ABSTRACT
Aqueous extract of Hibiscus sabdariffa L. is widely consumed in Nigeria as a local beverage used to quench thirst and also because of its antihypertensive action. The present study investigated the effect of consumption of aqueous extract of H. sabdariffa on thirst perception (TP) in mild to moderate hypertensive Nigerians. Fifty mild to moderate hypertensive patients attending medical out-patients clinic of Enugu State University Teaching Hospital were recruited for the study. They were randomly divided into two groups: A and B. Those in group A were given equivalent dose of placebo while group B received 150 mg/kg of H. sabdariffa daily for 4 weeks. All the subjects were given weekly appointments and a week worth of infusion. Thirst perception, serum electrolytes and blood pressure (BP) were measured at baseline and weekly during treatment. TP reduced significantly (p<0.001) in H. sabdariffa group compared to placebo throughout the duration of the experiment. Serum Na+ reduced significantly (p<0.001) in H. sabdariffa compared to placebo group in weeks 3 and 4. Blood pressure (SBP, DBP and MAP) also reduced significantly (p<0.001) in weeks 3 and 4. Thus, consumption of H. sabdariffa reduced thirst perception in mild to moderate hypertensive Nigerians. This validates its traditional use to ‘quench thirst’ and complements its antihypertensive action. Reduction in serum Na+ may be the possible mechanism of action.
Key words: Hibiscus sabdariffa, thirst perception, essential hypertension, serum electrolytes.
Thirst is important for maintaining body fluid homeostasis; it is a subjective perception that provides the urge for humans and animals to drink fluids. It is a component of the regulatory mechanisms that maintain body fluid
homeostasis and ultimately is essential for survival (McKinley and Johnson, 2004). Thirst is thought to be part of a corrective mechanism which acts as a support to the physiological control of fluid balance in the body. Thirst can also be a prominent symptom in diseases which disrupt fluid balance in the body.
The definition of thirst has been the subject of much debate, with major disagreement focusing on whether it is a local (for example, pharyngeal) or general sensation (Fitzsimons, 1972). Dryness of the mouth (DM) and throat region is a striking feature in thirst, and some have gone so far as to say that this feeling of dryness of mouth is an essential component of thirst, but very few claim that we drink when we are thirsty solely to abolish the disagreeable sensations that arise in the mouth when salivation is insufficient to keep the mouth and pharynx moist. The evidence being that the sensation of thirst and the sensation of dryness of the mouth could be dissociated from each other (Fitzsimons, 1972). Robertson (1984) defined thirst as ‘a generalized deep-seated feeling of a desire for water’. As thus defined, thirst is not synonymous with drinking, because drinking can be affected positively or negatively by a variety of factors such as personal and cultural factors. Also, this terminology is only appropriate for human studies as animals cannot report the sensation of thirst. Thirst is also defined as a conscious sensation of a need for water and a desire to drink (Robertson, 1991). Factors recognized as components of thirst include: body water deficit, brain integration of central and peripheral nerve messages relating to the need for water and an urge to drink.
Studies of thirst mechanism and dryness of mouth have been hampered by the lack of objective methods of quantification. Estimates of thirst and DM rely solely on the subject’s ability to perceive and to report the sensation. Sometimes one can check such information by observing the amount of water drunk spontaneously. A geometric rating scale was devised by Thompson and Campbell (1977) to quantify acute changes in thirst in controlled experimental settings.
Using this method, Robertson (1984) assessed the effects of osmotic stimuli on thirst mechanism and vasopressin secretion at various times during the infusion of hypertonic solution in healthy adults and reported that the osmotic threshold for the onset of thirst was 293.5 mOsm/Kg, which is approximately 10 mOsm/Kg above the osmotic threshold for vasopressin release.
Thompson et al. (1986) used a visual analogue scale (VAS) to study thirst ratings, subjects were allowed to define their own ratings before the experiment rather than be assigned to zero thirst ratings. Rolls et al. (1980) also explored the characteristics of osmotically induced thirst throughout a wider range of plasma osmolalities than previously examined. From linear regression analysis of their results, Rolls et al. (1980) concluded that the osmolar threshold for thirst onset (281 mOsm/Kg) is at the lower end of the physiological range of plasma osmolality and was much lower than that quoted in previous studies (Baylis and Robertson, 1980; Robertson, 1984). These workers also reported that thirst perception (TP) rises in a progressive fashion throughout a wide range of plasma osmolalities and that the osmolar threshold for thirst onset was similar to the theoretical osmolar threshold for vasopressin release (285 mOsm/ kg).
Circulating angiotensin II is known to play a role in thirst sensation. Animal experiments suggest that angiotensin II binds to the angiotensin type 1 receptor, stimulating thirst, sodium appetite and both arginine vasopressin (AVP) and oxytocin (OT) secretion (Felgendreger et al., 2012). Thirst perception in hypertensive patients is a topic that is currently receiving attention in order to determine the choice and benefits of antihypertensive drugs. Beverage prepared from Hibiscus sabdariffa is traditionally used to quench thirst in some countries including Nigeria and the antihypertensive activity of H. sabdariffa has been well documented (Adegunloye et al., 1996; Jonadet et al., 1990; Herrera-Arellano et al., 2004; Nwachukwu et al., 2015a). It has been shown that thirst ratings using the VAS are highly reproducible (Thompson et al., 1991), hence the present study assessed thirst perception in mild to moderate hypertensive Nigerians treated with aqueous extract of H. sabdariffa using this method.
Plant collection
Dried calyces of H. sabdariffa were purchased from Ogbete main market, Enugu. They were authenticated at the herbarium section of Botany Department, University of Nigeria, Nsukka and a specimen voucher number UNH/314b was assigned to it for future references.
Subjects
Fifty mild to moderate hypertensive subjects aged 35-60 years attending Medical Out-Patient (MOP) clinic of Enugu State University Teaching Hospital, Parklane, Enugu, were recruited for the study. They were randomly divided into 2 groups of 25 subjects per group. The study was carried out in line with the Guidelines of the Helsinki Declaration for human studies (as amended) and approved by the institutional ethics committee (ESUTTH/ EC/11002).
Inclusion criteria
(i) Newly diagnosed but untreated mild to moderate hypertension, using the WHO/ISH (1999/2003) classification of hypertension.
(ii) The subjects were properly briefed about the study and informed consent obtained.
Exclusion criteria
(i) Patients with diabetes, nephropathy, cardiopathy, hepatic disease and cancer were excluded from this study.
(ii) Pregnant women, individuals with evidence of secondary hypertension, chronic smokers and alcoholics were excluded.
(iii) Those who did not complete the study were also excluded.
Subjects who met the inclusion criteria were randomly divided into 2 groups: A and B.
Group A - Subjects were given equivalent dose (150 mg/kg) in volume of placebo taken orally before breakfast daily for 4 weeks. Blackcurrant (Glaxosmithkline®, UK) was used as placebo.
Group B- Subjects were given 150mg/kg of H. sabdariffa infusion orally once daily before breakfast for 4 weeks.
All the subjects were given weekly appointments and a week worth of infusion. Blood pressure, thirst perception and serum electrolytes were measured before and at weekly intervals for 4 weeks. Clinical evaluation and adherence to treatment were evaluated weekly. Additional measure was taken to monitor subjects in placebo group daily via phone calls.
Preparation of H. sabdariffa infusion
The method of Herrara- Arellano et al. (2004) was used with some modifications. 40 g of dry calyces of H. sabdariffa were weighed and ground in electric mill to obtain particles <2 mm. It was used to make an infusion by adding 2 L of boiling clean bottle water (Aquafina by Pepsi Nig. Ltd) and allowed to stand for 30 min. The solution was filtered using Whatman’s no.1 filter paper. The filtrates were stored in clean plastic containers at room temperature. The following modifications were made:
(i) Infusions were prepared and given to subjects.
(ii) Time allowed for extraction was extended from 10 to 30 min.
Placebo preparation
Blackcurrant (Glaxosmithkline®, UK) was diluted with clean bottle water (Aquafina, 7up bottling company Nig. Ltd) to obtain approximately the same colour as HS infusion.
HS dosage calculation
From extraction,
150 mg/kg was selected because it is far below the LD50 of HS (>5000 mg/kg) and similar dose has been used in a previous human study (Herrera-Arellano et al.,2004); this dose also produced approximately the same colour as the locally brewed HS (‘Zobo’) drink.
H. sabdariffa extract standardization
The H. sabdariffa extract was standardized using the colorimeter method of Fuleki and Francis (1958). This method was based on the ability of anthocyanin (a major active compound present in H. sabdariffa) to produce a color at pH 1.0 that disappears at pH 4.5. This special characteristic is produced by a pH dependent structural transformation of the chromophore. This method allows for fast and accurate determination of total anthocyanins, in spite of the presence of other compounds. The total anthocyanins concentration is obtained by using the formula:
Concentration (mg/ml) = A x MW x FD x 1000/ (Æ x 1).
(A= Absorbance of diluted sample; MW= Molecular weight of anthocyanin; FD= Dilution factor; Æ= Molar absorptivity). From this method, the total anthocyanin contained in 20 g of H. sabdariffa dissolved in 1 L was 10.04 mg.
Blood pressure
BP was measured by a physician who was not aware of the treatment group assigned to subjects. Two consecutive readings were taken from each subject at five minutes interval and the average of these was taken as the mean blood pressure reading. Measurement was taken between 8.00 am to 10.00 am.
Thirst perception (thirst ratings)
Thirst ratings were assessed in the subjects using the visual analogue scale (VAS) (Thompson et al., 1986). The scale is a marked but uncalibrated 10 cm vertical line with the top and base representing ‘very thirsty’ and ‘not thirsty’ respectively. The subjects were properly taught how to use the scale to estimate how thirsty they feel. They were later asked to respond to the question ‘How thirsty do you feel?’ by putting a mark on the line rating scale.
Serum electrolytes
Serum electrolytes (Na+, K+ and Cl−) were determined by ion selective electrode using Audicom automated electrolyte analyzer (AC9000 series) China.
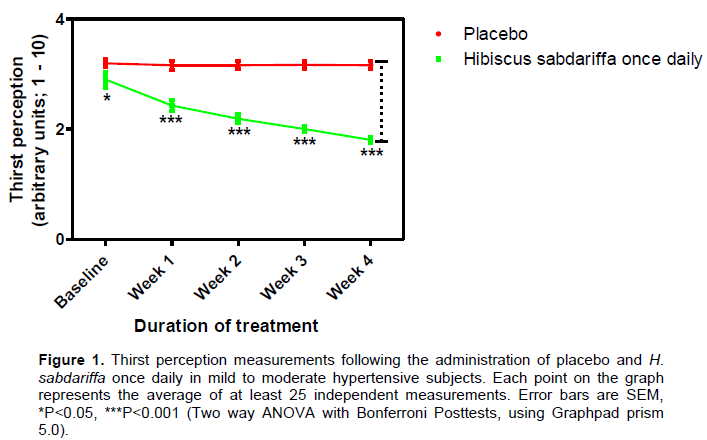
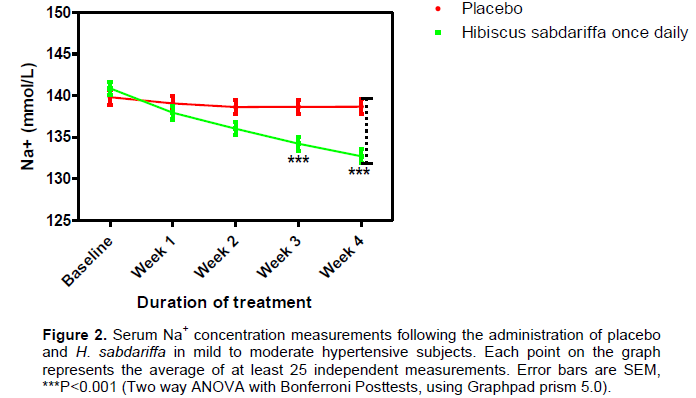
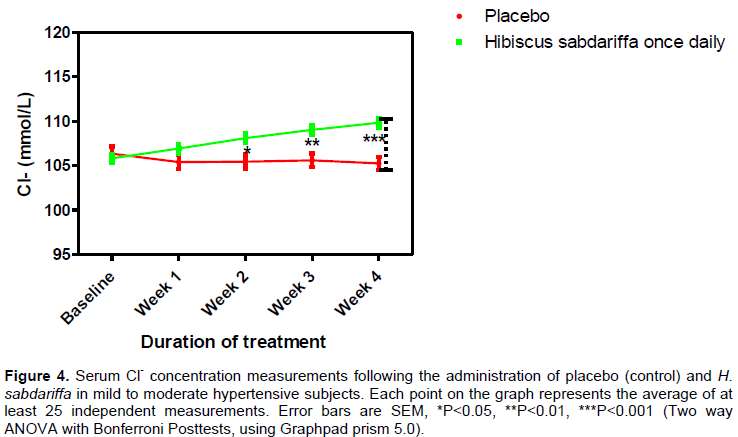
All the 50 subjects recruited completed the study. Thirst perception reduced significantly (p<0.001) in H. sabdariffa group compared to placebo from week 1 till the end of the study (Figure 1). Serum Na+ significantly reduced (p<0.001) at weeks 3 and 4 in H. sabdariffa group compared to placebo (Figure 2). In both groups, K+ did not differ significantly from baseline values but when compared to each other, K+ remained significantly lower (p<0.001) in H. sabdariffa group throughout the period of study (Figure 3). Conversely, a significant increase in serum Cl- was observed in H. sabdariffa group at weeks 3 (p<0.01) and 4 (p<0.001) (Figure 4).
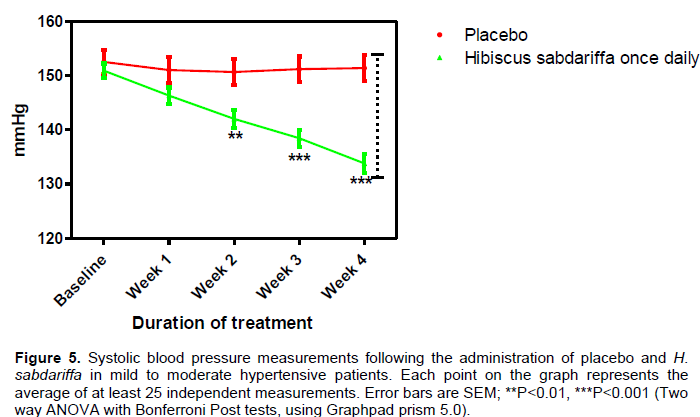
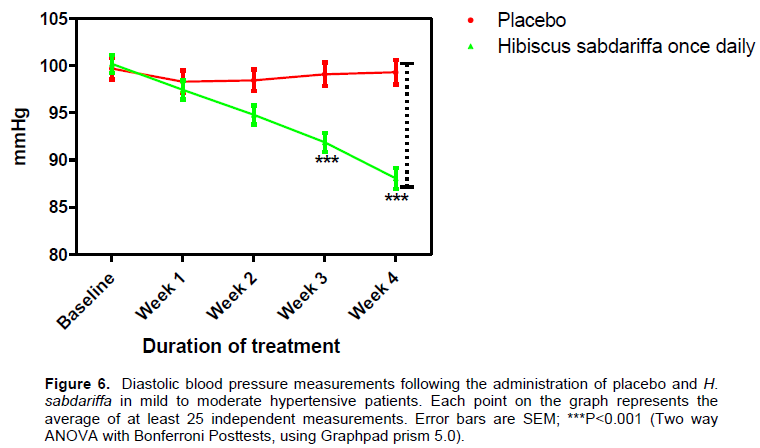
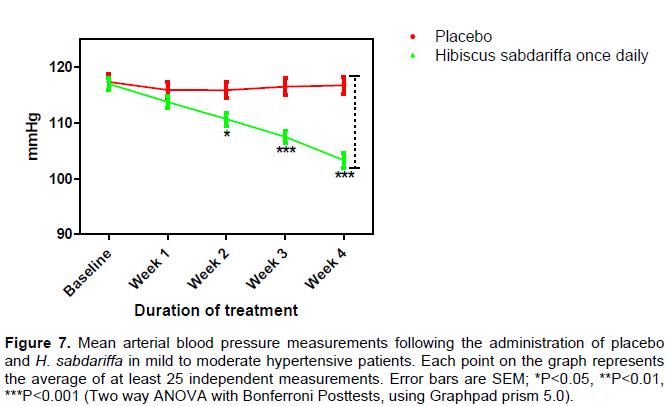
There was a significant reduction (p<0.001) in SBP (Figure 5), DBP (Figure 6) and MAP (Figure 7) in H. sabdariffa group compared to placebo at weeks 3 and 4 in H. sabdariffa group.
In the present study, a significant reduction in thirst perception was observed in the H. sabdariffa group. Similarly, a corresponding reduction in serum Na+ was also observed in this group. The physiological driving force behind the desire to drink liquid is the maintenance of blood osmolality. Sensory osmoreceptors in the lamina terminalis and other areas of the brain stimulate cortical effector regions, principally in the anterior cingulate cortex and insula, to trigger the sensation of thirst in response to a rise in blood osmolality (Farrell et al., 2011). The intensity of thirst and the amount of water required to quench it are directly proportional to blood osmolality.
The VAS may be susceptible to distortion by a variety of personal and cultural influences; this method however, provides the best available description of the function of the thirst mechanism so far (Robertson, 1984). Reduction in serum Na+ may reduce the osmolality of extracellular fluid (ECF) (Rasmussen et al, 2003) and invariably thirst perception. Conversely, reports from previous studies have shown that increase in plasma osmolality increased thirst in both animals (Sufit et al., 1985) and humans (Gordon et al., 1997). These workers attributed this to the physiologic role of Na+ balance through angiotensin II in the control of thirst. Sodium balance also plays a key role in the control of the renin-angiotensin system (Gordon et al., 1997) and H. sabdariffa has been shown to influence some basic components of the system in hypertensive subjects (Herrera-Arellano et al., 2004). Serum Na+ has been positively associated with blood pressure (Shailendra et al., 2011) and reduction in serum Na+ was earlier reported in hypertensive subjects after consumption of H. sabdariffa and was thought to be one of its anti-hypertensive mechanisms of action (Nwachukwu et al., 2015a).
Body fluid osmolality in humans is maintained between 280 and 295 mOsm/kg H2O, representing one of the most highly regulated parameters of body physiology. This is accomplished through an integration of thirst, arginine vasopressin (AVP) secretion, and renal responsiveness to AVP (Verbalis, 2007). Systemic osmoregulation is a vital process whereby changes in plasma osmolality, detected by osmoreceptors, modulate ingestive behaviour, sympathetic outflow and renal function to stabilize the tonicity and volume of the extracellular fluid. Change s in the central processing of osmosensory signals are likely to affect the hydro-mineral balance and other related aspects of homeostasis (Bourque, 2008). A rise in osmolality of blood will stimulate sensory osmoreceptors in the hypothalamus and other areas of the brain to create the sensation of thirst (Bourque, 2008; 2007; Farrell et al., 2011). Similarly, a fall in blood osmolality will reduce the stimulation of these receptors and thus the sensation of thirst. The reduction in serum Na+ (plasma volume) observed in the H. sabdariffa group in the present study was directly related to fall in thirst perception and thus justifies the traditional use of H. sabdariffa in certain countries including Nigeria to quench thirst (Adegunloye et al., 1996).
Hypertension has been positively correlated with thirst (Shailendra et al., 2011); it was reported to increase thirst perception (Stachenfeld, 2008), stimulate RAAS (Atlas, 2007) and alter sodium perception (Conlin et al., 1999). But H. sabdariffa consumption was reported to reduce plasma aldosterone level (Nwachukwu et al., 2015b) and exert antihypertensive action in humans (Herrea-Arellano et al., 2004; McKay et al., 2010). Decrease in plasma aldosterone was reported to cause natriuresis in normal humans (Gordon et al., 1997) and may be the mechanism responsible for the reduction in serum Na+ with a consequent reduction in plasma osmolality and thus thirst perception.
Consumption of H. sabdariffa reduced thirst perception in mild to moderate hypertensive Nigerians. This validates its traditional use to ‘quench thirst’ and complements its antihypertensive action. Reduction in serum Na+ may be the mechanism through which this is achieved.
We recommend further studies to investigate the mechanisms through which H. sabdariffa reduces thirst perception.
The authors have not declared any conflict of interests.
We wish to express our gratitude to the management of ESUT Teaching Hospital, Enugu, for allowing us to make use of their facility.
REFERENCES
|
Adegunloye BJ, Omoniyi JO, Owolabi OA, Ajagbonna OP, Sofola OA, Coker HA (1996). Mechanisms of the blood pressure lowering effect of the calyx extract of Hibiscus sabdariffa in rats. Afr. J. Med. Med. Sci. 25:235‑238.
|
|
|
|
Atlas SA (2007). The renin-angiotensin aldosterone system: pathophysiological role and pharmacologic inhibition. J. Manage. Care Pharm. 13(8 Suppl B):9-20.
Crossref
|
|
|
|
|
Baylis PH, Robertson GL (1980). Plasma Vasopressin Response to Hypertonic Saline Infusion to Assess Posterior Pituitary Function. J. R. Soc. Med. 73:255-260.
|
|
|
|
|
Bourque CW (2008). Central mechanism of osmosensation and systemic osmoregulation. Nat. Rev. Neurosci. 9(7):519-31.
Crossref
|
|
|
|
|
Conlin P, Moore T, Williams G, Hollenberg N (1999). Altered sodium perception in essential hypertensive patients following rapid volume expansion. J. Hum. Hypertens. 13(10):701-6.
Crossref
|
|
|
|
|
Farrell MJ, Bowala TK, Gavrilescu M, Phillips PA, McKinley MJ, McAllen RM, Denton DA, Egan GF (2011). Cortical activation and lamina terminalis functional connectivity during thirst and drinking in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 301(3):R623-31.
Crossref
|
|
|
|
|
Felgendreger LA, Fluharty SJ, Yee DK, Flanagan-Cato LM (2012). Endogenous angiotensin II-induced p44/42 MAPK activation mediates sodium appetite but not thirst or neurohypophysial secretion in male rats. J. Neuroendocrinol. 25(2):97.
Crossref
|
|
|
|
|
Fitzsimons JT (1972). Thirst. Physiol. Rev. 52:468-561.
|
|
|
|
|
Fuleki T, Francis FJ (1968). Quantitative methods of anthocyanins: Determination of total anthocyanin and degradation index for cranberry juice. J. Food Sci. 33:78‑83.
Crossref
|
|
|
|
|
Gordon MS, Majzoub JA, Williams GH, Gordon MB (1997). Sodium balance modulates thirst in normal man. Endocrinol. Res. 23(4):377-92.
Crossref
|
|
|
|
|
Herrera‑Arellano A, Flores‑Romero S, Chavez‑Soto MA, Tortoriello J (2004). Effectiveness and tolerability of a standardized extract from Hibiscus sabdariffa in patients with mild to moderate hypertension: A controlled and randomized clinical trial. Phytomedicine 11:375‑82.
Crossref
|
|
|
|
|
Jonadet M, Bastide J, Boyer B, Carnat AP, Lamaison JL (1980). In vitro enzyme inhibitory and in vivo cardioprotective activities of Hibiscus (Hibiscus Sabdariffa L.). Pharm. Belg. 45:120-1214.
|
|
|
|
|
McKay DL, Chen CY, Saltzman E, Blumberg JB (2010). Hibiscus sabdariffa L. tea (tisane) lowers blood pressure in prehypertensive and mildly hypertensive adults. J. Nutr. 140(2):298-303.
Crossref
|
|
|
|
|
McKinley MJ, Johnson AK (2004). The Physiological Regulation of Thirst and Fluid. News Physiol. Sci. 19(1):1-6.
Crossref
|
|
|
|
|
Nwachukwu DC, Aneke EI, Obika LFO, Nwachukwu NZ (2015a). Investigation of Antihypertensive Effectiveness and Tolerability of Hibiscus sabdariffa in Mild to Moderate Hypertensive Subjects in Enugu, South-east, Nigeria. Am. J. Phytomed. Clin. Ther. 3(4):339-345.
|
|
|
|
|
Nwachukwu DC, Aneke EI, Obika LF, Nwachukwu NZ (2015b). Effects of aqueous extract of Hibiscus sabdariffa on the renin-angiotensinaldosterone system of Nigerians with mild to moderate essential hypertension: A comparative study with lisinopril. Indian J. Pharmacol. 47:540-5.
Crossref
|
|
|
|
|
Rasmussen MS, Simonsen JA, Sandgaard NC, Høilund-Carlsen PF, Bie P (2003). Mechanisms of acute natriuresis in normal humans on low sodium diet. J Physiol. 3:15, 546(Pt 2):591-603.
|
|
|
|
|
Robertson GI (1991). Disorder of thirst in man. In: thirst physiology and psychological aspects (Eds: Ramsay DJ Broth DA), Springer Verlag, London. pp. 453-477.
Crossref
|
|
|
|
|
Robertson GL (1984). Abnormality of Thirst Regulation. Kidney Int. 25:460-469.
Crossref
|
|
|
|
|
Rolls BJ, Wood RJ, Roll ET, Lind H, Lind W, Ledingham JGG (1980). Thirst Following Water Deprivation in Humans. Am. J. Physiol. 239:R476-R482.
|
|
|
|
|
Shailendra KT, Bhanu PM, Ruchi T, Manish M, Kamlakar T (2011). Serum and urinary electrolytes level in the subjects of two different environmental conditions. J. Stress Physiol. Biochem. 7(1):20-26.
|
|
|
|
|
Stachenfeld NS (2008). Acute Effects of Sodium Ingestion on Thirst and Cardiovascular Function. Curr. Sports Med. Rep. 7(4Suppl):S7-13.
Crossref
|
|
|
|
|
Sufit E, Houpt KA, Sweeting M (1985). Physiological stimuli of thirst and drinking patterns in ponies. Equine Vet. J. 17(1):12-6.
Crossref
|
|
|
|
|
Thompson CJ, Bland J, Burd J, Bayliss PH (1986). The osmotic thresholds for thirst and vasopressin release are similar in healthy man. Clin. Sci. 71:651-656.
Crossref
|
|
|
|
|
Thompson CJ, Selby P, Baylis PH (1991). Reproducibility of Osmotic and Non-Osmotic Tests of Vasopressin Secretion in Man. Am. J. Physiol. 260:R533-R539.
|
|
|
|
|
Thompson DA, Campbell RG (1977). Hunger In Humans, Induced By 2-Deoxy- Glucose: Glucoprivic Control Of Taste Preference And Food Intake. Science 198:1065-1068.
Crossref
|
|
|
|
|
Verbalis JG (2007). How does brain sense osmolality? J. Am. Soc. Nephrol. 18(12):3056-3059.
Crossref
|
|
|
|
|
WHO/ISH (1999/2003). Statement on Hypertension. Management of Hypertension. J. Hypertens. 17:151-183.
|
|