Full Length Research Paper

ABSTRACT
Over a decade, different stakeholders have engaged concerted efforts to reduce morbidity and mortality related to asthma. Despite all these efforts, substantial proportions of asthmatic patients do not achieve proper asthma control. The aim of this study was to evaluate the level of asthma control and to assess the factors that might influence control of the disease. The study was conducted at the Ambo University Referral Hospital which is allied with College of Medicine and Health Sciences, Ambo University and serve for a training center for postgraduates and undergraduate medical and health sciences students. The study was conducted from February to March 2019 on a sample of 82 asthmatic patients. The dependent variable was asthma disease control, according to the Global Initiative for Asthma criteria. Accordingly, patients were classified into three classes; controlled, partially controlled and uncontrolled asthma. Binary logistic regression analysis was used to determine factors associated with the poor asthma control. The results were represented as percentages in valid results. Continuous variables were represented as a mean and standard deviation (SD). The level of asthma disease control and analysis of factors associated with poor asthma control was the main outcome measure. Results revealed that a total of 82 asthmatic patients with a mean age (standard deviation [SD]) of 44.9 ± 8.9 of years were participating in the study. Only 23.2% of patients were controlled, 2.4% had partial control and 74.4% were poorly controlled. Large proportions of patients (89.02%) recruited were treated with short acting beta agonists (SABA) plus medium/high daily doses of corticosteroids.In multivariate analysis, patients having concomitant allergic rhinitis (Adjusted odds ratio= AOR: 7.87; 95% CI [1.13 - 11.75]) and chronic sinus (AOR: 13.31; 95% CI [1.57-17.40]), not used ICS (AOR: 4.45; 95% CI [1.17-9.94]) and female sex (AOR: 3.26; 95% CI [0.87-6.20]) had increased odds of uncontrolled asthma with p-value of <0.05. Thus, large proportions of patients had poorly controlled asthma. Female sex, unused inhalational corticosteroids, co-morbidities like allergic rhinitis and sinusitis significantly increased the odds of having uncontrolled asthma.
Key words: Asthma, level of asthma control, determinants, Ambo University Referral Hospital.
Abbreviation: AURH, Ambo University Referral Hospital; GINA, Global Initiative for Asthma; ICS, Inhalational corticosteroids.INTRODUCTION
The Global Initiative for Asthma (GINA) (GINA, 2018)describes asthma as “a heterogeneous disease, usually characterized by chronic airway inflammation.” According to the Global Asthma Report 2018, about 339 million asthma patients. It causes a high global burden of deaths and disability, with around 1000 people dying from asthma and is in the top 20 causes of years of life lived with a disability (Global Asthma Network, 2018). It is estimated that asthma costs $USD 1,900 in Europe and $USD 3, 100 in USA (Nocon and Booth, 1991; Godard et al., 2002; Smith et al., 2005; CDC, 2010; Akinbami et al., 2012; Nunes et al., 2018).
Over the past three decades, governments, health services, and allied researchers have put in concerted efforts to reduce morbidity and mortality related to chronic diseases, including asthma. These efforts led to many new initiatives to develop clinical practice guideline, to conduct research to fill the gaps, to develop new interventions and to continuously update the guidelines according to experimental data (Szefler, 2011). Despite all these efforts, substantial proportions of asthmatic patients do not achieve proper asthma control Price et al., 2014; Braido et al., 2016). In Ethiopia, prevalence of uncontrolled asthma is relatively high (Zemedkun et al., 2014; Gebremariam et al., 2017).
Socio-demographic characteristics, psychosocial factors, asthma severity, adherence to monitoring and treatment guideline, drug regimens, inhalational techniques, and exposure to infectious agents and allergens, and co-morbid diseases were found to influence asthma control. A limited number of studies in Ethiopia indicated most asthmatic patients attending hospitals in Ethiopia had uncontrolled or partially controlled asthma due to several risk factors for poor asthma control (Zemedkun et al., 2014; Gebremariam et al., 2017).The aim of this study was to evaluate the level and determinants of asthma disease control among asthmatic patients at the Ambo University Referral Hospital (AURH) through the GINA criteria and to assess the factors that might influence control of the disease.
ETHICAL APPROVAL
Ethical clearance to conduct this study was secured and obtained from the Ethical Review Board of College of Medicine and Health Sciences of Ambo University. Permission to collect data was secured from AURH medical director. Participants were provided an explanation of the study objective and were included in the study after verbal consent was secured. The confidentiality of the study participants was maintained by assigning unique study identifiers during data collection and analysis.
METHODOLOGY
Study area and design
This observational cross-sectional study was conducted in AURH from February to March 2019 on a sample of 82 asthmatic patients. During this period, the investigators filled the questionnaires and validated by experts (physicians in the Medical Ward of the AURH) concerning the asthma control level, socio-demographic, clinical and environmental characteristics and medications use. The feasibility of the study was conducted in the hospital within the research to access the validity and quality of the questionnaires.
Study population
Asthmatic patients were included in the study, if they were diagnosed with asthma for at least three months by physicians, according to Ethiopian General Hospital Standard Treatment guideline and GINA guideline (FMHACA, 2014; Global Initiative for Asthma, 2018). The diagnosis was based on medical history and physical examination. Patients with mental illness, chronic obstructive pulmonary disease (COPD), bronchiectasis, lung cancer, and cardiac illness were excluded from the study. The date of inclusion in the study is the first date of contact with the patient.
Study variables
The dependent variable was asthma disease control, according to GINA criteria (Global Initiative for Asthma, 2018). GINA asthma control criteria (shown in Table 1) were evaluated for each study participant and the level of asthma symptom control questionnaire were administered to the patient on the first day of the visit. These include; frequency of the daytime symptoms, nighttime symptoms, use of rescue medication (selective short-acting bronchodilators like inhalational Salbutamol) in the previous week and any limitations of activity. Accordingly, patients were classified into three classes; controlled, partially controlled and uncontrolled asthma.
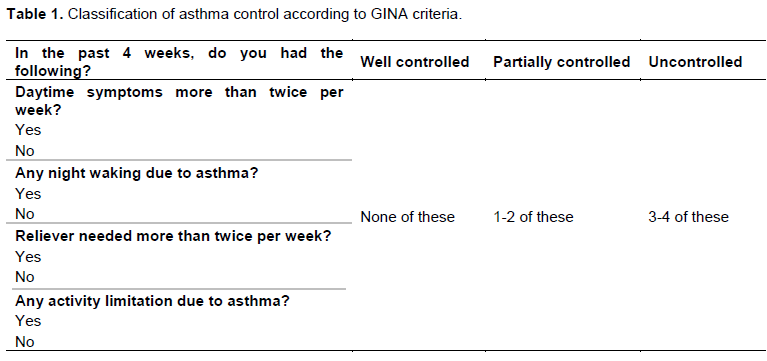
i) Controlled asthma: the absence of daytime symptoms (no more than twice a week), the absence of nighttime symptoms, no limitations in activities, and limited need for rescue medication (not more than twice a week).
ii) Partially controlled: one or two of the four questions according to GINA criteria.
iii) Uncontrolled asthma: the presence of three or more events of daytime symptoms (more than twice a week), the presence of nighttime symptoms, limitations in activities, and need for rescue medication (more than twice a week) for the last four weeks. The independent variables, including Socio-demographic, clinical and environmental characteristics were collected using interview, observational and patient card review. Clinical characteristics of asthmatic patients and the use of ICS medication, including its adherence issues was assessed by checking whether patients faced with the difficulty of inhaling technique by asking them to demonstrate how they are using their metered dose inhaler or nebulizer. Adherence was assessed by asking the patients whether they can access the medication, and remember to use at the right time at prescribed dose and duration. Using more than 200 dose/month of inhaled Salbutamol was considered as a high dose SABA use according to GINA guidelines (Global Initiative for Asthma, 2018).
Socio-demographic variables: Age, sex, marital status, occupational status, place of residence, education status, and economic status.
Clinical and environmental variables: Co-morbidities, exposure to asthma triggering agents, history of asthma exacerbation, emergency visit due to asthma attacks, history of intubation, psychological problem, adherence to treatment, social drug use, types of drug used.
Statistical analysis
The collected data were cleaned, coded, and entered into the SPSS version 20.0 software. Descriptive statistic was used to describe the percentage and the number distributions of variables in the study. The results were represented as percentages in valid results. Continuous variables were represented as a mean and standard deviation (SD). Categorical variables were represented as percentages.
Binary logistic regression analysis was used to determine factors associated with poor asthma control. A univariate logistic regression analysis was performed to separately examine the association of each factor with the asthma disease control. Then, all factors with a statistical significance of p-value < 0.25 in the univariate analysis were included in multivariable logistic regression. The final models were built using a stepwise selection method with a p < 0.05 significance level. The controlled asthma disease was considered as a reference category.
RESULTS
Socio-demographic characteristics of asthmatic patients
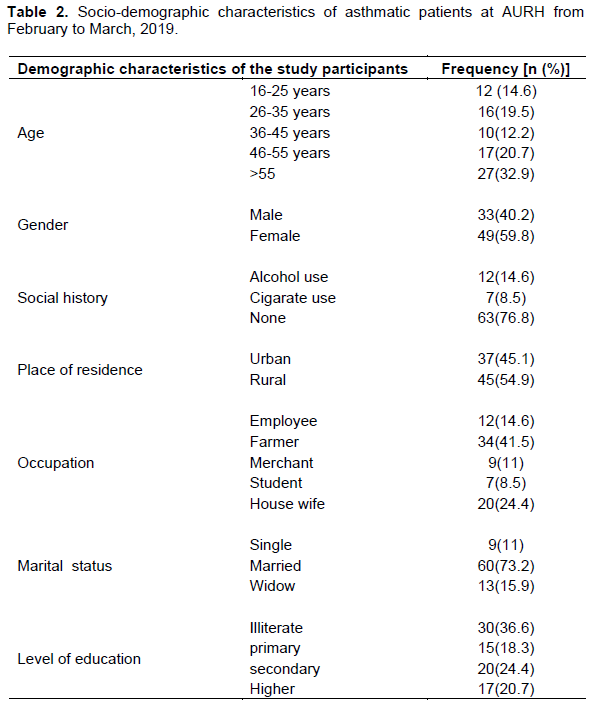
A total of 82 asthmatic patients with a mean age (standard deviation [SD]) of 44.9 ± 8.9 of years were participating in the study, of which 59.8% were females. Significant proportions of the study participants were illiterate (36.6%) and farmers (41.5%). The number of alcohol users and smokers were 12 (14.6%) and 7 (8.5%), respectively as shown in Table 2.
Clinical characteristics of asthmatic patients
According to GINA criteria, 23.2% of patients were controlled, 2.4% had partial control and 74.4% were poorly controlled. For this study, we considered the partially controlled group as uncontrolled asthma (total 76.8%) to determine factors associated with controlled asthma in multivariable logistic regression.
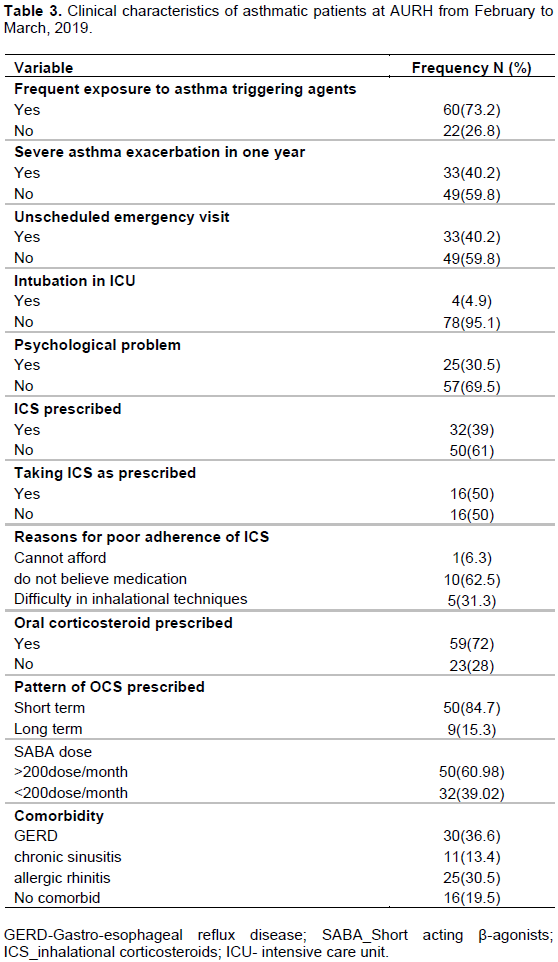
Of all, 33 (40.2%) of the patients had an emergency visit due to asthma exacerbations in the past 12 months and 4 patients were intubated in the intensive care unit (ICU). Large proportions of patients (80.5%) had concomitant disease and its proportion differed significantly across the groups of patients with the highest value in uncontrolled asthma groups (65.9%). Heartburn (GERD), 30 (36.6%) and allergic rhinitis, 25 (30.5%) were the most prevalent co-morbidities. The proportion of each concomitant disease was statistically significant for the group of patients with the highest value in uncontrolled asthma groups for GERD (93.3%) and allergic rhinitis (64%) with p-value of <0.05. Table 3 presented the clinical characteristics of asthmatic patients.
Pharmacological treatment
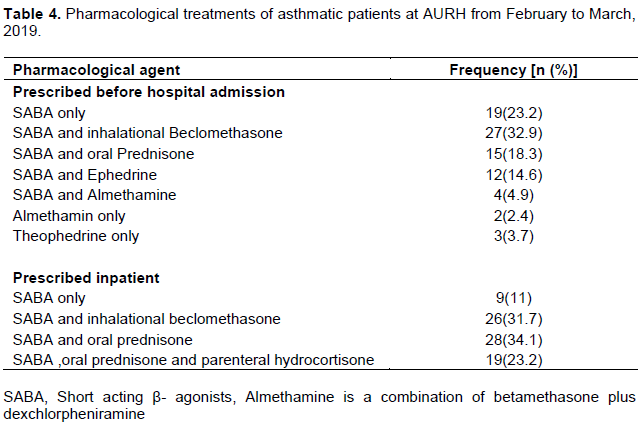
Large proportions of patients (89.02%) recruited were treated with SABA plus medium/high daily doses of corticosteroids. Table 4 illustrates the types of drugs used by the 82 patients. Oral corticosteroids were ever prescribed in 59 (72%) patients, of which 50 patients were short term indication. ICS was indicated for 32 (39%) of the patients. SABA plus inhalational beclomethasone were the most common drug therapy prescribed both in the outpatient and inpatient, 27 (32.9%) and 26 (31.7%) respectively. SABAs only were used in 9 patients. Poor adherence to ICS was reported in half of the patients. Lack of trust to the effectiveness of the medication (62.5%), difficult with inhalational techniques (31.3%), and unable to afford the medications were the leading causes.
Determinants of asthma disease control
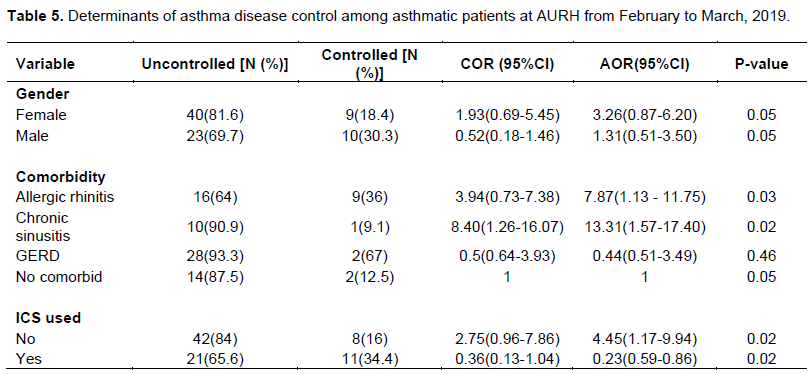
A stepwise binary logistic regression was used to determine association between dependent variable (GINA asthma control) and independent variables (age, sex, marital status, occupational status, place of residence, education status, economical status, co-morbidities, exposure to asthma triggering agents, history of asthma exacerbation, emergency visit due to asthma attack, history of intubation, psychological problem, adherence to treatment, social drug use, and types of drug used). In univariateanalysis, asthmatic patients with concomitant disease like allergic rhinitis (Crude odd ratio, COR: 3.94; 95% CI [0.73-7.38]), and chronic sinus (COR: 8.40; 95% CI [1.26-16.07]) were the most predictive of poor asthma control with a significance level for removal from model of 0.25. Similarly, female patients (COR: 1.93; 95% CI [0.69 - 5.45]) and those that had no prescribed ICS (COR: 2.75; 95% CI [0.96-7.86]) had a greater risk of uncontrolled asthma than their comparator.
In multivariate analysis, patients having concomitant allergic rhinitis (Adjusted odds ratio= AOR: 7.87;95% CI [1.13 - 11.75]) and chronic sinus (AOR: 13.31; 95% CI [1.57-17.40]), not used ICS (AOR: 4.45; 95% CI [1.17-9.94]) and female sex (AOR: 3.26; 95% CI [0.87-6.20]) had increased odds of uncontrolled asthma with p-value of <0.05 as shown in Table 5.
DISCUSSION
In this study, a total of 82 asthmatic patients from AURH uncontrolled asthma, according to GINA criteria. The proportion of this finding is relatively higher than the reports from other parts of the African countries, 63.3% in Nigeria (Desalu et al., 2012)and 56% in Congo (Kabengele et al., 2019). In Ethiopia, similar studies conducted in Addis Ababa and Jimma indicated lower proportion of patients had uncontrolled asthma, 71.4 and 65% respectively (Zemedkun et al., 2014; Gebremariam et al., 2017). Poor control of asthma was reported from Italian observational cross sectional study (Corrado et al., 2013)in which only 9.1% had controlled asthma according to asthma control test (ACT). In contrast to these studies and despite asthma control is suboptimal worldwide, relatively well-controlled asthma was reported from Iran 54.7% (Asthma, 2017), Bangkok (46.7%) (Wanlapakorn et al., 2014)and Saudi Arabia (60.2%) (Al-Zahrani et al., 2015). A study conducted in Pneumology and Allergy Hospital units in Spain indicated, only 3.9% had uncontrolled severe persistent asthma (Kabengele et al., 2019). This might indicate there is a significant difference in asthma control among developed countries and developing countries. Studies suggested that African countries have significant poverty and a higher level of air pollution in comparison to European and other developed countries (Sinharoy et al., 2018).
The multivariate analysis showed that co-morbidities like allergic rhinitis and chronic sinus, being a female, and patients never prescribed ICS were predictive of poor asthma control. Females had 3.3 times more odds of uncontrolled asthma than males. The finding was comparative with other studies. A study from Saudi Arabia reported that females had approximately 2 times greater odds of having uncontrolled asthma than males (Bin Saeed, 2015). Similarly, a study from Cameroon reported that major risk factor associated with poor asthma control was being a female (Hugo et al., 2016). Other studies from Turkey, Italy, and the USA showed that females have poorer asthma control than males (Turktas et al., 2010; Corrado et al., 2013; McCormick et al., 2014). This might be due to frequent exposure of the majority of females to different asthma triggering agents. In this study, the majority of female asthmatic patients (73.5%) were frequently exposed to asthma triggering agents where more than half of those populations live in rural area.
The current study showed that asthmatic patients having chronic sinusitis and rhinitis were more likely to encounter uncontrolled asthma than their comparator. Inconsistent with this finding, a study from Saudi Arabia found that asthmatic patients with chronic sinusitis had 2.0 times more odds of uncontrolled asthma (Bin Saeed, 2015).UK study reported that rhinitis patients were 4-5 times more likely to have poorly controlled asthma than their comparator (Hoskins et al., 2011). Other studies also confirmed that allergic rhinitis and sinusitis are associated with more exacerbations in patients with poorly controlled asthma and severe asthmatic symptoms (Guerra et al., 2002; Dixon et al., 2006; Hojo et al., 2015).
The other predictive factor associated with poor asthma control was lack of inhaled corticosteroids, which is the preferred first line controller therapy for persistent asthma. The result of this study showed that only 39% of asthmatic patients had ever prescribed ICS and asthmatic patients who never prescribed ICS had 4.5 times increased odds of uncontrolled asthma. Several studies indicated that use of corticosteroids improved asthma control, survival and quality of life (Suissa et al., 2000; Boulet et al., 2012; Louis et al., 2012). A similar study from Turkey found that the percentage of patients using inhaled corticosteroid (ICS) were significantly lower in patients with uncontrolled disease compared to controlled asthma patients (Turktas et al., 2010).
CONCLUSION
In this study, only 23.2% of patients were well controlled asthma according to GINA criteria. Less modifiable demographic factors like being a female sex significantly increased the odds of having uncontrolled asthma. Clinical factors such as lack of prescribed ICS and co- morbidities like allergic rhinitis and chronic sinusitis increased the risk of uncontrolled asthma.
LIMITATION OF THE STUDY
The major limitation of this study was a small sample size and lack of adequate asthma diagnostic and monitoring parameters in the hospital like a lung function test (Spirometers) to effectively measure the level of asthma control. The current asthma symptoms alone might not accurately reflect the level of asthma severity and control. The other limitation of this study was, the fact that we did not ascertain whether the patients were actually taking the prescribed medications, and there is no effective and accurate manner in which to measure true asthma medication adherence. Moreover, our sample size was not uniform in various criteria like males, females, and children as it may affect our statistical data predictions and conclusions.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
FUNDING
Funding was obtained from Ambo University.
REFERENCES
|
Akinbami LJ, Sullivan SD, Campbell JD, Grundmeier RW, Hartert TV, Lee TA, Smith RA(2012).Asthma outcomes: healthcare utilization and costs. Journal of Allergy and Clinical Immunology 129(3):S49-S64. |
|
|
Al-Zahrani JM, Ahmad A, Abdullah AH, Khan AM, Al-Bader B, Baharoon S, Hamdan AJ (2015). Factors associated with poor asthma control in the outpatient clinic setting. Annals of thoracic medicine 10(2):100. |
|
|
BinSaeed AA (2015).Asthma control among adults in Saudi Arabia: Study of determinants.Saudi Medical Journal 36(5):599. |
|
|
Boulet LP, Vervloet D, Magar Y, Foster JM (2012). Adherence: the goal to control asthma. Clinics in chest medicine 33(3):405-417. |
|
|
Braido F, Brusselle G, Guastalla D, Ingrassia E, Nicolini G, Price D, LIAISON Study Group. (2016). Determinants and impact of suboptimal asthma control in Europe: The international cross-sectional and longitudinal assessment on asthma control (LIAISON) study. Respiratory research 17(1):51. |
|
|
Centers For Disease Control and Prevention (2010) 'Asthma's Impact on the Nation Data from the CDC National Asthma Control Program',CDC: Asthma's Impact on the Nation (2012). |
|
|
Corrado A, Renda T, Polese G, Rossi A (2013). Assessment of asthma control: the SERENA study. Respiratory Medicine 107(11):1659-1666. |
|
|
Desalu OO, Fawibe AE, Salami AK (2012).Assessment of the level of asthma control among adult patients in two tertiary care centers in Nigeria. Journal of Asthma 49(7):765-772. |
|
|
Dixon AE, Kaminsky DA, Holbrook JT, Wise RA, Shade DM, Irvin CG (2006).Allergic rhinitis and sinusitis in asthma: differential effects on symptoms and pulmonary function. Chest 130(2):429-435. |
|
|
FMHACA (2014). Food, Medicine and Healthcare Administration and Control Authority of Ethiopia Standard Treatment Guidelines For General Hospital Diseases Investigations Good Prescribing & Dispensing Practices for Better Health Outcomes' Stg. |
|
|
Gebremariam TH, Binegdie AB, Mitiku AS, Ashagrie AW, Gebrehiwot KG, Huluka DK, Schluger NW (2017). Level of asthma control and risk factors for poor asthma control among clinic patients seen at a Referral Hospital in Addis Ababa, Ethiopia. BMC research notes 10(1):558. |
|
|
Global Initiative for Asthma (GINA) (2018). Global Strategy for Asthma Management and Prevention, 2018. |
|
|
Global Asthma Network (2018). The Global Asthma Report 2018, Auckland, New Zealand. doi: ISBN: 978-0-473-29125-9\r978-0-473-29126-6 (ELECTRONIC). |
|
|
Godard P, Chanez P, Siraudin L, Nicoloyannis N, Duru G (2002). Costs of asthma are correlated with severity: a 1-yr prospective study. European Respiratory Journal 19(1):61-67. |
|
|
Guerra S, Sherrill DL, Martinez FD,Barbee RA (2002). Rhinitis as an independent risk factor for adult-onset asthma. Journal of Allergy and Clinical Immunology 109(3):419-425. |
|
|
Hojo M, Ohta K, Iikura M, Hirashima J, Sugiyama H, Takahashi K (2015).The impact of co-existing seasonal allergic rhinitis caused by Japanese Cedar Pollinosis (SAR-JCP) upon asthma control status. Allergology International 64(2):150-155. |
|
|
Hoskins G, Williams B, Jackson C, Norman PD, Donnan PT (2011). Assessing asthma control in UK primary care: use of routinely collected prospective observational consultation data to determine appropriateness of a variety of control assessment models. BMC family practice 12(1):105. |
|
|
Hugo MNB, Walter PYE, Maïmouna M, Malea NM, Ubald O, Adeline W,Christopher K(2016).Assessment of asthma control using asthma control test in chest clinics in Cameroon: a cross-sectional study. Pan African Medical Journal 23(1). |
|
|
Kabengele BO, Kayembe JMN, Kayembe PK, Kashongue ZM, Kaba DK, Akilimali PZ (2019). Factors associated with uncontrolled asthma in adult asthmatics in Kinshasa, Democratic Republic of Congo. PloS one 14(4). |
|
|
Louis R, Schleich F, Barnes PJ (2012). Corticosteroids: still at the frontline in asthma treatment?. Clinics in Chest Medicine 33(3):531-541. |
|
|
McCormick SP, Nezu CM, Nezu AM, Sherman M, Davey A, Collins BN (2014).Coping and social problem solving correlates of asthma control and quality of life. Chronic Respiratory Disease 11(1):15-21. |
|
|
Nocon A, Booth T (1991).The social impact of asthma. Family Practice 8(1):37-41. |
|
|
Nunes C, Pereira AM, Morais-Almeida M (2017). Asthma costs and social impact. Asthma research and practice 3(1):1. |
|
|
Price D, Fletcher M, Van Der Molen T (2014). Asthma control and management in 8,000 European patients: the REcognise Asthma and LInk to Symptoms and Experience (REALISE) survey. NPJ primary care respiratory medicine 24:14009. |
|
|
Sinharoy A, Mitra S, Mondal P (2018). Socioeconomic and environmental predictors of asthma-related mortality. Journal of environmental and public health 2018. |
|
|
Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, Harvey I (2005). A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma. In NIHR Health Technology Assessment programme: Executive Summaries. NIHR Journals Library. |
|
|
Suissa S, Ernst P, Benayoun S, Baltzan M,Cai B (2000). Low-dose inhaled corticosteroids and the prevention of death from asthma. New England Journal of Medicine 343(5):332-336. |
|
|
Szefler SJ (2011).Advancing asthma care: the glass is only half full!. Journal of allergy and clinical immunology 128(3):485-494. |
|
|
Turktas H, Mungan D, Uysal MA, Oguzulgen K (2010). Determinants of asthma control in tertiary level in Turkey: a cross-sectional multicenter survey. Journal of Asthma 47(5):557-562. |
|
|
Wanlapakorn N, Sritippayawan S, Deerojanawong J (2014). Prevalence of asthma, level of control and factors associated with asthma control in Thai elementary school students in Bangkok. Asian Pacific journal of allergy and immunology 32(4):287. |
|
|
Zemedkun K, Woldemichael K, Tefera G (2014). Assessing control of asthma in Jush, Jimma, south west Ethiopia. Ethiopian journal of health sciences 24(1):49-58. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


