Full Length Research Paper

ABSTRACT
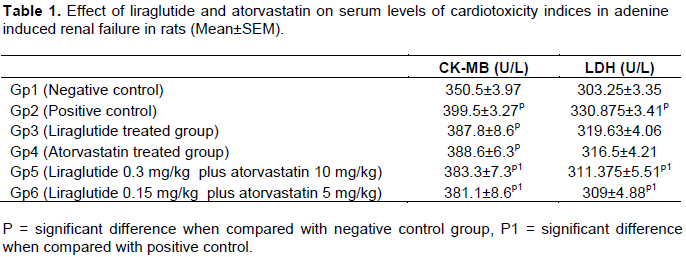
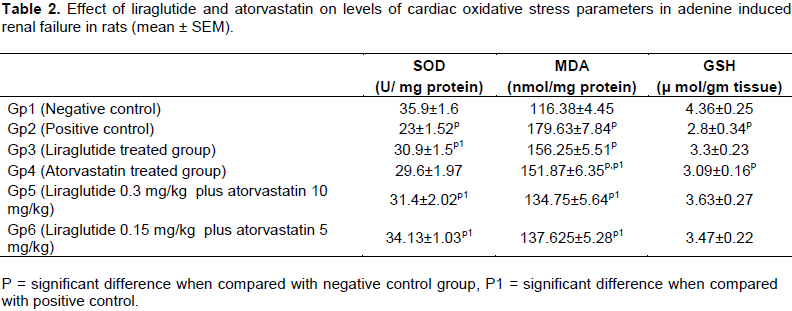
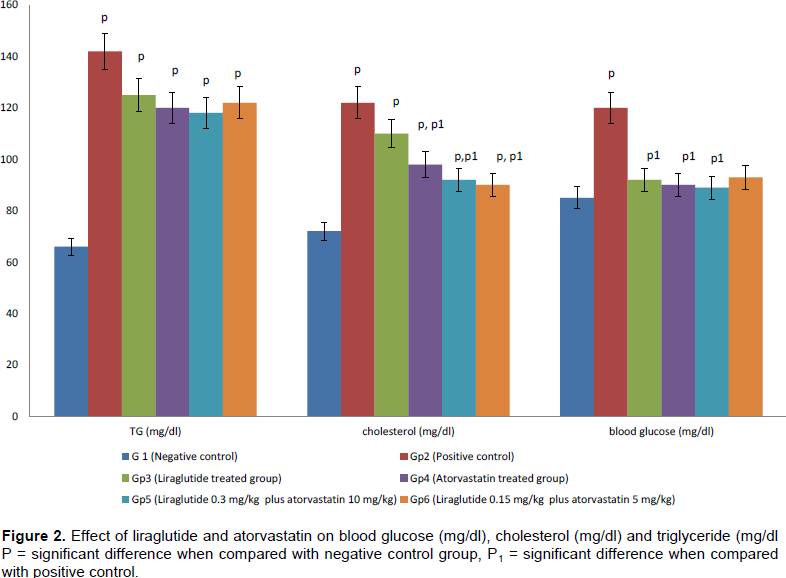
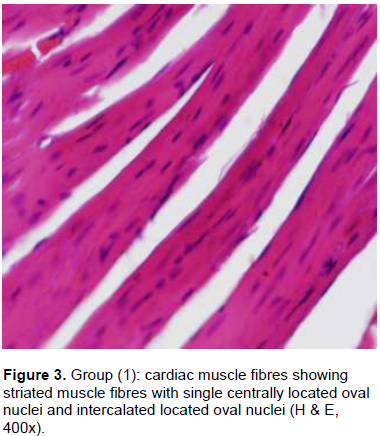
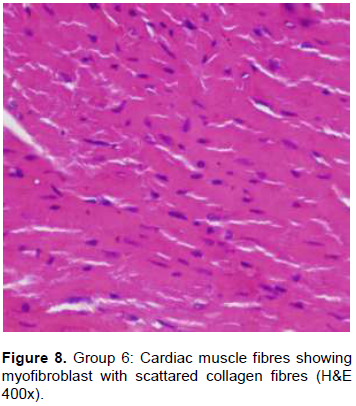
The prevalence of cardiovascular changes markedly increases with deterioration of patient's renal function and can stack up 65 to 70% in end-stage renal disease. A rapid fall in renal function is often associated with uncontrolled congestive heart failure. Beyond their lipid-lowering effect, statins have been shown to protect the heart in different diseases. Liraglutide is a glucagon-like peptide-1 (GLP-1) analogue, used to control diabetes. It improves cardiac dysfunction in non-diabetics, but underlying mechanisms remain to some extent, unclear. Fifty two male Sprague-Dawley rats weighing 200 to 250 g were grouped into negative control, positive control, liraglutide treated group (0.3 mg/kg), atorvastatin treated group (10 mg/kg), liraglutide and atorvastatin treated group (0.3 and 10 mg/kg, respectively), liraglutide and atorvastatin treated group (0.15 and 5 mg/kg, respectively). Combination of both drugs significantly reduce creatine phosphokinase isoenzyme (CK-MB) in both doses (p<0.008, p <0.002) and lactate dehydrognase (LDH) (p<0.04, p<0.01). Liraglutide alone or in combination with atorvastatin in both doses (p<0.02, p<0.01 and p<0.01) significantly increased superoxide dismutase (SOD). Atorvastatin alone (p<0.02) or in combination with liraglutide in both doses (p<0.001, p<0.001) induced a significant decrease of malondialdehyde (MDA). Atorvastatin alone (p<0.01) or in combination with liraglutide in both doses induced a significant amelioration of nitric oxide (NO) and cholesterol (p<0.01 and p<0.02). Significant improvements in blood urea nitrogen (BUN) and glucose profile were seen with all tested drugs either single or in combination. Combined implementation of both drugs improves histopathological changes of cardiac muscle fibres. Liraglutide has promising effects on cardiovascular changes in adenine induced chronic nephropathy through modulation of LDH, CK-MB and improvement of NO and SOD. Also, it can mitigate fibrosis and cardiac tissue changes. Its effects markedly increase in conjunction with atorvastatin. Combined administration of liraglutide and atorvastatin in a high dose has a reliable effect on improving outcome in biochemical and histopthological cardiac muscle fibers changes.
Key word: Atorvastatin, liraglutide, adenine, renal failure.
INTRODUCTION
MATERIALS AND METHODS
RESULTS


DISCUSSION
CONCLUSION
CONFLICT OF INTEREST
REFERENCES
|
Adachi Y, Sasagawa I, Nakada T (1993). Reproductive insufficiency in the male rat with adenine-induced chronic renal failure. Urol. Int. 51(4):228-230. |
|
Al Za'abi M, Al Busaidi M, Yasin J, Schupp N Nemmar A, Ali BH (2015). Development of a new model for the induction of chronic kidney disease via intraperitoneal adenine administration, and the effect of treatment with gum acacia thereon. Am. J. Transl. Res. 7(1):28-38. |
|
Amano F, Noda T (1995). Improved detection of nitric oxide radical (NO) production in an activated macrophage culture with a radical scavenger, carboxy and Griess reagent. FEBS. Lett. 368(3):425-428. |
|
An Z, Yang G, He YQ, Dong N, Ge LL, Li SM, Zhang WQ (2013). Atorvastatin reduces myocardial fibrosis in a rat model with post-myocardial infarction heart failure by increasing the matrix metalloproteinase-2/tissue matrix metalloproteinase inhibitor-2 ratio. Chin. Med. J. (Engl). 126(11):2149-2156. |
|
Bancroft JD, Gamble M (2002). Theory and practice of histological techniques.5th. Ed. Edinburgh. Churchill Livingstone Publication. pp. 172-175, 593-620. |
|
Bernheim F, Bernhiem ML, Wilbur KM (1948). The reaction between TBA and the oxidation products of certain lipids. Biol. Chem. 174:257-264. |
|
Beutler E, Duron O, Kelly BM (1963). Improved method for the determination of blood glutathione. J. Lab. Clin. Med. 61: 882-888. |
|
Cámara-Lemarroy CR, Guzmán-de la Garza FJ, Alarcón-Galván G, Cordero-Pérez P, Mu-oz-Espinosa L, Torres-González L, Fernández-Garza NE (2014). Hepatic ischemia/reperfusion injury is diminished by atorvastatin in Wistar rats. Arch. Med. Res. 45(3):210-216. |
|
Cetinkaya DB, Uyar Y, Ozbilgin K, Köse C (2013). Effect of raloxifene and atorvastatin in atherosclerotic process in ovariectomized rats. J. Obstet. Gynaecol. Res. 39(1):229-236. |
|
Chang CZ, Wu SC, Lin CL, Hwang SL, Howng SL, Kwan AL (2010). Atorvastatin preconditioning attenuates the production of endothelin-1 and prevents experimental vasospasm in rats. Acta Neurochir. 152(8):1399-1406. |
|
Dai Y, Mehta JL, Chen M (2013). Glucagon-like peptide-1 receptor agonist liraglutide inhibits endothelin-1 in endothelial cell by repressing nuclear factor-kappa B activation. Cardiovasc. Drugs Ther. 27(5):371-380. |
|
Deshmukh HA, Colhoun HM, Johnson T, McKeigue PM, Betteridge DJ, Durrington PN, Fuller JH, Livingstone S, Charlton-Menys V, Neil A, Poulter N, Sever P, Shields DC, Stanton AV, Chatterjee A, Hyde C, Calle RA, Demicco DA, Trompet S, Postmus I, Ford I, Jukema JW, Caulfield M, Hitman GA (2012). Genome-wide association study of genetic determinants of LDL-c response to atorvastatin therapy: importance of Lp (a). J. Lipid Res. 53(5):1000-1011. |
|
El Rabey HA, Al-Seeni MN, Amer HM (2013). Efficiency of Barley Bran and Oat Bran in Ameliorating Blood Lipid Profile and the Adverse Histological Changes in Hypercholesterolemic Male Rats. J. Biomed Res. Int. 1:1155-1166. |
|
Farag MM, Mohamed MB, Youssef EA (2015). Assessment of hepatic function, oxidant/antioxidant status, and histopathological changes in rats treated with atorvastatin: Effect of dose and acute intoxication with acetaminophen. Hum. Exp. Toxicol. 34(8):828-837. |
|
Fossati P, Principe M (1982). Serum triglycerides determined colorimetrically with an enzyme that produces hydrogen peroxide. Clin. Chem. 28:2077-2080. |
|
Gao H, Zeng Z, Zhang H, Zhou X, Guan L, Deng W, Xu L (2015). The Glucagon-Like Peptide-1 Analogue Liraglutide Inhibits Oxidative Stress and Inflammatory Response in the Liver of Rats with Diet-Induced Non-alcoholic Fatty Liver Disease. Biol. Pharm. Bull. 38(5):694-702. |
|
Gundapaneni KK, Shyamala N, Galimudi RK, Sahu SK, Hanumanth SR (2016). A Therapeutic Effect of Atorvastatin on Genetic Damage in Coronary Artery Disease. J. Clin. Diagn. Res. 10(6):28-30. |
|
Halbirk M, Nørrelund H, Møller N, Holst JJ, Schmitz O, Nielsen R, Nielsen-Kudsk JE, Nielsen SS, Nielsen TT, Eiskjaer H, Bøtker HE, Wiggers H (2010). Cardiovascular and metabolic effects of 48-h glucagon-like peptide-1 infusion in compensated chronic patients with heart failure. Am. J. Physiol. Heart Circ. Physiol. 298(3):H1096-H1102. |
|
Henry RJ (1974). Clinical chemistry: principles and techniques. 2nd ed. NY: Harper and Row. |
|
Hernández-Reséndiz S, Correa F, García-Ni-o, WR, Buelna-Chontal M, Roldán FJ, Ramírez-Camacho I, Delgado-Toral C, Carbó R, Pedraza-Chaverrí J, Tapia E, Zazueta C (2015). Cardio-protection by curcumin post-treatment in rats with established chronic kidney disease. Cardiovasc. Drugs Ther. 29(2):111-120. |
|
Hou J, Manaenko A, Hakon J, Hansen-Schwartz J, Tang J, Zhang JH (2012). Liraglutide, a long-acting GLP-1 mimetic, and its metabolite attenuate inflammation after intracerebral hemorrhage. J. Cerebral Blood Flow Metab. 32(12):2201-2210. |
|
Inoue T, Inoguchi T, Sonoda N, Hendarto H, Makimura H, Sasaki S, Yokomizo H, Fujimura Y, Miura D, Takayanagi R (2015). GLP-1 analog liraglutide protects against cardiac steatosis, oxidative stress and apoptosis in streptozotocin-induced diabetic rat. Atherosclerosis 240(1):250-259. |
|
John S, Schneider MP, Delles C, Jacobi J, Schmieder RE (2005). Lipid-independent effects of statins on endothelial function and bioavailability of nitric oxide in hypercholesterolemic patients. Am. Heart J. 149(3):473. |
|
Kiernan JA (1999). Histological and Histochemical Methods Theory and practice (3rd). Arnold, A member of the hodder. Headline Group. London. New York and New Delhi. |
|
Kucera M, Oravec S, Hirnerova E, Huckova N, Celecova Z, Gaspar L, Banach M (2014). Effect of atorvastatin on low-density lipoprotein subpopulations and comparison between indicators of plasma atherogenicity a pilot study. Angiology 65(9):794-799. |
|
Liao D, Liu YQ, Xiong LY, Zhang L (2016). Renoprotective effect of atorvastatin on STZ-diabetic rats through inhibiting inflammatory factors expression in diabetic rat. Eur. Rev. Med. Pharmacol. Sci. 20(9):1888-1893. |
|
Liu J, Liu Y, Chen L, Wang Y, Li J (2013). Glucagon-Like Peptide-1 Analog Liraglutide Protects against Diabetic Cardiomyopathy by the Inhibition of the Endoplasmic Reticulum Stress Pathway. J. Diabetes Res. 2013:630537. |
|
Liu XY, Wang LX, Chen Z, Liu LB (2016). Liraglutide prevents beta-amyloid-induced neurotoxicity in SH-SY5Y cells via a PI3K-dependent signaling pathway. Neurol. Res. 38(4):313-319. |
|
Lowry OH, Rosenbrough NJ, Farr AL, Randall RJ (1955). Protein measurement with the Folin-phenol reagent. J. Biol. Chem. 193:265-275. |
|
Mehrzadi S, Kamrava SK, Dormanesh B, Motevalian M, Hosseinzadeh A, Hosseini Tabatabaei SM, Ghaznavi H (2016). Melatonin synergistically enhances protective effect of atorvastatin against gentamicin-induced nephrotoxicity in rat kidney. Can. J. Physiol. Pharmacol. 94(3):265-271. |
|
Nakata S, Tsutsui M, Shimokawa H, Yamashita T, Tanimoto A, Tasaki H, Ozumi K, Sabanai K, Morishita T, Suda O, Hirano H, Sasaguri Y, Nakashima Y, Yanagihara N (2007). Statin treatment upregulates vascular neuronal nitric oxide synthase through Akt/NF-kappaB pathway. Arterioscler. Thromb. Vasc. Biol. 27(1):92-98. |
|
Nikolaidis L, Elahi D, Shen Y, Shannon RP (2005). Active metabolite of GLP-1 mediates myocardial glucose uptake and improves ventricular performance in conscious dogs with dilated cardiomyopathy. Am. J. Physiol. Heart Circ. Physiol. 289(6):H2401-H2408. |
|
Noyan-Ashraf MH, Shikatani EA, Schuiki I, Mukovozov I, Wu J, Li RK, Volchuk A, Robinson LA, Billia F, Drucker DJ, Husain M. (2013). Glucagon-Like Peptide-1 Analog Reverses the Molecular Pathology and Cardiac Dysfunction of a Mouse Model of Obesity. Circulation 127(1):74-85. |
|
Patton CJ, Crouch SR (1977). Spectrophotometric and kinetic investigation of the Berthelot reaction for the determination of ammonia. Anal. Chem. 49:464-469. |
|
Poornima I, Brown SB, Bhashyam S, Parikh P, Bolukoglu H, Shannon RP (2008). Chronic glucagon-like peptide-1 infusion sustains left ventricular systolic function and prolongs survival in the spontaneously hypertensive, heart failure-prone rat. Circ. Heart Fail. 1(3):153-160. |
|
Serizawa K, Yogo K, Tashiro Y, Aizawa K, Kawasaki R, Hirata M, Endo K (2015). Epoetin beta pegol prevents endothelial dysfunction as evaluated by flow-mediated dilation in chronic kidney disease rats. Euro. J. Pharmacol. 767:10-16. |
|
Sharma MK, Jalewa J, Hölscher C (2014). Neuroprotective and anti-apoptotic effects of liraglutide on SH-SY5Y cells exposed to methylglyoxal stress. J. Neurochem. 128(3):459-471. |
|
Sokos GG, Nikolaidis LA, Mankad S, Elahi D, Shannon RP (2006). Glucagon-like peptide-1 infusion improves left ventricular ejection fraction and functional status in patients with chronic heart failure. J. Card. Fail. 12(9): 694-699. |
|
Sun G, Li Y, Ji Z (2015). Atorvastatin attenuates inflammation and oxidative stress induced by ischemia/reperfusion in rat heart via the Nrf2 transcription factor. Int J ClinExp Med. Sep 15;8(9): 14837-1445. |
|
Suzuki N, Matsumoto H, Kitada C, Kimura S, Fujino M (1989). Production of endothelin-1 and big-endothelin-1 by tumor cells with epithelial-like morphology. J. Biochem. 106:736-741. |
|
Thaung HP, Yao Y, Bussey CT, Hughes G, Jones PP, Bahn A, Sammut IA, Lamberts RR (2015). Chronic bilateral renal denervation reduces cardiac hypertrophic remodelling but not β-adrenergic responsiveness in hypertensive type 1 diabetic rats. Exp. Physiol. 100(6):628-639. |
|
Tietz NW (1976). Fundamental of clinical chemistry. W. B. Saunders, Philadelphia. P 633. |
|
Trinder P (1969). Enzymatic colorimetric method for glucose determination. Ann. Clin. Biochem. 6:24-27. |
|
Wang CY, Liu PY, Liao JK (2008). Pleiotropic effects of statin therapy: molecular mechanisms and clinical results. Trends Mol. Med.14:37-44. |
|
Wang YG, Yang TL (2015). Liraglutide reduces oxidized LDL-induced oxidative stress and fatty degeneration in Raw 264.7 cells involving the AMPK/SREBP1 pathway. J. Geriatr. Cardiol. 12(4):410-416. |
|
Yokozawa T, Zheng PD, Oura H, Koizumi F (1986). Animal model of adenine induced chronic renal failure in rats. Nephron, 44:230-234. |
|
Zhang K, He X, Zhou Y, Gao L, Qi Z, Chen J, Gao X (2015). Atorvastatin Ameliorates Radiation-Induced Cardiac Fibrosis in Rats. Radiat. Res. 184(6):611-620. |
|
Zhang LH, Pang XF, Bai F, Wang NP, Shah AI, McKallip RJ, Li XW, Wang X, Zhao ZQ (2015). Preservation of Glucagon-Like Peptide-1 Level Attenuates Angiotensin II-Induced Tissue Fibrosis by Altering AT1/AT 2 Receptor Expression and Angiotensin-Converting Enzyme 2 Activity in Rat Heart. Cardiovasc. Drugs Ther. 29(3):243-255. |
|
Zhou S, Zhao P, Li Y, Deng T, Tian L, Li H (2014). Renoprotective effect of atorvastatin on STZ-diabetic rats through attenuating kidney-associated dysmetabolism. Euro. J. Pharmacol. 5(740):9-14. |
|
Zhou SJ, Bai L, Lv L, Chen R, Li CJ, Liu XY, Yu DM, Yu P (2014). Liraglutide ameliorates renal injury in streptozotocin induced diabetic rats by activating endothelial nitric oxide synthase activity via the downregulation of the nuclear factor κB pathway. Mol. Med. Rep. 10(5):2587-2594. |
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


