Full Length Research Paper

ABSTRACT
This assessment aims to identify the increasing number of morbidity of drug susceptible tuberculosis (TB) and its treatment outcomes, government cost of medicines as well as the economic impact on society. A retrospective observational study had been conducted in a government hospital using a patient’s record from 2013 to 2017, treated under the Direct Observed Therapy Short Course (DOTS) program in Karachi, Pakistan. Altogether, 3872 drug-susceptible TB patients were included in the study. All data had been analyzed using SPSS version 16 software. It had been found from the data that each year number of new smear-positive TB patients remained same, that is, 85% in 2013, 90% in 2014, 89.5% in 2015, 91% in 2016 and 92.3% in 2017 while slight decrease in relapse cases, that is, 15, 10, 10.4, 9 and 7.6% in 2013 to 2017, respectively. The single factor analysis of variance (ANOVA) shows that there is no significant difference between the gender of TB patient throughout the duration with the p-value=0.3769. During the years of study, cost of medicine increased due to rapid rise of inflation in the region which inturn caused the significant financial constraint on patients and their families. moral and financial support are important to render an individual productive again in the society.
Key words: Drug-susceptible tuberculosis (DS-TB), anti-tubercular therapy, cost of medicine.
INTRODUCTION
Tuberculosis (TB) is leading infectious disease in developing countries which commonly affect a momentous number of populations. As per the global TB report of World Health Organisation (WHO) in 2018 an approximately 10.0 million (range, 9.0-11.1 million) people sufferered from TB (World Health Organization, 2019). Globally, TB is amongst the 10th most common cause of death (Pakistan Observer, 2017).
According to a global report of World Health Organization (WHO) in 2017, TB has been found to be the 9th primary cause of demises all over the world and the primary cause of a single infectious microorganism, standing above AIDS/HIV. In 2016, there had been an approximated 10.4 million people diagnosed with TB in which adults were 90%, male were 65%, 10% of people suffering were with HIV (74% in Africa) while 56% people had been found in 5 countries, that is, India, Indonesia, China, the Philippines, and Pakistan while in 2016, WHO African Region and WHO South-East Asia Region, the approximated death among HIV negative individuals from TB has been found to be 82% (World Health Organization, 2017).
WHO efforts associated to control and to lessen the pulmonary TB affirmed TB as a global emergency in the year 1993. This concluded that TB has been continuous as well as the main burden of mortality all over the world (De Muynck et al., 2001; National TB Control Programme, 2009; World Health Organization, 2009c). It has also been observed from Neolithic times that human beings had been plagued by TB. All over the world, TB has been a serious issue because it is one of the reasons for thousands of demises from centuries. In Europe, 25% of people had died during the 17 and 18th centuries because of Pulmonary TB. In a similar way, numerous areas in the US, that is, Texas, Louisiana, New York, New Jersey, California, Hawaii, and Alaska had been reported with maximum cases of pulmonary TB from the year 1986 to 1992 Cruz (2007). Likewise, the WHO report showed that during 2008, there had been approximately 9.4 million people recognized as the new cases of TB (World Health Organization, 2010a).
According to the WHO report, it had been found that several countries in Asia such as Bangladesh, Philippines, India, Indonesia, Pakistan, and China interpose 50% all new cases of Pulmonary TB (World Health Organization, 2006). In Pakistan, the pulmonary TB has been the main health issue, also recognized as the 4th primary cause of mortality (World Health Organization, 2009a; Yadav et al., 2012). By assessing WHO report of 2000, it has identified that TB has been a major and important disease in Karachi city particularly amongst the individuals who belong to poor and deprived families and believed as the chief reason of the demise of adults in malnourished societies. WHO has further recognized that Pakistan has been ranked 8th behind Bangladesh, India, Indonesia, and China as per the approximated number of cases of Pulmonary TB with an incidence of 175/100,000 persons (World Health Organization, 2003, 2009b). Furthermore, assessment of overall TB cases in twenty-three countries of Eastern Mediterranean Region (EMR), WHO stated that alone, Pakistan has been responsible for 44% of overall TB cases (World Health Organization, 2003). Reports showed that greater than 48000 Pakistanis died every year because of TB (The Express Tribune, 2011).
TB is very contagious, infectious as well as devastating disease carrying a greater incidence of mortality and morbidity. It is an airborne infection caused mycobacterium TB which is spread through the cough and sneeze of active TB patients (Mayoclinic, 2019).
Worldwide, the approximated number of new cases registered yearly was found to be 10.4 million patients with a mortality rate of approximated 1.4 million patients. In Pakistan, in the year 2016, approximated 510,000 patients had been diagnosed with TB with an incidence of 276/100,000. According to the latest global TB report 2016, Pakistan is among those thirty countries of the world which have high TB disease and a high Multi-Drug Resistant (MDR)-TB problem.
As stated by an official of National TB Control Program (NTP), an overall 10,000 patients of TB had been registered in thirty TB centers where financial support, free consultation, and medicines were provided to needy patients. Total 330,000 TB patients were registered however an approximated 600,000 individuals were suffering from TB within the country. In Pakistan, TB incidences per 100,000 populations have been approximately 181; and the reporting of cases is 150 per 100,000 per year, whereas the success rate of treatment is 85%. Above 700,000 patients of TB had been cured with free of cost while a hundred percent latest and updated Direct Observed Therapy Short Course (DOTS) treatment method is implemented within the country. (Pakistan Observer, 2017).
TB is the most far-reaching transmissible irresistible illness and still uncontrolled in numerous developing nations. Great adherence of the patient to the TB treatment regimens is the establishment stone to viable Anti Tubercular Therapy (ATT). Unfortunately, nonfulfillment or noncompliance is named as a key problem to the control of TB at public health level which aide to the resistance of drug in the treatment of TB (Khan et al., 2005; Lee and Chang, 2001).
MATERIALS AND METHODS
Research design
The study had been designed as a retrospective observational study using patient’s records from 2013 to 2017, treated in a DOTs program from tertiary care, teaching, a state-owned government hospital in Karachi.
Setting
Registered and treated patients of TB using established regimen advocated by WHO. New patients with smear-positive TB underwent category I treatment which comprises four-drug regimen in 2-month intensive phase treatment, that is, rifampicin, isoniazid, pyrazinamide, and ethambutol followed by 4-month continuous phase treatment which included 2 drugs, that is, rifampicin and isoniazid. If patients fail from category I treatment, then category II treatment had been given which include 2 months of intensive phase therapy, that is, rifampicin, isoniazid, pyrazinamide, and ethambutol followed by 4-month continuous phase treatment which included rifampicin, isoniazid, ethambutol and streptomycin injections.
Population
The study population consisted of all drug-susceptible TB patients treated in a DOTs program from a government hospital from January 2013 to December 2017 in Karachi.
Inclusion criteria
Patients diagnosed with drug-susceptible TB by legally qualified professionally competent authorized health care professional. No age limit restriction of patient.
Exclusion criteria
A patient diagnosed with multi-drug resistant TB that is, MDR-TB.
Collection of data and analysis
The patient data had been collected from one government hospital. Altogether 3872 DS-TB patients had been included in the study. Patient treatments cards as well as the TB register, had been inspected in order to file patient characteristics as well as treatment outcome. A record had been made of a type of TB, TB category and final treatment outcome by means of standardized definitions. Death had been described as death due to any reason during anti-TB treatment. The data collected included patient age and gender, treatment outcomes, newly registered cases and relapse cases of TB each year, government cost of ATT anti-TB therapy for both Category I and Category II DS-TB patients. The data were scrutinized for completeness and consistency, and all records were keyed in twice. A descriptive analytical approach had been used to examine the clinical administration and clinical results. All data had been analyzed using SPSS version 16 software.
RESULTS
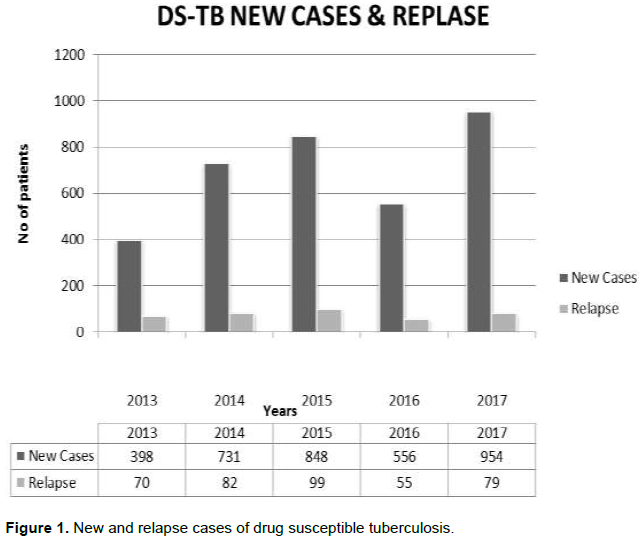
It had been found from data that each year number of new smear-positive TB patients remains same, that is, 85% in 2013, 90% in 2014, 89.5% in 2015, 91% in 2016 and 92.3% in 2017 while slight decrease in relapse cases, that is, 15% in 2013, 10% in 2014, 10.4% in 2015, 9% in 2016 and 7.6% in 2017 as shown in Figure 1.
Distributions of patients suffering from TB are high in the age group 15 to 34 years as shown in Table 1. The p-value of ANOVA: Single factor test shows that there is no significant difference between the gender of TB patient throughout the duration, that is, p-value is 0.3769 as shown in Table 2.

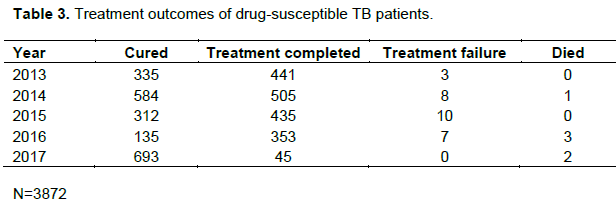
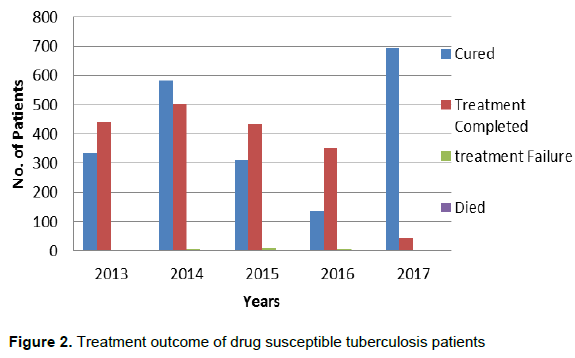
Table 3 and Figure 2 show the cured number of patients, died, failure and treatment completed while treatment completed term used for those patients who have completed treatment and bacteriological follow-up without evidence of failure but does not meet the cure definition due to the absence of bacteriological results.
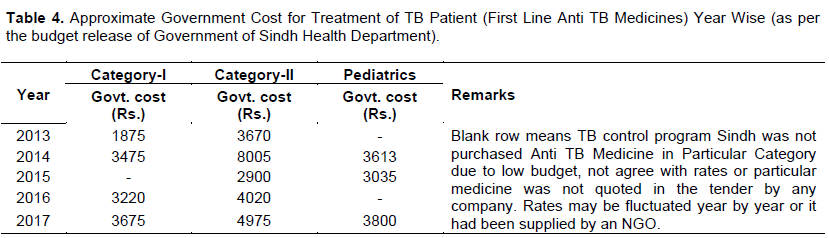
With the passage of time cost of medicine for both categories I and III patients there is an increase due to the rapid rise of inflation as shown in Table 4 where it only represents the cost of anti-tubercular medicine excluding laboratory cost for both categories I and II patients.


DISCUSSION
In Pakistan, TB has been one of the most widespread diseases and over 1.5 million individuals had been suffering from TB as it is considered the 2nd primary reason for death (World Health Organization, 2012; Yadav et al., 2012). It is widespread in Pakistan because of the lack of financial resourses by government as well as non-government organizations, lack of disease awareness as TB is highly contagious and implementation of new preventive, diagnostic and therapeutic measures in public health care setups (Simou and Koutsogeorgou, 2014). For controlling and eradicating disease, WHO plays a dynamic role and affirmed TB as a global emergency in the year 1993. For this purpose, NTP is established in 1995. National TB program is a national organization under the Ministry of Inter-Provincial Coordination (IPC) (National Tuberculosis Program (NTP) Pakistan, 2010). The 1st National TB program guidelines had been developed in the year 1995 in numerous regions of Pakistan, however, DOT policy had been instigated in year 1994 (Hussain et al., 2005).
More than 90% of TB cases had been found in developing countries in which 45% of total cases hold by Pakistan in EMR of World Health Organization. In order to decrease the burden of TB in the population of Pakistan, the government of Pakistan revised the allocation of fund to instigate DOT and affirmed it as “National Emergency” in the year 2002 because of these struggles Direct Observed Therapy Short Course outspread from 4% in 2002 to 50% in 2003 (National TB Control Programme Pakistan, 2004).
For complete remedy from TB, compliance is required from both patients and physicians. Explanation of symptoms is important to public health officials, clinician, and agencies which use symptom-based screening surveys to investigate for active TB.
TB occurs most commonly in economically valuable age of people, that is, from 15 to 54 years of age. 15 to 54 years age group faced the high expense and upraised the economic cost for society, which hinder the individual growth as well as the development of society (Rajeswari et al., 1999). Furthermore, most of the patients suffering from TB were working on daily wages which eventually leads to loss of income. Total cost is higher in uneducated patients as compared to patients with 10th years of education, that is, matric; this is because of the inadequate education of health regarding TB and its contagious nature of the disease (Ali et al., 2003). Economic burden of the disease pull an approximated hundred million people under the poverty line every year.
Moreover, recommended standard guidelines of pulmonary TB by World Health Organization comprises total 6 months course of treatment in which two months is initial phase (intensive phase) with daily four drugs regimen, comprising Isoniazid, Rifampicin, Pyrazinamide and Ethambutol, accompanied by four months continuous phase with two drugs including Isoniazid and Rifampicin for weekly three times (World Health Organization, 2009c).
The most frequently used drugs comprise Pyrazinamide, Isoniazid, Ethambutol, and Rifampicin whereas some other drugs that might be used to treat TB comprise Para-aminosalicylic acid, Ethionamide, Amikacin, Streptomycin, and Moxifloxacin (Wright et al., 2004). In Pakistan, evaluation of prescription of anti-TB drugs had been observed in numerous clinical studies, a study conducted in Northern area of Pakistan showed 80% physician noncompliance in duration (Akhtar et al., 1995)and unsuitable practice of prescribing for an extended duration (Shehzadi et al., 2005). Khan and Malik (2003) reported that only 73.3% of physicians who prescribed right recommended intensive phase drugs whereas 25.8% of physicians prescribed continuous phase drugs. The prescribing error of TB regimen leads to the development of resistance of anti-TB drugs and finally in the development of multi-drug resistant tuberculosis (MDR-TB) which causes a high economic impact on society.
The present study showed the cost of medicine supplied by the government for a TB control program in Sindh as shown in Table 4. Free of cost consultation as well as medicines are provided at TB, a center which shows access to patients in the National TB Program. One of the studies showed that the cost of treatment of pulmonary TB per case was Rs. 5100 cured in home-based supervision conducted in Sahiwal, Rawalpindi, Gujranwala city in Pakistan (Khan et al., 2002)and considered as the cost-effective treatment.
It has been found that 90% of mortality in developing nations happens because of pulmonary TB disease. South East Asia and sub-Saharan Africa identified as a high burden of TB disease. Therefore, the influences of pulmonary TB on the economy as well as economic efficiency are noteworthy that they frequently affect the adults (Global Tuberculosis Institute, 2012; World Health Organization, 2010b).
Furthermore, the pulmonary TB patients are prescribed medically to take rest, because they are affected financially. This practice not only impersonated the noteworthy economic influence on their families but also influenced the economic growth of national economies of the country because of their incompetence and lack of fitness to participate economically, as they are incapable to turn into useful workers. The pulmonary TB affects immune system as well as weaken body as such some individuals are unable to perform heavy labor and get exhausted quickly. In order to attain individual productivity again, financial and moral support are important (Kidder and Oppenheim, 2007; Langendam et al., 2011; Qayyum et al., 2010).
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Akhtar T, Safi MI, Ahmed N (1995). Management of Tuberculosis By Practitioners of Peshawar. Journal-Pakistan Medical Association 45(12):44-44. |
|
|
Ali S, Rabbani F, Siddiqui U, Zaidi A, Sophie A, Virani S, Younus N (2003). Tuberculosis: do we know enough? A study of patients and their families in an out-patient hospital setting in Karachi, Pakistan. The International Journal of Tuberculosis and Lung Disease 7(11):1052-1058. |
|
|
Cruz D (2007). Learning and Living in the 21st Century Iv for Hs' 2007. Ed: Rex Bookstore, Inc. |
|
|
De Muynck A, Siddiqi S, Ghaffar A, Sadiq H (2001). Tuberculosis control in Pakistan: critical analysis of its implementation. Journal of Pakistan Medical Association 51(1):41-47. |
|
|
Global Tuberculosis Institute (2012). A History of Tuberculosis Treatment. |
|
|
Hussain A, Mirza Z, Qureshi FA, Hafeez A (2005). Adherence of private practitioners with the National Tuberculosis Treatment Guidelines in Pakistan: A survey report. Journal of Pakistan Medical Association 55(1):17-19. |
|
|
Khan J, Malik A (2003). Tuberculosis in Pakistan: are we losing the battle? Journal-Pakistan Medical Association 53(8):320-320. |
|
|
Khan M, Walley J, Witter S, Imran A, Safdar N (2002). Costs and cost-effectiveness of different DOT strategies for the treatment of tuberculosis in Pakistan. Health Policy and Planning 17(2):178-186. |
|
|
Khan M, Walley J, Witter S, Shah S, Javeed S (2005). Tuberculosis patient adherence to direct observation: Results of a social study in Pakistan. Health Policy and Planning 20(6):354-365. |
|
|
Kidder DS, Oppenheim ND (2007). The Intellectual Devotional: Revive Your Mind, Complete Your Education, and Roam Confidently with the Culture d Class: Rodale Books. |
|
|
Langendam MW, van der Werf MJ, Huitric E, Manissero D (2012). Prevalence of inappropriate tuberculosis treatment regimens: A systematic review. European Respiratory Journal 39(4):1012-1020. |
|
|
Lee JH, Chang JH (2001). Drug-resistant tuberculosis in a tertiary referral teaching hospital of Korea. The Korean Journal of Internal Medicine 16(3):173. |
|
|
Mayoclinic (2019). Tuberculosis symtoms and causes. |
|
|
National TB Control Program me; Ministry of Health (2009). Strengthening Public Private Partnership 500,000 Young People Mobilized On World TB Day. |
|
|
National TB control Program Pakistan (2004). 10:1. |
|
|
National Tuberculosis Program Pakistan (NTP)., About NTP. (2010). |
|
|
Pakistan Observer (2017). 119 TB treatment centres functioning across country. Pakistan Observer. |
|
|
Qayyum S, Ahmed I, Ansari G (2010). Comparing Daily Versus partially Intermittent Regimen of ATT in non HIV patients with new Pulmonary Tuberculosis (TB) in DOTS program. |
|
|
Rajeswari R, Balasubramanian R, Muniyandi M, Geetharamani S, Thresa X, Venkatesan P (1999). Socio-economic impact of tuberculosis on patients and family in India. The International Journal of Tuberculosis and Lung Disease 3(10):869-877. |
|
|
Shehzadi R, Irfan M, Zohra T, Khan JA, Hussain SF (2005). Knowledge regarding management of tuberculosis among general practitioners in northern areas of Pakistan. JPMA. The Journal of the Pakistan Medical Association 55(4):174-176. |
|
|
Simou E, Koutsogeorgou E (2014). Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy 115(2-3):111-119. |
|
|
The Express Tribune (2011). Pakistan ranks sixth in TB patients: WHO. |
|
|
World Health Organization (WHO) (2003). Country Profile: Pakistan, Global Tuberculosis Control WHO Report pp. 99-101. |
|
|
World Health Organization (WHO) (2006). Tuberculosis Facts. Retrieved from WHO/HTM/STB/factsheet/2006.1 |
|
|
World Health Organization (WHO) (2009a). Global Tuberculosis control. |
|
|
World Health Organization (WHO) (2009b). Global Tuberculosis control. |
|
|
World Health Organization (WHO) (2009c). Global tuberculosis control: epidemiology, strategy, financing: WHO report 2009: World Health Organization. |
|
|
World Health Organization (WHO) (2010a). Global Tuberculosis Control: Surveillance, Planning, Financing. |
|
|
World health organization (WHO) (2010b). Treatment of Tuberculosis-Guidelines. 4th. |
|
|
World Health Organization (WHO) (2012). Global Tuberculosis Report. |
|
|
World Health Organization (WHO) (2017). Executive Summary. |
|
|
World Health Organization (WHO) (2019). Executive summary of global report |
|
|
Wright J, Walley J, Philip A, Pushpananthan S, Dlamini E, Newell J, Dlamini S (2004). Direct observation of treatment for tuberculosis: A randomized controlled trial of community health workers versus family members. Tropical Medicine and International Health 9(5):559-565. |
|
|
Yadav A, Garg S, Chopra H, Bajpai S, Bano T, Jain S, Kumar A (2012). Treatment practices in pulmonary tuberculosis by private sector physicians of Meerut, Uttar Pradesh. Indian Journal of Chest Diseases and Allied Sciences 54(3):161. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


