ABSTRACT
There is an alarming rise in treatment failures from artemisinin combination therapy (ACT). The aim of this study was to access the therapeutic effectiveness of ACT in the market and the rate of re-occurrence of malaria shortly after completion of therapy. The rate of adherence to therapy and relapse rate of four hundred volunteers, who recently treated malaria, were assessed using quantitative interview-semi structured questionnaire. Adherence levels were 56.0% while relapse rate was 47.0%. The rate of relapse among volunteers who adhered to therapy was 40.63%. While encouraging continuous quality assessment of artemisinin combination drugs, it is equally important for public health practitioners and institutions to design deliberate programs to enlighten the public on the importance of adherence to therapy as this rather than quality of medicines may be contributing largely to drug resistance.
Key words: Artemisinin combination therapy, malaria, quality assessment.
Despite the enormous interventions, malaria is still a concern in most developing countries in Africa. Malaria is the most significant
parasitic disease of humans, and claims the lives of more children worldwide than any other infectious disease and it is the third most infectious diseases plaguing the sub-Saharan regions with tuberculosis and diarrhoeal infections and has become a major public health issue and concern (World Health Organization, 2014). The emergence of resistant strains of
Plasmodium falciparum to chloroquine and some antimalarial drugs led to the World Health Organisation recommendation on the use of artemisinin combination therapy (ACT) as a first line treatment for uncomplicated malaria (Ezenduka et al., 2014). According to the National Malaria Elimination Program (NMEP) Strategic Plan 2014-2020, malaria accounts for about 60% of outpatient visits and 30% of hospitalizations in Nigeria. It is a leading cause of mortality in children underfive, and is responsible for an estimated 300,000 total deaths annually (President’s Malaria Initiative Nigeria, 2015).
Artemisinin which is isolated from the plant Artemisia annua is a sesquiterpene lactone with an unusual peroxide bridge believed to be responsible for the therapeutic actions of the plant. Artemisinins not merely achieve prompt clearance of the asexual parasites that are responsible for symptomatic blood-stage infection; they also diminish the numbers of sexual-stage parasites (gametocytes) responsible for spread. Combined with a second, longer acting partner drug, the resultant artemisinin-based combination therapy (ACT) is expected to allow fewer opportunities for the progress of drug resistance as the artemisinin component kills the majority of parasites at the start of the treatment, while the more slowly metabolized partner drug clears the lingering parasites. The biggest challenge yet to the effective control of malaria is combating drug resistance. The parasite responsible for malaria (P. falciparum) is becoming resistant even to ACT (Obidike et al., 2013; Afonso et al., 2006; Wongsrichanalai and Meshnick, 2008). Attempts by health research scientists to identify the root causes of drug resistance to malaria have largely focused on the quality pharmaceuticals (El-Duah and Ofori-Kwakye, 2012). Little attention is given to the role of individual patients in creating favourable environment for resistance to grow; lack of adherence to complete treatment regimen may be a fair factor contributing not only to the spread of drug resistance, but also to the disturbing increase in malaria-related morbidity and mortality. For example, El-Duah and Ofori-Kwakye (2012) attributed the emerging resistance to ACTs to the supply and distribution of poor quality (counterfeit or substandard) artemisinin-based anti-malarial drugs in various countries. There are also various reports on the resistance of P. falciparum to ACTs in circulation in some parts of Nigeria (Ibekwe, 2009; Ajayi and Ukwaja, 2013).
The aim of this study therefore was to assess the use of artemisinin combination therapy among Abuja residents who recently treated malaria in order to evaluate the adherence pattern and relapse rate.
Study design and site
The volunteers used in the study were selected from nine different locations within the Federal Capital Territory, Nigeria. The territory is located in the North Central Geo-Political Zone of Nigeria. FCT Abuja is the capital of Nigeria. It occupies a land area of 7,753.9 km2. It comprises of both urban and rural settlement. All subjects were requested to fill a consent form admitting them into the study. Volunteers were also told that the inclusion into the study was not by compulsion and they were free to opt out.
Exclusion criteria
People below the age of 15 and above 70 years were excluded from the study. Volunteers who had no prior knowledge about malaria infection or who had not treated malaria with ACTs within the past one month were also excluded from the study.
Information provided
At recruitment, subjects were provided with an information sheet in English detailing the purpose of the study, which was also explained verbally. Volunteers’ queries were answered after which they were invited to provide a written consent.
Sampling method
Four hundred volunteers were administered quantitative interviews using a semi structured questionnaire to assess their adherence to therapy levels (adherence to dosing frequency and duration) and rate of relapse of malaria (El-Duah M and Ofori-Kwakye, 2012).
Data analyses
Data analysis was performed using SPSS Version 16 (SPSS Inc. Chicago IL, USA) and Graph Pad Prism 5.
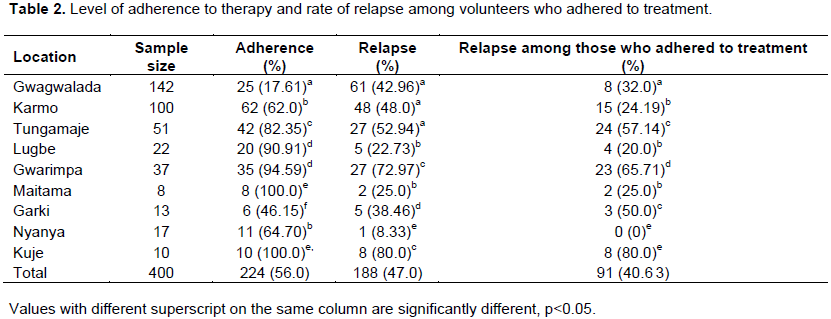
The results on the bio data/characteristics of the study population are represented in Table 1. A total of 197 males and 203 females volunteered to be included in the study. The age distribution was in four categories: 15-29 (205), 30-44 (129), 44-60 (48), and above 60 (18) years. Most of the respondents were students. The results on their level of education showed that most respondents were literate (363) with most of them having tertiary education (167). The level of adherence to therapy and malaria relapse rate is shown in Table 2. There was a wide variation in the level of adherence (17.61 to 100%). The relapse rate generally was 8.33 to 80.0% and relapse among respondent who adhered to treatment guideline was 0 to 80.0%.
The poor adherence (56.0%) habit of the study population in this study is a matter of great concern and could be linked to poor awareness of the public on the importance of adhering strictly to their prescribed treatment regimen. Adherence has been defined as the degree to which patients use medicines according to the health providers’ prescriptions and is an essential element in the control of infectious disease (Chatio et al., 2015). Some of the respondents confirmed that during the course of therapy they either skipped a dose of their medication or did not continue therapy as soon as they got relief from the symptoms of the disease. This corresponds with recent reports that certain individuals frequently use medicines incompletely or halt the management once the signs lessen and preserve the rest to be used later (Mace et al., 2011). Forgetfulness and poor patient- health professional relationship have been shown to affect adherence to the usage of medicines including ACTs (Osterberg and Blaschke, 2005).
Other factors that have been reported to affect adherence to medication is the use of intricate or technical terms by health providers while prescribing. A study by Amponsah et al. (2015) shows that about 76% of patients with malaria failed to complete their treatment as prescribed due to poor knowledge on malaria. Many of the measures used to improve adherence emphasize on the provision of education to increase knowledge; simplifying the medication regimen (fewer drugs or fewer doses); or making it easier to remember-adherence aids, refill reminders (World Health Organization, 2014).
Comprehensive interventions should address a variety of issues, including knowledge, motivation, social support, and individualizing therapy based on a person's concerns and needs. This agrees with a study by Khantikul et al. (2009) who associated adherence behaviour of people to their level of access to information on anti-malarials and demographic factors.
The average re-occurrence (relapse) of malaria infection- after treatment with the ACTs, within the study group was 47.0%. This high rate of relapse can be linked to inability of the respondents to strictly adhere to their medication, a possibility of treatment failure from the drugs or re-infection by the malaria parasite. However, the most alarming aspect is the high relapse (40.63%) rate among volunteers who claimed to have strictly adhered to their treatment. This can be due to the use of counterfeit or substandard ACTs or a case of re- infection. Recent findings have associated treatment failures to distribution of counterfeit and substandard drugs (El-Duah and Ofori-Kwakye, 2012). In sub-Saharan Africa, the circulation of substandard and perhaps counterfeit artemisinin-based formulations is posing a threat to the wellbeing of citizens and is wide becoming a gross public health issue. A quality assessment study of different brands of ACT in the Nigerian market reported significant variances in the dissolution profiles of some brands of artesunate tablets, with one product possessing an extremely low dissolution rate which can result in poor bioavailability of the product (Esimone et al., 2008). Be that as it may, the role of individual patients in creating favourable environment for resistance to grow possibly due to low or absence of adherence to complete treatment regimen may be a fair factor contributing to the spread of malaria drug resistance.
In the opinion of these researchers, malaria is a public health emergency in Africa and until African health administrators and political leaders see it as such, we shall continue to suffer its devastating impact especially on pregnant women and children.
There is need for public enlightenment on the use of ACTs with emphasis on the need to adhere strictly to anti-malarial therapy. While continuous regular quality assessment of the various brands of ACTs in the market is encouraged, we propose that, there is need to carry out studies to correlate non-adherence to resistance development.
The authors have not declared any conflict of interests.
The authors are grateful to the Management of the National Institute for Pharmaceutical Research and Development as well as the staff of Microbiology and Biotechnology Department of the Institute for their contribution. They appreciate the efforts of those who contributed immensely to the distribution and collation of the questionnaires. The authors also appreciate the contributions of Mrs Christiana Daniels for the statistical analysis of the study.
REFERENCES
|
Afonso A, Hunt P, Cheesman S, Alves AC, Cunha CV, Do Rosário V, Cravo P (2006). Malaria parasites can develop stable resistance to artemisinin but lack mutations in candidate genes atp6 (encoding the sarcoplasmic and endoplasmic reticulum Ca2+ ATPase), tctp, mdr1, and cg10. Antimicrob. Agents Chemother. 50(2):480-489.
Crossref
|
|
|
|
Ajayi NA, Ukwaja KN (2013). Possible artemisinin-based combination therapy-resistant malaria in Nigeria: a report of three cases. Rev. Soc. Bras. Med. Trop. 46(4):525-527.
Crossref
|
|
|
|
|
Amponsah AO, Vosper H, Marfo AA (2015). Patient Related Factors Affecting Adherence to Antimalarial Medication in an Urban Estate in Ghana. Malar. Res. Treat. pp. 1-8.
Crossref
|
|
|
|
|
Chatio S, Aborigo R, Adongo PB, Anyorigiya T, Akweongo P, Oduro A (2015). Adherence and uptake of artemisinin- based combination treatments for uncomplicated malaria: A qualitative study in Northern Ghana. PLoSONE 10(2):1-14.
Crossref
|
|
|
|
|
El-Duah M, Ofori-Kwakye K (2012). Substandard artemisinin-based antimalarial medicines in licensed retail pharmaceutical outlets in Ghana. J Vector Borne Dis. 49:131-139.
|
|
|
|
|
Esimone CO, Okoye FBC, Onah BU, Nworu CS, Omeje EO (2008). In vitro bioequivalence study of nine brands of artesunate tablets marketed in Nigeria. J Vector Borne Dis. 45:60-65.
|
|
|
|
|
Ezenduka CC, Okonta MJ, Esimone CO (2014). Adherence to treatment guidelines for uncomplicated malaria at two public health facilities in Nigeria; Implications for the 'test and treat' policy of malaria case management. J. Pharmaceut. Policy Pract. 7:1-5.
Crossref
|
|
|
|
|
Ibekwe J (2009). Artemisinin resistant M#malaria on the horizon. Int. J. Med. Med. Sci. 1(6):1-3.
|
|
|
|
|
Khantikul N, Butraporn P, Kim HS, Leemingsawat S, Tempongko SB, Suwonkerd W (2009). Adherence to antimalarial drug therapy among Vivax Malaria Patients in Northern Thailand. J. Health Popul Nutr. 27(1):4-13.
Crossref
|
|
|
|
|
Mace KE, Mwandama D, Jafali J, Luka M, Filler SJ, Sande J, Ali D, Kachur SP, Mathanga DP, Skarbinski J (2011). Adherence to treatment with artemether-lumefantrine for uncomplicated malaria in rural Malawi. Clin. Infect. Dis. 53(8):772-779.
Crossref
|
|
|
|
|
Obidike IC, Okhale S, Aboh MI, Salawu OA (2013). Isolation, fractionation and evaluation of the antiplasmodial properties of Phyllanthus niruri resident in its chloroform fraction. Asian Pac. J. Trop. Med. 6(3):169-175.
Crossref
|
|
|
|
|
Osterberg L, Blaschke T (2005). Adherence to medication. N. Engl. J. Med. 353:487-497.
Crossref
|
|
|
|
|
President's Malaria Initiative Nigeria (2015). Malaria operational plan FY 2015 P 15.
|
|
|
|
|
World Health Organization (WHO) (2014). World Malaria Report 2014 FACT SHEET. Available:
View Accessed 2014 Nov 3.
|
|
|
|
|
Wongsrichanalai C, Meshnick SR (2008). Declining artesunate-mefloquine efficacy against falciparum malaria on the Cambodia Thailand border. Emerg. Infect. Dis. 14:716-719.
Crossref
|
|