expectancy is estimated at 63.4 years (World Life Expectancy, 2018) and a per capita GDP of 1708 (Trading Economics, 2018).
The metropolis has 28 health service facilities and one teaching hospital, the Tamale Teaching Hospital (TTH). The study included the only tertiary health facility, three secondary and primary health facilities in the metropolis. The tertiary health facility was the TTH, which has a bed capacity of 450 and sees over 100, 000 patients a year. It provides all specialist care services to patients referred from other facilities lower facilities in the northern sector of Ghana. It also serves as an institution for training in health related professions.
The secondary health facilities were the Tamale West Hospital (TWH), Tamale Central Hospital (TCH) and the Seventh Day Adventist Hospital (SDAH). With bed capacities of 185, 126 and 100 each, these facilities provide reproductive and child health, laboratory, and pharmaceutical care services to outpatients and inpatients within the Tamale metropolis and beyond. They are manned by medical officers and physician assistants who generate prescriptions. The primary health facilities were five private health facilities and three sub district facilities, which offer general Outpatient Department (OPD) services. Prescribers in these facilities are mostly physician assistances, nurses and midwifes. Public facilities are those that are owned by the government and work to serve the general population, while private health facilities are owned by corporate entities and are driven by profits.
Study design, population and sampling
In a prospective observational survey, a total of 600 outpatient prescriptions issued at the selected health facilities between February and July, 2017, were collected as recommended by the WHO (1993). In a systematic manner, 12 health facilities were purposefully selected, to ensure the inclusion of all the categories of health facilities in terms of services provided and ownership. To this end, all facilities in the metropolis were stratified into four as: tertiary, secondary, primary, and also public or private health facilities. From the 12 facilities 50 prescriptions were randomly selected using a computer generated set of random numbers to reach the 600 prescriptions.. The prescriptions were collected at the OPD of the selected facilities till the targeted number was reached in each facility.
Data collection
This was a prescription survey, in which data was collected using a specially designed check list by three trained research assistants. For each prescription issued at the OPD, the WHO/INRUD core prescribing indicators and the ownership of the facility such as private or public were captured. On the day of the research, the research assistants extracted the study information after the dispenser had completed dispensing at the OPD pharmacy or dispensary. The specific data required to measure the prescribing indicators were recorded for each patient encounter and entered directly into an ordinary prescribing indicator form.
Prescribing indicators
The World Health Organization/International Network for Rational Use of Drugs (WHO/INRUD) has set standard prescription indicators that guide the prescribing of medicines (WHO, 1993). The prescribing indicators used in this study were adapted and pretested versions of those recommended by the WHO (1993), and described as follows:
(1) Average number of drugs prescribed per encounter: was calculated by dividing the total number of different drug products prescribed, by the number of encounters surveyed. Fixed dose combined drugs prescribed for one health problem was counted as one. This indicator was used to measure the degree of polypharmacy
(2) Percentage of drugs prescribed by generic name: - calculated by dividing the number of drugs prescribed using generic name by the total number of drugs prescribed, multiplied by 100.
(3) Percentage of encounters with an antibiotic: - obtained by dividing the number of patient encounters in which an antibiotic was prescribed by the total number of encounters surveyed, multiplied by 100.
(4) Percentage of encounters with an injection: - calculated by dividing the number of patient encounters in which an injection was prescribed by the total number of encounters surveyed, multiplied by 100.
(5) Percentage of drugs prescribed from the essential drug list:- calculated by dividing number of drugs prescribed which are in the essential drug list by the total number of drugs prescribed, and multiplied by 100.
Data analysis
Data collected was double entered and verified using the software Epi Info (version 3.5.1 (CDC, Atlanta, Georgia USA), which was designed to include range checks. The data was exported to SPSS (version 18; SPSS Inc., Chicago, Illinois, USA) for analysis. The unpaired t-test was used to compare means for continuous variables and the Chi-square test for differences in proportions for categorical variables. A P-value of <0.05 was considered statistically significant. Generic prescribing and EDL drugs were analysed using recent pharmacological textbooks, the Ghana national standard treatment guidelines and the Ghana Essential Medicine List (EDL).
RESULTS
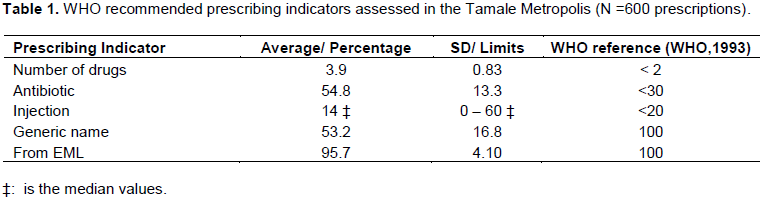
The prescribing indicators measured on the 600 individual prescriptions gathered from all the facilities are summarised in Table 1. The comparison of how the indicators performed between public and private health farcicalities is presented in Table 2.

Average number of drugs per encounter
The overall average (standard deviation) number of drugs per encounter in all twelve health facilities (HFs) surveyed was 3.9 (0.83). Among the individual HFs, the highest average number of drugs prescribed was observed in a private clinic with an average (standard deviation) of 5.8 (1.20) drugs per encounter, whereas the least average of 2.9 (1.00) was observed in a public health centre. Comparing the averages of the public and private facility prescriptions indicated that, the average number of medicines in the private health facilities (4.3) was more and significantly different from that prescribed in the public health facilities (3.5), P < 0.001 (Table 2).
Percentage encounter with an antibiotic prescribed
The mean (sd) percentage encounter with antibiotic prescribed in the HFs in the metropolis was found to be 54.8% (13.30). The least (34%) was observed in a private health facility whereas the highest (78%) was observed in a public facility. The results indicate that both public and private facilities had high utilization of antibiotics; 56 and 54% respectively, and there were no significant difference in the proportions between public and private facilities (P = 0.330).
Percentage of injections prescribed
The overall median injection prescribed in the facilities within the metropolis was 14%. Over 50% of the health facilities had injections prescribed at above 10%. The highest percentage injection prescribed was 60%, with only one facility recording no injection prescribed. A chi-square analysis returned a significant difference between percentage of injections between public and private health facilities. The public health facilities had a significantly lower proportion of 13% compared to the 25% in the private facilities (P < 0.001).
Percentage prescriptions with generic name
Over all, there was 53% prescription written by generic names in the metropolis (Table 1). The highest prescribing by generic name in a facility was 84%, while over 30% (4/12) of all the facilities prescribed drugs by generic names at a rate lower than 50%. As low as 18% of prescription by generic name was recorded in a facility. A comparison between public and private health facilities indicated that public health facilities had a statistically significant and higher overall prescribing by generic names than private facilities (61.7 vs. 44.8%; P < 0.001) (Table 2).
Percentage prescription from the essential medicines list
Overall, there was a mean (sd) of 95.7% (4.10) of prescribing from the EML in the metropolis (Table 1). All the health facilities, except one, issued over 90% of prescription from the EML. Only one facility had all (100%) of its prescriptions coming from the EML, with 84.6% being the lowest rate of prescribing from the EML in a facility. There was no difference between public and private health facilities regarding percentage prescribing from the EML (P = 0.053) (Table 2).

DISCUSSION
CONCLUSION
Prescribing within the Tamale metropolis was irrational, characterised by over-prescribing of medicines (polypharmacy), higher prescribing of antibiotics, and lower adherence with generic prescribing in all the health facilities of the metropolis. For all of these indicators mentioned, the private facilities performed poorly compared with the public one. Prescribing from the essential medicines list was overall encouraging, although still below the recommended 100%. Only prescribing of injectable forms met the WHO recommendations.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors are grateful to Dr Stephen Apanga (School of Medicine and Health Sciences, University for Development Studies, Tamale Ghana) and Dr Martin Adokiya (School of Allied Health Sciences, University for Development Studies, Tamale) for their immense support in the formulation of the study. The authors also thank the Northern Regional Health Directorate, in particular Dr James Sarkodie, who facilitated access to the health facilities included in the study.
REFERENCES
|
Afriyie DK, Tetteh R (2014). A description of the pattern of rational drug use in Ghana Police Hospital. Internal Journal of Pharmacy and Pharmacology 3(1):143-148. |
|
|
Ahiabu MA, Tersbøl BP, Biritwum R, Bygbjerg IC, Magnussen P (2015). A retrospective audit of antibiotic prescriptions in primary healthcare facilities in Eastern Region, Ghana. Health Policy and Planning 31(2):250-258. |
|
|
Akhtar M, Vohora D, Pillai K, Dubey K, Roy M, Najmi A, Khanam R (2012). Drugs prescribing practices in paediatric department of a north Indian university teaching hospital. Asian Journal of Pharmaceutical and Clinical Research 5(1):146-149. |
|
|
Apanga S, Chirawurah D, Kudiabor C, Adda J, Adoesom J A, Punguyire D (2014). Evaluation of drug prescribing patterns under the national health insurance Scheme in rural Ghana. International Journal of Pharmaceutical Sciences and Research 5(6):2193-2198. |
|
|
Assiri GA, Grant L, Aljadhey H, Sheik A (2016). Investigating the epidemiology of medication errors and error-related adverse drug events (ADEs) in primary care, ambulatory care and home settings: A Systematic review protocol; British Medical Journal Open. |
|
|
Atif M, Sarwar MR, Azeem M, Umer D, Rauf A, Rasool A, Ahsan M, Scahill S (2016). Assessment of WHO/INRUD core drug use indicators in two tertiary care hospitals of Bahawalpur, Punjab, Pakistan. Journal of Pharmaceutical Policy and Practice 9(1):27. |
|
|
Boonstra E, Lindback M, Khulumani P, Ngome E, Fugelli P (2002). Adherence to treatment guidelines in primary healthcare facilities in Bostwana. Tropical Medicine International Health 7(2):178-186. |
|
|
Bossu WK, Ofori-Adjei D (2000). An audit of prescribing practices in healthcare facilities of the Wassa West district of Ghana. West Africa Journal of Medicine 19(4):298-303. |
|
|
Desalegan AA (2013). Assessment of drug use pattern using WHO prescribing indicators at Hawassa university teaching and referral hospital, south Ethiopia: a cross-sectional study BMC Health Services Research 13:170. |
|
|
Desta Z, Abula T, Gebre-Yohannes A, Worku A (2002). Drug prescribing patterns for outpatients in three hospitals in north-west Ethiopia. Ethiopian Journal of Health Development 6(2):183-189. |
|
|
Dielman JL (2017). Future and potential spending on health 2015-40: development assistance for health, and government, prepaid private, and out-of-pocket health spending in 184 countries Global. Lancet 389(10083):2005-2030. |
|
|
Dong L, Yan H, Wang D (2010). Drug prescribing indicators in village health clinics across 10 Provinces of Western China. Family Practice 28:63-67. |
|
|
El Mahalli AA (2012). WHO/INRUD drug prescribing indicators at primary health care centers in Eastern province, Saudi Arabia. Eastern Mediterranean Health Journal 18(11):1091-1096. |
|
|
Essential Medicines List (EML) (2010). Ghana Essential Medicines List, 6th Edition. |
|
|
EU (2017). EU Action on Antimicrobial Resistance |
|
|
GNDP (2002). A Baseline Survey of the Pharmaceutical Sector. Ghana National Drug Program, Accra. |
|
|
IRUM (2008). Institutionalizing rational use of medicines in Ghana. Accra: Multiple Impression 34. |
|
|
Kohl H, Shank WH (2007). Increasing Generic drug use in medicare Part D: The role of government. Journal of the American Geriatric Society 55:1106-1109. |
|
|
Krahenbuhl-Melcher A, Schlienger R, Lampert M, Haschke M, Drewe J, Krahenbuhl S (2007). Drug related problems in hospitals: A review of a recent literature. Drug Safety 30:379-407. |
|
|
Li B, Webster TJ (2018). Bacteria Antibiotic Resistance: New Challenges and Opportunities for Implant-Associated Orthopaedic Infections. Journal of Orthopaedic Research 36(1):22-32. |
|
|
Maiga D, Diawara A, Maiga MD (2006). Evaluation of rational prescribing and dispensing of medicines in Mali. Revue d'epidemiologie et de sante publique 54(6):497-505. |
|
|
Ofori-Adjei D (1993). Report on Tanzanian field test. INRUD News 3(1):9. In How to investigate drug use in health facilities. WHO: Geneva; 1993. 74(WHO/DAP/93.1) |
|
|
Ofori-Asenso R, Agyeman AA (2015). A review of injection and antibiotic use at primary healthcare (Public and Private) centers in Africa. Journal of Pharmacy and Bioallied Sciences 7(3):175-180. |
|
|
Ofori-Asenso R, Agyeman AA (2016). Irrational use of medicines-a summary of key concepts. Pharmacy 4(4):35. |
|
|
Ofori-Asenso R., Brhlikova P, Pollock AM (2016). Prescribing indicators at primary healthcare centers within the WHO. African region: A systematic analysis (1995-2015) BMC Public Health, 16:724. |
|
|
Oguanobi HI (2018). Broadening the conversation on the TRIPS agreement: Access to medicines includes addressing access to medical devices. The Journal of World Intellectual Property 21(1-2):70-87. |
|
|
Quick JD, Hogerzeil HV, Velasquez G, Rago L (2002). Twenty-five years of essential medicines. Bulletin of World Health Organisation 80:913-914. |
|
|
Ruwan K, Prasad C, Rausinghe B (2006). Pattern of private sector drug prescription in Galle: A descriptive cross-sectional study. Galle Medical Journal 11(1):64-68. |
|
|
Singh S, Dadhich AP, Agarwal AK (2003). A study of prescribing practices in a tertiary care hospital using WHO core indicators. Asia Pacific Journal of Pharmacology 16(1):9-14. |
|
|
Trading Economics (2018). |
|
|
Uzoma SON, Lungu A, Ombaka E (1995). Drug use studies in church facilities in Africa. INRUD News 5:20 |
|
|
Washington DC (1998). Institute of medicine. Microbial threats to health: emergence, detection and response; National Academies press. |
|
|
Wiffen PJ, Mayon WRT (2001) Encouraging good antimicrobial prescribing practice: A review of antibiotic prescribing policies used in the South East Region of England. BMC Public Health. 1(4). |
|
|
World Health Organization (WHO) (1993). How to Investigate Drug use in health facilities: Selected Drug Use indicators EDM, Research Series No. 007, WHO/DAP/93.1. |
|
|
World Health Organization (WHO) (1998). Guide to Drug Financing Mechanisms. |
|
|
World Health Organization (WHO) (2001). Global Strategy for containment of Antimicrobial Resistance. |
|
|
World Health Organization (WHO) (2002). Promoting rational use of medicines: core components - WHO Policy Perspectives on Medicines. |
|
|
World Life Expectancy (2018). |
|
|
Wiffen PJ, Mayon White RT (2001). Encouraging good antimicrobial prescribing practice: A review of antibiotic prescribing policies used in the South East Region of England. BMC Public Health 1(4). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


