Full Length Research Paper

ABSTRACT
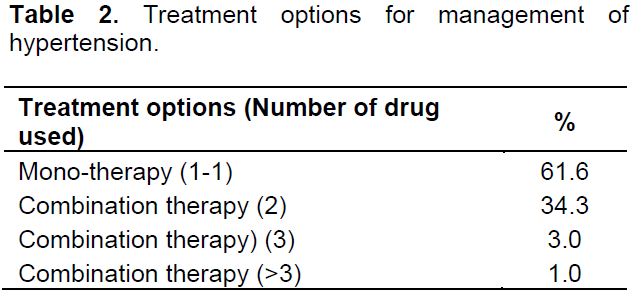
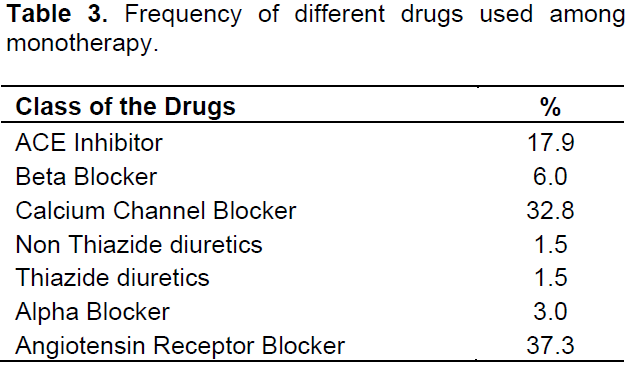
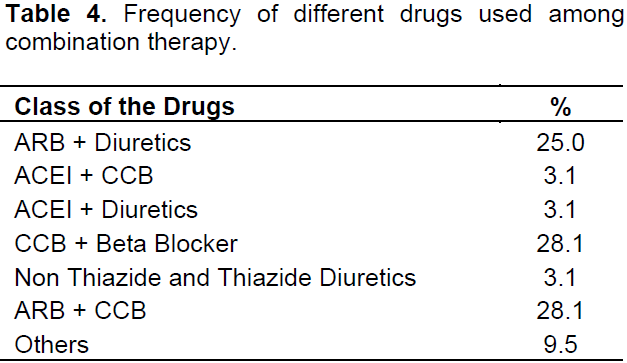
The exponential increase in patients with hypertension puts an enormous burden on healthcare providers. To describe the trends in the prescription of antihypertensive medication in a tertiary care hospital, Bangladesh is the objective of the study. This is a hospital based descriptive cross sectional study conducted at the Medicine outpatient Department in Dhaka Medical College Hospital. Patients more than 20 years of age suffering from Hypertension were included in the study. Data was collected by interviewing using a semi-structured questionnaire and analysed by computer with the help of SPSS 16. A total hundred patients were included in the study and 61.6% patients were prescribed on single drug and 38.4% patients were prescribed on combined therapy. Among the prescriptions having single anti-hypertensive medication most commonly used drugs are Angiotensin Receptor Antagonist (37.3%), Calcium Channel Blocker (32.8%), and ACE Inhibitor (17.9%), Beta Blocker (6%), Alpha Blocker (3%), Thiazide and non-Thiazide Diuretics 1.5% each. Among the prescriptions having combined drug therapy Angiotensin Receptor Blocker along with Calcium Channel Blocker and Calcium Channel Blocker along with Beta Blocker were equally (28.1%) chosen by the physicians and use of Angiotensin Receptor Blocker along with Diuretics was 25%, ACE Inhibitor with Calcium Channel Blocker 3.1%, ACE Inhibitor with Diuretics 3.1%, Thiazide and Non Thiazide Diuretics was 3.1% and other drugs were used for 9.5%. Pattern of using antihypertensive medications varies according to presence of co-morbidities and duration but does not vary significantly between male and female patients.
Key words: Anti-hypertensive drugs, hypertension, prescription pattern, management of hypertension.
INTRODUCTION
Hypertension has been identified as the leading global risk factor for mortality and considered as the third contributing factor of disease burden worldwide that makes it a major public health challenge (Rodgers et al., 2004). Elevated blood pressure accounts for two-thirds and one-half of all cases of stroke and ischemic heart disease respectively. Prevalence of chronic kidney disease is about 22% among the undiagnosed hypertensive patients and 17% of pre hypertensive patients in the USA (Alam et al., 2014). The exponential increase in the patients with hypertension puts an enormous burden on both the healthcare authorities an healthcare providers.
Eighty percent of this burden occurred in low socio economic and middle-income countries. Prompt and proper management of hypertension can significantly minimize the risk of stroke by 30-41% and of coronary heart diseases by 22%. Despite the availability of effective treatments, studies have shown that in many countries, less than 25% of patients treated for hypertension achieved optimum blood pressure. It is found that early detection, treatment, and control of hypertension are inadequate in low-income countries and awareness about hypertension is also low. Sometimes the situation is even worse (Khanam et al., 2014).
Bangladesh is passing through a phase of epidemiological transition from communicable diseases to non-communicable disease and currently has a double burden of disease (Moniruzzamani et al., 2013). This indicates that the prevalence of hypertension is modest now but will show a rising trend. But only a few studies were done to find out the actual prevalence of essential Hypertension in Bangladeshi people. According to a meta-analysis covering studies up to 1994 reported a prevalence of hypertension among the adult population of Bangladesh is 11.3% (Zaman et al., 2011). Though globally cardiologists play the major role for treating hypertension even at initial stage (Majumder, 2012) but the scenario of Bangladesh is slightly different in this aspect. The primary goal of the management of hypertension is to achieve the maximum reduction in the long-term total risk of cardiovascular morbidity and mortality (Mancia et al., 2007). But owing to unfavourable socio-economic condition most of the people in Bangladesh especially the poor or marginalized people do not consult cardiologist for the initial treatment of hypertension or uncomplicated hypertension. Rather they consult it with village doctors, drug seller and registered physician. Moreover, they are using public health facilities like outdoor services of different tertiary care hospitals. But it is essential to get the proper management of hypertension in due time as this phenomenon usually comes with co-morbid diseases like diabetes mellitus, heart disease, renal disease and other vascular, endocrine and metabolic disorders. Understanding the recent trends of the prescription pattern can be used by Government to ensure supply of appropriate drugs and also helps proper management of subsidies. Therefore, the current study was carried out with an objective to evaluate the Pattern of Drugs prescribed for treatment of hypertensive patients.
MATERIALS AND METHODS
Ethical consideration
The researcher was duly concerned about the ethical issues related to the study. Formal ethical clearance was taken from the ethical review committee of the ASA University Bangladesh for conducting the study as well as formal permission was taken from the responders. Confidentiality was maintained properly. Informed written consent was taken from the subject informing the nature and purpose of the study, procedure of the study, the right to refuse, accept and withdraw to participate in the study as well as the participants did not gain financial benefit from this study. The present study posed a very low risk to the participants, as procedures such as medical treatments, invasive diagnostics or procedures causing psychological, spiritual or social harm were not included.
Design and subjects
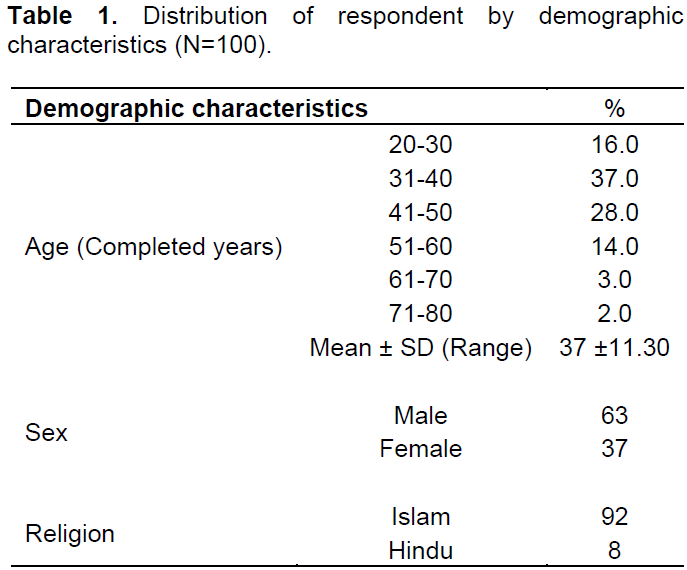
The current study was part of the Master of Public Health (MPH) thesis under the department of Public Health, ASA University Bangladesh. The descriptive, cross sectional study was conducted at Medicine Outpatient Department (OPD) of Dhaka Medical College Hospital (DMCH); which is a place where initial treatment is provided in hypertensive patients. Data were collected during the period of May 2015 to July 2015 from 100 patients by interviewing with a Bangla semi-structured questionnaire with non-probability purposive sampling. Patients suffering from hypertension above 20 years of age were included in the study. Participants, not willing to participate in the study and visited for the first time to the respective physician were excluded from the sample. After managing data properly it was analyzed in SPSS 16 version and Microsoft Excel Software 2007 version.
RESULTS
DISCUSSION
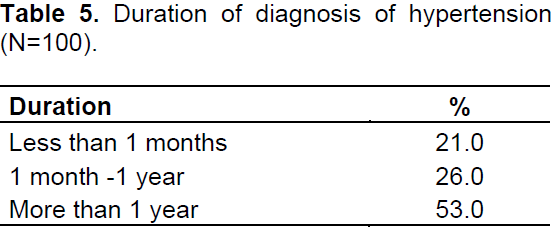
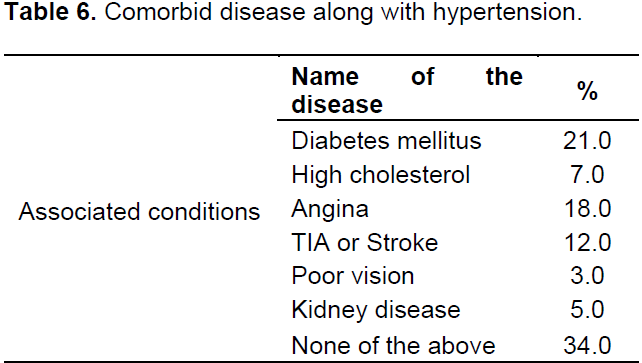
Hypertension has become a major health concern in low income countries. This study is one of the few studies that address the prescribing pattern of antihypertensive medications for the patients attending in outpatient department of Dhaka Medical College Hospital. We found an overall high prevalence of hypertension and low prevalence of awareness, treatment and control of the disease. The study highlighted mostly the hypertensive patients though different co morbid diseases like diabetes mellitus, angina, TIA/stroke, renal disease and others were also considered as associated conditions. This survey was conducted in a short period of three months and it is possible that since that time the prescribing pattern might have been changed. Among different classes of drugs most commonly used, drugs among single therapy were angiotensin receptor antagonist (37.3%), Calcium channel blocker (32.8%) and ACE inhibitor (17.9%) subsequently. Noticeably use of Beta blocker was very low (6%). Use of combination therapy for the management of hypertension was significantly high (38.4%) and most favorable combination chosen by the physicians were calcium channel blocker with beta blocker and angiotensin receptor blocker with calcium channel antagonist and both patterns were prescribed at almost equal rate (28.1%) among Bangladeshi people. 25% patients were prescribed angiotensin receptor blocker along with diuretics combination rather than isolated use of diuretics and centrally acting drug like methyldopa and alpha blocker.
Our finding is slightly different from the observation of drug prescribed for hypertension at primary health care facilities in Trinidad in respect of using ACE inhibitor (67.1%), Beta blocker (26.6%) and calcium channel blocker (14.3%) (Clement et al., 2012). Another finding was observed in the department of veterans affairs, United States of America (USA) where there was increased use of ACE inhibitor (range 28.95 to 38.3%), Beta blocker (range 19.9 to 28.6%), thiazide diuretics (range 11.2 to 16.5%), calcium channel blockers (range 20.1 to 28.1%) and angiotensin receptor blockers (range 1.5 to 5.5%)(Lopez et al., 2000). As the national hypertension management guidelines was not available so different experience physicians can also impact the choose of drug during prescription which may influence the prescription pattern and may linked to the slight difference of pattern from other studies.
In this study, 61.6% patients were prescribed single drug and 38.4% patients were prescribed combined therapy. Whereas, the combination therapy is the most prescribed pattern than mono therapy in Nigeria but male patients were more than female patients which is similar to other studies (Etuk et al., 2008). In this study, combination therapy were prescribed by the physicians about 39% and among them calcium channel antagonist along with beta blocker combination and angiotensin receptor blocker with calcium antagonist were equally chosen by physician and it is 28.1% whereas angiotensin receptor blocker and diuretics combination were preferred 25%. Isolated use of diuretics in combination therapy is significantly low about 3%. Use of monotherapy was more in the study as probably because of improper use of referral system of this country. Most of the people use the tertiary care hospital as a primary treatment centre and single drug therapy was prescribed to manage initial hypertension usually. It was interesting to note that less frequent use of thiazide diuretics in this study which is similar to other study particularly in uncomplicated hypertension though different guidelines suggest the use of thiazide diuretics (Petitti et al., 2006).
The present study represents the prescription pattern of the antihypertensive drugs used in hypertensive patients with associated diabetes mellitus, angina and stroke or TIA which is similar to different studies.
CONCLUSION
LIMITATIONS OF THE STUDY
ABBREVIATIONS
CONFLICT OF INTERESTS
ACKNOWLEDGEMENTS
REFERENCES
|
Alam DS, Chowdhury MAH, Siddiquee AT, Ahmed S, Niessen LW (2014). Awareness and control of hypertension in Bangladesh: follow-up of a hypertensive cohort. BMJ Open 4(12):e004983-e004983. |
|
|
Clement YN, Ali S, Harripaulsingh S, Lacaille K, Mohammed O, Mohammed S, Ragbir T, Ramirez E, Tshiamo K (2012). Prescripción de medicamentos para la hipertensión en los centros de atención primaria de lasalud en Trinidad. West Indian Med. J. 61(1):43-48. |
|
|
Etuk E, Isezuo SA, Chika A, Akuche J, Ali M (2008). Prescription pattern of anti-hypertensive drugs in a tertiary health institution in Nigeria. Ann. Afr. Med. 7(3):128-32. |
|
|
Lopez J, Meier J, Cunningham F, Siegel D (2000). Antihypertensive medication use in the Department of Veterans Affairs: a national analysis of prescribing patterns from 2000 to 2002. Am. J. Hypertens. 17(12 Pt 1):1095-1099. |
|
|
Majumder A (2012). Patterns of antihypertensive Drug Utilization among the Cardiologists of Bangladesh in Initiating Hypertension Treatment. Cardiovasc. J. 4(2):114-119. |
|
|
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Erdine S, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Lindholm LH, Viigimaa M, Adamopoulos S, Agabiti-Rosei E, Ambrosioni E, Bertomeu V, Clement D, Erdine S, Farsang C, Gaita D, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O'Brien E, Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P, Waeber B, Williams B (2007). Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 25(6):1105-1187. |
|
|
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G, Dominiczak A, Galderisi M, Grobbee DE, Jaarsma T, Kirchhof P, Kjeldsen SE, Laurent S, Manolis AJ, Nilsson PM, Ruilope LM, Schmieder RE, Sirnes PA, Sleight P, Viigimaa M, Waeber B, Zannad F, Redon J, Dominiczak A, Narkiewicz K, Nilsson PM, Burnier M, Viigimaa M, Ambrosioni E, Caufield M, Coca A, Olsen MH, Schmieder RE, Tsioufis C, van de Borne P, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Clement DL, Coca A, Gillebert TC, Tendera M, Rosei EA, Ambrosioni E, Anker SD, Bauersachs J, Hitij JB, Caulfield M, De Buyzere M, De Geest S, Derumeaux GA, Erdine S, Farsang C, Funck-Brentano C, Gerc V, Germano G, Gielen S, Haller H, Hoes AW, Jordan J, Kahan T, Komajda M, Lovic D, Mahrholdt H, Olsen MH, Ostergren J, Parati G, Perk J, Polonia J, Popescu BA, Reiner Z, Rydén L, Sirenko Y, Stanton A, Struijker-Boudier H, Tsioufis C, van de Borne P, Vlachopoulos C, Volpe M, Wood DA (2013). 2013 ESH/ESC guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 34(28):2159-219. |
|
|
Moniruzzamani AT, Rahmani S, Acharyyai A, Islami FA, Ahmedi MSAM, Zamanii MM (2013). Prevalence of hypertension among the Bangladeshi adult population: A meta-analysis. Regional Health Forum 17(1):15-19. |
|
|
Petitti DB, Xie F, Barzilay JI (2006). Prescribing patterns for thiazide diuretics in a large health maintenance organization: relationship to participation as an ALLHAT clinical center. Contemp. Clin. Trials 27(5):397-403. |
|
|
Rodgers A, Ezzati M, Vander Hoorn S, Lopez AD, Lin RB, Murray CJ (2004). Comparative Risk Assessment Collaborating Group. Distribution of Major Health Risks: Findings from the Global Burden of Disease Study. PLoS Med. 1(1):e27. |
|
|
Zaman M, Taleb A, Rahman S, Acharyya A, Islam FA, Ahmed MSAM, Zaman M (2011). SP1-112 Prevalence of hypertension among Bangladeshi adult population: a meta-analysis. J. Epidemiol. Commun. Health 65(Suppl 1):A405-A405. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


