Full Length Research Paper

ABSTRACT
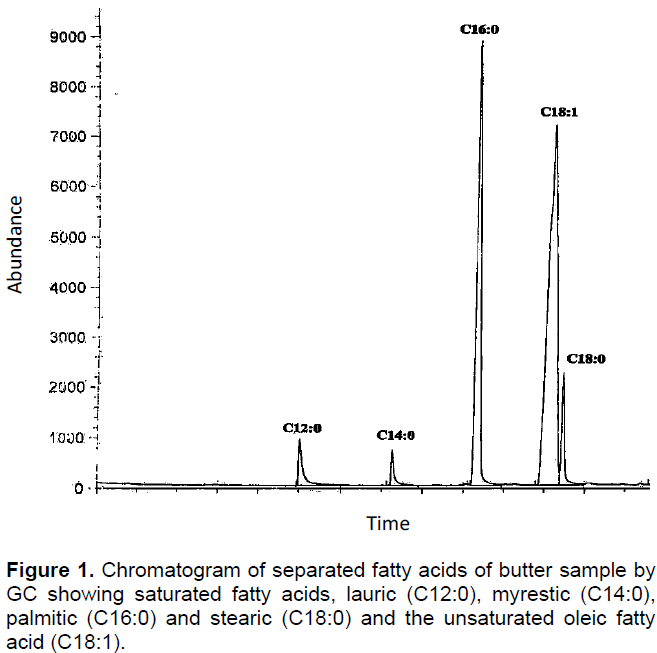
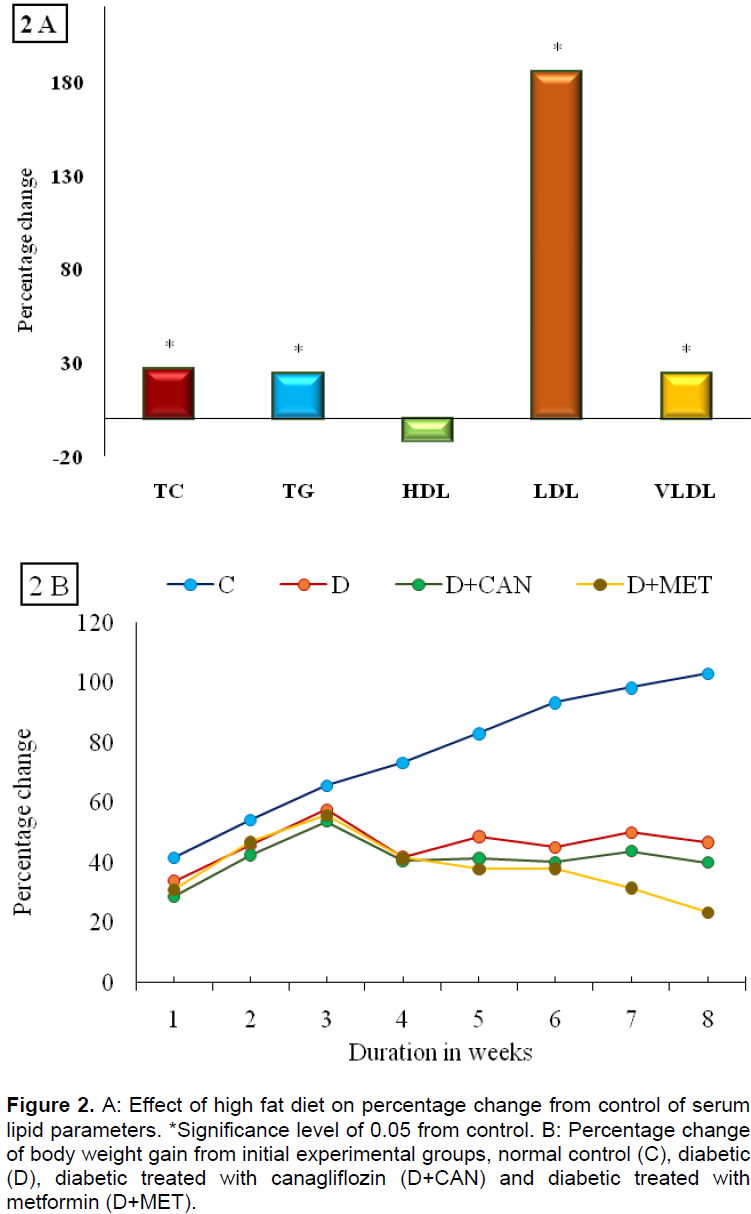
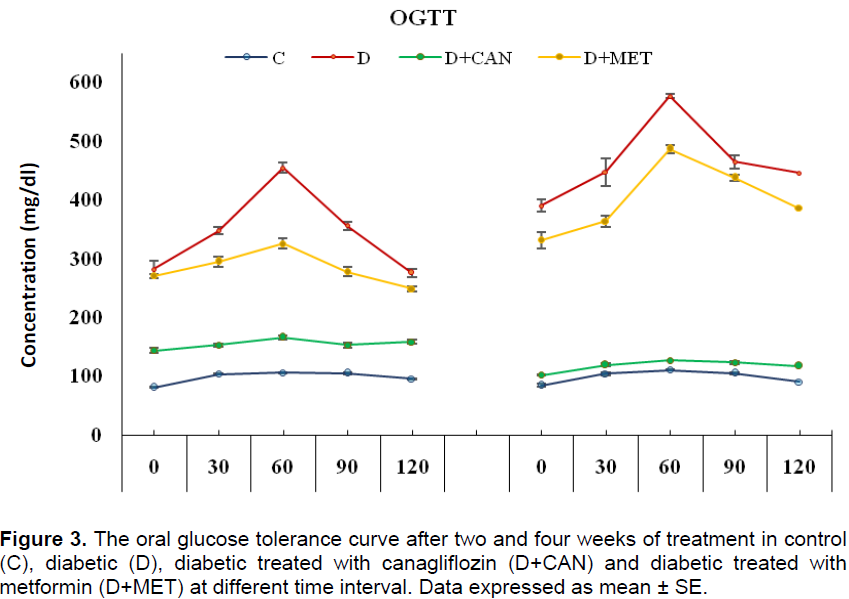
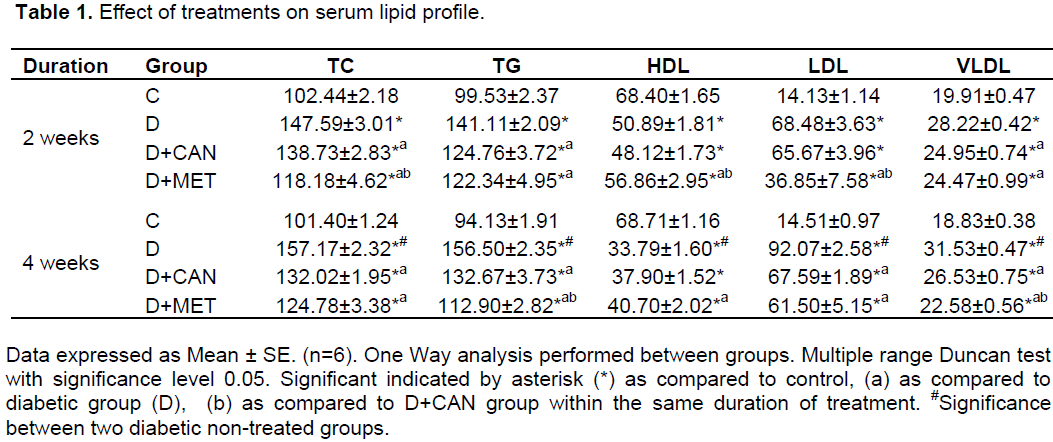
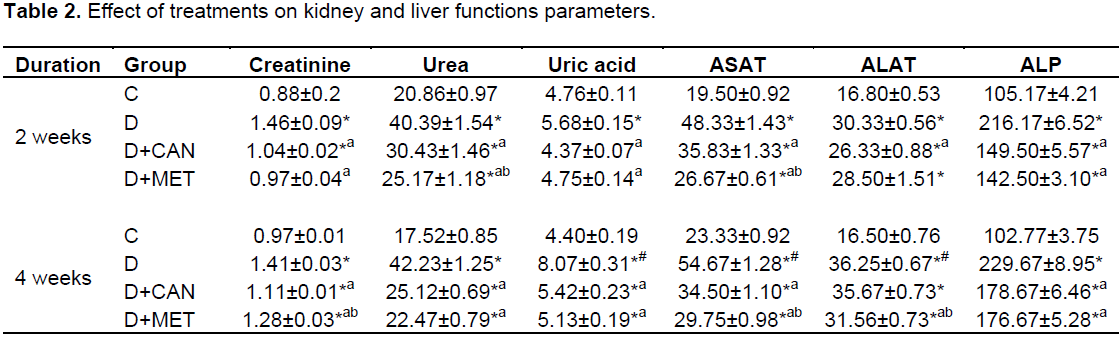
This study aimed to investigate the effect of canagliflozin (CAN) or metformin (MET) on investigated biochemical parameters in obese diabetic rat model. Obesity induced by melted butter administration and hyperlipidemic rats were subjected to streptozotocin (STZ; 35 mg/kg i.p) to develop the diabetic model (D). Animals were grouped as control (C), D none treated and diabetic treated with CAN (10 mg/kg) or MET (100 mg/kg) for two and four weeks. Both treated groups showed significant reduction in body weight and CAN group exhibited significant decrease in oral glucose tolerance test (OGTT) as compared to D or MET group in the experimental periods. Both drugs showed hypolipidemic activity by reducing total cholesterol (TC), triglyceride (TG), low-density lipoprotein (LDL) and very low-density lipoprotein (VLDL) and elevating high-density lipoprotein (HDL) as compared to D group values in the two intervals with advantage in MET effect. Both treatments achieved significant reduction in the diabetic elevated serum values for liver and kidney functions. These results indicate that butter high-fat diet and low dose of STZ makes normal male adult rat associated with hyperlipidemia, glucose intolerance and disturbed liver and kidney functions. Treatment by either CAN or MET resisted the metabolism disturbance of the butter high fat diet/STZ -induced obese type 2 diabetes mellitus rats.
Key words: Canagliflozin, metformin, obese diabetic rats, glucose intolerance, biochemical parameters.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONFLICT OF INTERESTS
ACKNOWLEDGEMENT
REFERENCES
|
Afzal M, Kazmi I, Gupta G, Rahman M, Kimothi V, Anwar F (2012). Preventive effect of Metformin against N-nitrosodiethylamine-initiated hepatocellular carcinoma in rats. Saudi Pharm. J. 20(4):365-370. |
|
|
Badran M, Laher I (2012). Type II Diabetes Mellitus in Arabic-Speaking Countries. Int. J. Endocrinol. 11 p. |
|
|
Bansal P, Paul P, Mudgal J, Nayak PG, Pannakal ST, Priyadarsini KI, Unnikrishnan MK (2012). Antidiabetic, antihyperlipidemic and antioxidant effects of the flavonoid rich fraction of Pileamicrophylla (L.) in high fat diet/streptozotocin-induced diabetes in mice. Exp. Toxicol. Pathol. 64(6):651-658. |
|
|
Bhandari U, Chaudhari HS, Khanna G, Najmi AK (2013). Antidiabetic effects of Embeliaribes extract in high fat diet and low dose streptozotocin-induced type 2 diabetic rats. Front Life Sci. 7(3-4):186-196. |
|
|
Chino Y, Samukawa Y, Sakai S, Nakai Y, Yamaguchi J, Nakanishi T, Tamai I (2014). SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule byincreased glycosuria. Biopharm. Drug Dispos. 35(7):391-404. |
|
|
de la Rosa LC, Vrenken TE, Buist-Homan M, Faber KN, Moshage H (2015). Metformin protects primary rat hepatocytes against oxidative stress-induced apoptosis. Pharm. Res. Perspect. 3(2):e00125. |
|
|
Eleazu CO, Eleazu KC, Chukwumam S, Essien UN (2013). Review of the mechanism of cell death resulting from streptozotocin challenge in experimental animals, its practical use and potential risk to humans. J. Diabetes Metab. Disord. 12(1):60. |
|
|
Friedewald WT, Levy RI, Fredrickson DS (1972). Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the ultracentrifuge. Clin. Chem. 18:499-502. |
|
|
Geerling JJ, Boon MR, van der Zon GC, van den Berg SA, van den Hoek AM, Lombès M, Princen HM, Havekes LM, Rensen PC, Guigas B (2014). Metformin lowers plasma triglycerides by promoting VLDL-triglyceride clearance by brown adipose tissue in mice. Diabetes 63(3):880-91. |
|
|
Guidance for Industry and Reviewers (2002). Estimating the safe starting dose in clinical trials for therapeutics in adult healthy volunteers. Food Drug Adm. pp. 1-26. |
|
|
Halimi S, Vergès B (2014). Adverse effects and safety of SGLT-2 inhibitors. Diabetes Metab. 40(6-1):28-34. |
|
|
Inagaki N, Kondo K, Yoshinari T, Kuki H (2015). Efficacy and safety of canagliflozin alone or as add-on to other oral antihyperglycemic drugs in Japanese patients with type 2 diabetes: A 52-week open-label study. J. Diabetes Invest. 6(2):210-218. |
|
|
Ji L, Han P, Liu Y, Yang G, Dieu Van NK, Vijapurkar U, Qiu R, Meininger G (2015). Canagliflozin in Asian patients with type 2 diabetes on metformin alone or metformin in combination with sulphonylurea. Diabetes Obes. Metab. 17(1):23-31. |
|
|
Komala M, Panchapakesan U, Pollock C, Mather A (2013). Sodium glucose cotransporter 2 and the diabetic kidney. Curr. Opin. Nephrol. Hypertens 22(1):113-119. |
|
|
Ledoux M, Chardigny JM, Darbois M, Soustre Y, Sébédio JL, Laloux L (2005). Fatty acid composition of French butters, with special emphasis on conjugated linoleic acid (CLA) isomers. J. Food Compost. Anal. 18:409-425. |
|
|
Liang Y, Arakawa K, Ueta K, Matsushita Y, Kuriyama C, Martin T, Du F, Liu Y, Xu J, Conway B, Conway J, Polidori D, Ways K, Demarest K (2012). Effect of canagliflozin on renal threshold for glucose, glycemia, and body weight in normal and diabetic animal models. PLoS One 7(2):e30555. |
|
|
Lin J, Yang R, Tarr PT, Wu PH, Handschin C, Li S, Yang W, Pei L, Uldry M, Tontonoz P, Newgard CB, Spiegelman BM (2005). Hyperlipidemic effects of dietary saturated fats mediated through PGC-1beta coactivation of SREBP. Cell 120(2):261-273. |
|
|
Lobato NS, Filgueiram FP, Hagihara GN, Akamine EH, Pariz JR, Tostes RC, Carvalho MH, Fortes ZB (2012). Improvement of metabolic parameters and vascular function by metformin in obese non-diabetic rats. Life Sci. 90(5-6):228-235. |
|
|
Luis-Rodríguez D, Martínez-Castelao A, Górriz JL, De-Álvaro F, Navarro-González JF (2012). Pathophysiological role and therapeutic implications of inflammation in diabetic nephropathy. World J. Diabetes 3(1):7-18. |
|
|
Marchetti P, Del Guerra S, Marselli L, Lupi R, Masini M, Pollera M, Bugliani M, Boggi U, Vistoli F, Mosca F, Del Prato S (2004). Pancreatic islets from type 2 diabetic patients have functional defects and increased apoptosis that are ameliorated by metformin. J. Clin. Endocrinol. Metab. 89(11):5535-5541. |
|
|
Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B (2009). Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 32(1):193-203. |
|
|
Nisly SA, Kolanczyk DM, Walton AM (2013). Canagliflozin, a new sodium-glucose cotransporter 2 inhibitor, in the treatment of diabetes. Am. J. Health Syst Pharm. 70(4):311-319. |
|
|
Polidori D, Sha S, Mudaliar S, Ciaraldi TP, Ghosh A, Vaccaro N, Farrell K, Rothenberg P, Henry RR (2013). Canagliflozin Lowers Postprandial Glucose and Insulin by Delaying Intestinal Glucose Absorption in Addition to Increasing Urinary Glucose Excretion: Results of a randomized, placebo-controlled study. Diabetes Care 36(8):2154-2161. |
|
|
Prasanna K, Narsimha R (2014). Evaluation of clarithromycin pharmacokinetics after single and repeated oral administration of atorvastatin in hyperlipidemicWistar rats. Afr. J. Pharm. Pharmacol. 8(15):399-407. |
|
|
Randle P, Garland P, Hales C, Newsholme E (1963).The glucose fatty-acid cycle its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet 281(7285):785-789. |
|
|
Randle P, Newsholme E, Garland P (1964). Regulation of glucose uptake by muscle. 8. Effects of fatty acids, ketone bodies and pyruvate, and of alloxan-diabetes and starvation, on the uptake and metabolic fate of glucose in rat heart and diaphragm muscles. Biochem. J. 93(3):652-665. |
|
|
Reed MJ, Meszaros K, Entes LJ, Claypool MD, Pinkett JG, Gadbois TM, Reaven GM (2000). A new rat model of type 2 diabetes: the fat-fed, streptozotocin-treated rat. Metabolism 49(11):1390-1394. |
|
|
Reeves PG, Nielsen FH, Fahey GCJr (1993). AIN-93 Purified Diets for Laboratory Rodents: Final Report of the American Institute of Nutrition Ad Hoc Writing Committee on the Reformulation of the AIN-76A Rodent Diet. J. Nutr. 123(11):1939-1951. |
|
|
Rutkowska J, Adamska A (2011). Fatty Acid Composition of Butter Originated from North-Eastern Region of Poland. Pol. J. Food Nutr. Sci. 61(3):187-193. |
|
|
Saad M, Kamel M, Hanafi M (2015). Modulation of Adipocytokines Production and Serum NEFA Level by Metformin, Glimepiride, and Sitagliptin in HFD/STZ Diabetic Rats. Biochem Res Int. 7p. |
|
|
Sahin K, Onderci M, Tuzcu M, Ustundag B, Cikim G, Ozercan IH, Sriramoju V, Juturu V, Komorowski JR (2007). Effect of chromium on carbohydrate and lipid metabolism in a rat model of type 2 diabetes mellitus: the fat-fed, streptozotocin-treated rat. Metabolism 56(9):1233-1240. |
|
|
Sasidharan S, Joseph J, Anandakumar S, Venkatesan V, AriyattuMadhavan C,Agarwal A (2013). An experimental approach for selecting appropriate rodent diets for research studies on metabolic disorders. Biomed Res Int. 2013:752870. |
|
|
Scheen AJ. (2015). Pharmacodynamics, efficacy and safety of sodium-glucose co-transporter type 2 (SGLT2) inhibitors for the treatment of type 2 diabetes mellitus. Drugs 75(1):33-59. |
|
|
Srinivasan K, Viswanad B, Asrat L, Kaul C, Ramarao P (2005). Combination of high-fat diet-fed and low-dose streptozotocin-treated rat: A model for type 2 diabetes and pharmacological screening. Pharmacol. Res. 52(4):313-320. |
|
|
Stanton R (2014). Sodium Glucose Transport 2 (SGLT2) Inhibition Decreases Glomerular Hyperfiltration: Is There a Role for SGLT2 Inhibitors in Diabetic Kidney Disease? Circulation 129(5):542-544. |
|
|
Stenlöf K, Cefalu WT, Kim KA, Alba M, Usiskin K, Tong C, Canovatchel W, Meininger G (2013). Efficacy and safety of canagliflozinmonotherapy in subjects with type 2 diabetes mellitus inadequately controlled with diet and exercise. Diabetes Obes. Metab. 15(4):372-382. |
|
|
UK Prospective Diabetes Study (UKPDS) Group (1998). Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 352(9131):854-865. |
|
|
Vivian E (2014). Sodium-glucose co-transporter 2 (SGLT2) inhibitors: a growing class of antidiabetic agents. Drugs Context 3:212264. |
|
|
Wiernsperger N, Bailey C (1999). The antihyperglycaemic effect of metformin: therapeutic and cellular mechanisms. Drugs 58(1):31-39. |
|
|
Woods SC, Seeley RJ, Rushing PA, D'Alessio D, Tso P (2003). A controlled high-fat diet induces an obese syndrome in rats. J. Nutr. 133(4):1081-1087. |
|
|
Yang XP, Lai D, Zhong XY, Shen HP, Huang YL (2014). Efficacy and safety of canagliflozin in subjects with type 2 diabetes: systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 70(10):1149-1158. |
|
|
Zhang F, Ye C, Li G, Ding W, Zhou W, Zhu H, Chen G, Luo T, Guang M, Liu Y, Zhang D, Zheng S, Yang J, Gu Y, Xie X, Luo M (2003). The rat model of type 2 diabetes mellitus and its glycometabolism characters. Exp. Anim. 52(5):401-407. |
|
|
Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, Wu M, Ventre J, Doebber T, Fujii N, Musi N, Hirshman MF, Goodyear LJ, Moller DE (2001). Role of AMP-activated protein kinase in mechanism of metformin action. J. Clin. Invest. 108(8):1167-1174. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


