ABSTRACT
Elevated level of cholesterol is a risk factor for the development of cardiovascular disease. Community pharmacies are considered as ideal settings to provide screening services for chronic medical conditions. An adequate knowledge and a positive attitude towards cholesterol screening would increase pharmacist’s involvement in cholesterol lowering interventions and referrals. The objective of this study was to assess community pharmacists’ knowledge, attitude and resource availability in relation to cholesterol screening in Delta State, Nigeria. A 33 item pre tested self-administered questionnaire with a Cronbach’s alpha value of 0.628 was distributed to all 160 community pharmacists in Delta State. The questionnaire items assessed knowledge, attitude and available resources in relation to cholesterol screening. Categorical data was expressed as frequency and percentages. Chi-square test was performed to explore relationship between demographic variables and pharmacist’s knowledge. A p-value of less than 0.05 was considered statistically significant. More than half (64.7%) of community pharmacist were knowledgeable in relation to cholesterol and its influence on cardiovascular diseases. Cholesterol screening services were provided by only 11.3% community pharmacies in Delta State. Majority (82%) were willing to be trained in the use of cholesterol meter. Nearly half, 42.9% had a negative attitude towards cholesterol screening. Pharmacist’s knowledge about cholesterol and its influence in cardiovascular diseases was satisfactory. However, attitude towards cholesterol screening was largely negative and provision of such services was very low.
Key words: Cholesterol screening, community pharmacies, knowledge, Nigeria.
Cardiovascular diseases (CVD) have continued to exact a heavy toll on people in developing and developed countries of the world with devastating impact on quality of life (Go et al., 2014; WHO, 2014; Mozaffarian et al., 2015). Risk factors for development of CVD include high blood pressure, diabetes mellitus, smoking, and elevated serum cholesterol which is considered an independent risk factor for CVD (Wadhera et al., 2016; WHO, 2015; Keys et al., 1984). A positive relationship exists between total serum cholesterol levels, triglyceride levels, other arthrogenic particles and the development of CVD especially coronary heart disease (Stamler et al., 1986; Toth, 2005; Assmann et al., 1998; Austin et al., 1998).
Though the benefits of lowering cholesterol levels on the prevention of future heart attack, stroke, and death, have been well established both in those at risk and in persons with established CVD (Almuti et al., 2005; MRC/BHF, 2002; Anderson et al., 2013), there is still a huge treatment gap leaving out many persons who would have benefited from lipid lowering therapy (Hoerger et al., 1998; Bolli, 2014; Ahn et al., 2015). Also, for many persons on treatment, adherence to therapy is often compromised by perceived adverse effects of medication, resulting in discontinuation (Bitton et al., 2013; Roebuck et al., 2011). Community pharmacists are in an ideal position to support management of dyslipidemia and reduce risks associated with CVD, because they are highly accessible and are often the first point of entry into the health care system (Joyce et al., 2007). Pharmacists could assist by engaging in screening for dyslipidemia, promoting awareness and lifestyle interventions, and increasing adherence through assessment and resolution of drug therapy problems associated with use of lipid lowering medications.
A good knowledge of cholesterol and its influence on cardiovascular diseases, as well as a positive attitude towards cholesterol screening could increase impact of community pharmacists in reducing cardiovascular disease burden through cholesterol lowering inter-ventions. The objectives of this study were too assess the knowledge of community pharmacists in relation to cholesterol and its influence on cardiovascular diseases, evaluate attitude of community pharmacists towards cholesterol screening and to determine resources available in community pharmacies for cholesterol screening.
Study design
A cross sectional survey design was used for this study. A pretested 33 item questionnaire with Cronbach’s alpha value of 0.628 was distributed to the resident pharmacists at the various community pharmacies in Delta State.
Setting
This research was carried out in registered community pharmacies located in Delta State, Nigeria. Delta State is an oil rich state situated in the Niger Delta region of the country. A teaching hospital, several general hospitals and a host of private medical facilities offer health care services in the state. Laboratory services are provided by public and private laboratory facilities in the state.
Population/sample size
The population consisted of all community pharmacies in the state. The total number of registered community pharmacists in the state was 160. In view of the small population size, a census of all community pharmacies in the state was done.
Data collection and presentation
A pretested self-completion questionnaire was distributed to the pharmacists in charge of all community pharmacies in the state. The questionnaire was pretested in a sample of 25 community pharmacists in Asaba, the state capital city. The questionnaire consisted of 33 questions divided into four sections. Section A addressed pharmacist demographics. Section B contained questions assessing pharmacist’s knowledge, while Section C addressed pharmacist’s attitude towards cholesterol screening. Section D consisted of questions relating to resource availability for cholesterol screening in community pharmacies. Institutional permit was obtained for the study.
Data analysis
Data collected were entered into Microsoft Excel spread sheet and crosschecked for errors and missing data. Then, they were finally exported into the Statistical Package for Social Sciences (SPSS) software. Responses to the 20 knowledge questions were expressed as frequency and percentages. Pharmacists attitude was measured on a 5 point Likert scale ranging from 1 (strongly agree to 5 (strongly disagree) with an assumed midpoint of 3. Rated scores were treated as interval data suitable for quantitative analysis. Chi-square test was performed to explore relationship between demographic variables and pharmacist’s knowledge. A p-value of less than 0.05 was considered statistically significant.
Demographic characteristics of pharmacists
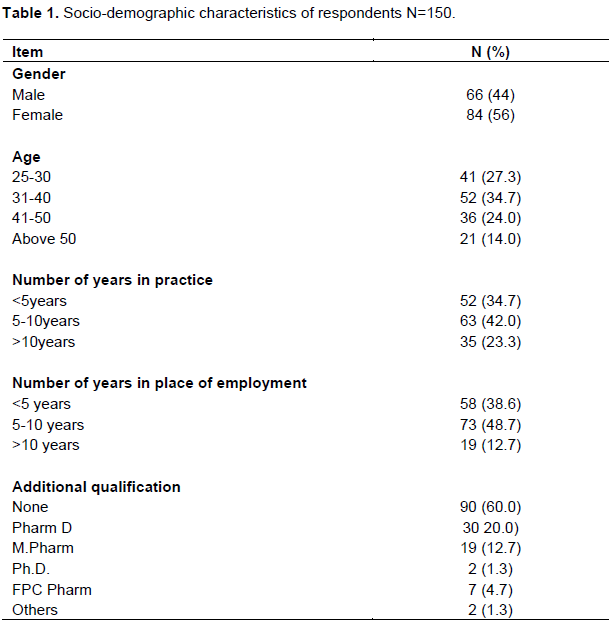
A total of 160 questionnaires were distributed but 150 were retrieved thus giving a response rate of 93.75%. Cronbach’s alpha value for the questionnaire showed modest level of internal consistency (0.628). There were more females (84, 56%) than males (66, 44%). The predominant age group was 31 to 40 years. Nearly half of the pharmacists have been in the practice for 5 to 10 years (42%) and most of them had no additional qualifications (60%) (Table 1).
Knowledge of cardiovascular disease
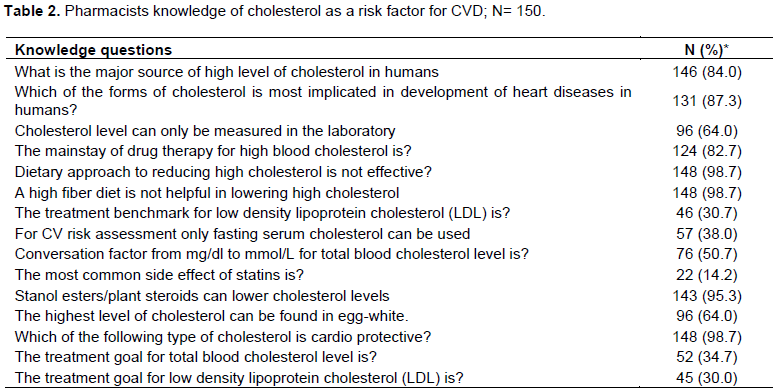
Knowledge about cholesterol and its influence in cardiovascular diseases was satisfactory as more than half (64.7%) of the respondents answered all knowledge questions correctly. However, scores were very low on questionnaire items relating to treatment targets for arthrogenic lipid fractions and side effects of statins (Table 2).
Proportion of pharmacists that answered knowledge questions correctly
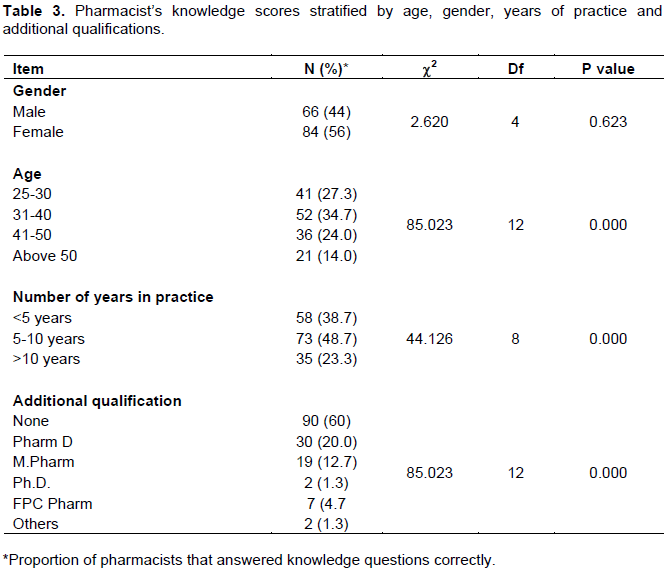
Age, practice experience and additional qualifications were significantly associated with pharmacist’s knowledge of cholesterol (Table 3).
Attitude to cholesterol screening
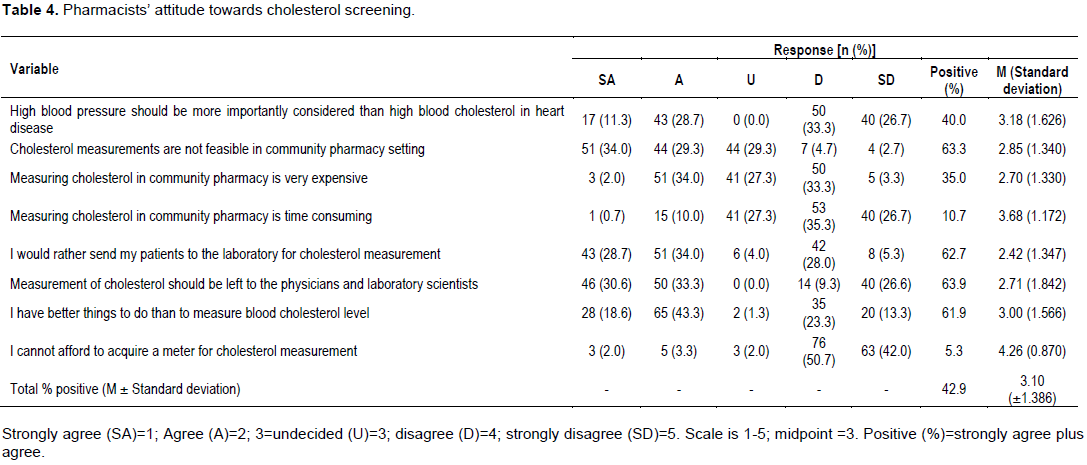
The overall percentage positive response to questions reflecting a negative attitude to cholesterol screening was 42.9% indicating that nearly half of pharmacists had a negative attitude towards cholesterol screening. Affordability of the cholesterol screening equipment was not a major factor influencing this negative attitude as only 5.3% strongly agreed or agreed with the statement that they could not afford cholesterol meters. More than half; 63.3% strongly agreed or agreed that cholesterol screening was not feasible in the pharmacy and that it should be left to laboratory scientists (63.9%). Details of pharmacist attitude with respect to cholesterol screening are shown in Table 4.
Resources for cholesterol screening
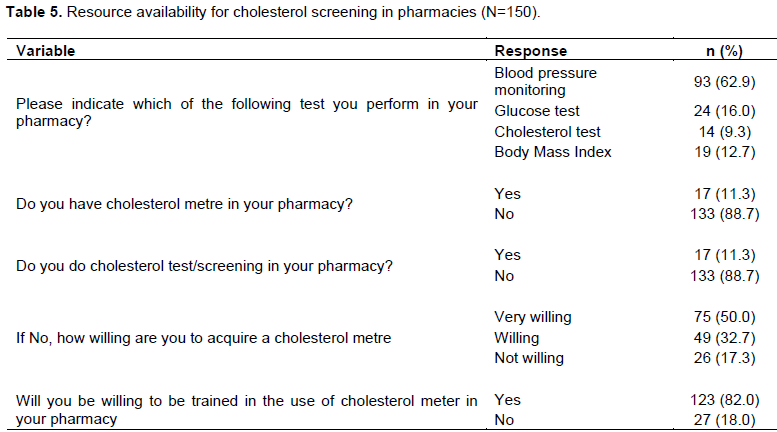
More than half of pharmacists surveyed (62%) were involved in blood pressure screening. Only 17 (11.3%) had cholesterol meters in the pharmacy and cholesterol screening was done by a very small percentage of pharmacists (9.3%). Majority (82%) of the pharmacists expressed a willingness to be trained in the use of cholesterol metre (Table 5).
The study population represented a wide variety of pharmacists’ cutting-across different age, gender, and experience in community pharmacy practice. There was predominance of females in the study population. This is in line with a similar study carried out in Great Britain in 2005 where it was observed that over 54.7% of practicing pharmacists were of the female gender (Hassell and Eden, 2006).
More than half of community pharmacists were knowledge able in relation to cholesterol and its influence other studies that show an inverse relationship between pharmacists practice experience and knowledge (Ibrahim and Hussein, 2017; Khan and Azha, 2017).
The significant association between additional qualification and knowledge agrees with the findings of an Indian study that showed that pharmacists with additional qualifications were significantly more knowledgeable than those with basic pharmacy degree (Ahmad et al., 2013). The most common service rendered was blood pressure assessment. The frequency of blood glucose, weight assessment and cholesterol screening performed in the various pharmacy outlets were also very low. The aforementioned Iranian study showed that although two-third of the participants believed that well-trained pharmacists can effectively deliver such services in community pharmacies, cholesterol screening services were rarely provided in Iranian community pharmacies. In contrast to these findings, pharmacists in developed countries have been involved in cholesterol screening and cardiovascular risk assessment for decades (Blenkinsopp et al., 2003; Bluml et al., 2000). That majority of community pharmacists surveyed expressed willingness to be trained in the use of cholesterol meter is a clarion call to national pharmacy organizations to evolve, initiate and implement point of care training programs for pharmacists.
Pharmacist’s knowledge about cholesterol and its influence in cardiovascular diseases was satisfactory. Pharmacists’ attitude towards providing cholesterol screening services in community pharmacies in Delta State was largely negative and resource availability was poor. However, majority of the pharmacists surveyed expressed willingness to be trained in the use of cholesterol meter.
Community pharmacy-based cholesterol screening training model should be developed in order to improve participation, output and impact of pharmacists in disease screening activities and to increase opportunistic high cholesterol detection rates in the general population.
The authors have not declared any conflict of interests.
REFERENCES
|
Ahmad A, Patel I, Balkrishnan R, Mohanta GP, Manna PK (2013). An evaluation of knowledge, attitude and practice of Indian pharmacists towards adverse drug reaction reporting: A pilot study. Perspect. Clin. Res. 4(4):204-210.
Crossref
|
|
|
|
Ahn E, Shin DW, Yang H, Yun JM, Chun SH, Suh B, Cho B (2015). Treatment Gap in the National Health-screening Program in Korea: Claim-based Follow-up of Statin Use for Sustained Hypercholesterolemia. J. Korean Med. Sci. 30(9):1266-1272.
Crossref
|
|
|
|
|
Almuti K, Rimawi R, Spevack D, Ostfeld RJ (2005) Effects of statins beyond lipid lowering: Potential for clinical benefits. Int. J. Cardiol. 109(1):7-15.
Crossref
|
|
|
|
|
Anderson TJ, Gregoire J, Hegele RA, Concutre P, John Mancini GB, McPherson R, Francis GA, Poirier P, Lau DC, Grover S, Genest J (2013) 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can. J. Cardiol. 29(2):151-167.
Crossref
|
|
|
|
|
Assmann G, Schulte H, Funke H, von Eckardstein A (1998).The emergence of triglycerides as a significant independent risk factor in coronary artery disease. Eur. Heart J. 19(suppl M):M8-M14.
|
|
|
|
|
Austin MA, Hokanson JE, Edwards KL (1998). Hypertriglyceridemia as a cardiovascular risk factor. Am. J. Cardiol. 81:7B-12B.
Crossref
|
|
|
|
|
Bitton A, Choudhry NK, Matlin OS, Swanton K, Shrank WH (2013). The impact of medication adherence on coronary artery disease costs and outcomes: a systematic review. Am. J. Med. 126(4):357-e7
Crossref
|
|
|
|
|
Blenkinsopp A, Anderson C, Armstrong M. (2003). Systematic review of the effectiveness of community pharmacy-based interventions to reduce risk factors for coronary heart disease. J. Public Health Med. 25:144-153.
Crossref
|
|
|
|
|
Bluml BM, McKenney JM, Cziraky MJ (2000). Pharmaceutical care services and result in Project Impact: Hyperlipidemia. J. Am. Pharm. Assoc.40:157-65.
Crossref
|
|
|
|
|
Bolli P (2014) Treatment of dyslipidemia- the problem of reaching the goal. Atherosclerosis 236(1):142-143
Crossref
|
|
|
|
|
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ (2014) Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation 129(3):e28.
Crossref
|
|
|
|
|
Hassell K, Eden M (2006). Workforce update – joiners, leavers and practicing and non-practicing pharmacists on the 2005 Register. Pharm. J. Vol. 276.
|
|
|
|
|
Hoerger T, Bala M, Bray JW, Wilcosky TC, LaRosa J (1998) Treatment patterns and distribution of low-density lipoprotein cholesterol levels in treatment-eligible United States adults. Am. J .Cardiol. 82(1):61-65.
Crossref
|
|
|
|
|
Ibrahim OM, Hussein1 RN (2017) Knowledge of pharmacists on proper use of oral contraceptive pills and missed dose instructions in United Arab Emirates Trop. J. Pharm. Res. 16(4):947-954
|
|
|
|
|
Jahangard-Rafsanjani Z, Sarayani A, Javadi MR., Hadjibabaie M, Rashidian A, Gholami K (2014). Pharmacist's Attitudes and Perceived Barriers about Community Pharmacy-Based Cardiovascular Risk Screening Services. J. Pharm. Care 2(4):142-148.
|
|
|
|
|
Joyce AW, Sunderland VB, Burrows S, McManus A, Howat P, Maycock B (2007). Community pharmacy's role in promoting healthy behaviors. J. Pharmacy Pract. Res. 37(1):42-44.
Crossref
|
|
|
|
|
Keys A, Menotti A, Aravanis C, Blackburn H, Djordjevic BS, Buzina R, Dontas AS, Fidanza F, Karvonen MJ, Kimura N, Mohacek I, Nedeljkovic S, Puddu V, Punsar S, Taylor HL, Conti S, Kromhout D, Toshima H (1984). The Seven Countries Study: 2,289 deaths in 15 years. Prev. Med. 13(2):141-54.
Crossref
|
|
|
|
|
Khan TM, Azhar S (2013). A study investigating the community pharmacist knowledge about the appropriate use of inhaler, Eastern Region AlAhsa, Saudi Arabia. Saudi Pharm. J. 21(2):153-157.
Crossref
|
|
|
|
|
Lee J, Matthew H, Damon B, Ines K, Gerald FW (2013). An audit of pharmacists' knowledge of familial hypercholesterolemia: Implications for community healthcare. Australian Pharm. 32(7):73-75.
|
|
|
|
|
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ, Howard VJ (2015a) – Heart Disease and Stroke Statistics – 2015 Update – A report from the American Heart Association. Circulation 2015, 131(4):e29-322.
Crossref
|
|
|
|
|
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Després JP, Fullerton HJ (2015b). Erratum for Heart Disease and Stroke Statistics—2015 Update A Report From the American Heart Circulation. 2015 Jun 16; 131(24):e535. Available at:
Pubmed
|
|
|
|
|
NCEP (2002). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report Circulation. 106:3143, Available at:
Pubmed
|
|
|
|
|
Roebuck MC, Liberman JN, Gemmill-Toyama M, Brennan TA (2011) Medication adherence leads to lower health care use and costs despite increased drug spending. Health Aff. (Millwood). 30(1):91-99.
Crossref
|
|
|
|
|
Stamler J, Wentworth D, Neaton JD (1986). Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356 222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA; 256(20):2823-2828.
Crossref
|
|
|
|
|
Toth PP (2005). The 'good cholesterol': high-density lipoprotein. Circulation, 111(5):e89-e91.
Crossref
|
|
|
|
|
Wadhera RK, Steen DL, Irfan K, Giugliano RP, Foody JM. (2016) A review of low-density lipoprotein cholesterol, treatment strategies, and its impact on cardiovascular disease morbidity and mortality. J. Clin. Lipidol. 10(3):472-489
Crossref
|
|
|
|
|
World Health Organization (WHO) (2015). Fact sheet heart disease risk factors. Available at
View
|
|
|
|
|
World Health Organization (WHO) (2014). The top 10 causes of death. Web site.
|
|
|
|
|
SPSS, S. (2010). 19.0. 0 for Windows Software. SPSS Inc., IBM Company, USA.
|
|