Review

ABSTRACT
Helicobacter pylori is a microorganism which has been the reason of various diseases, including gastritis, peptic, duodenal ulcer and cancer of the stomach. Urea breathe test (till 6 years), stool antigen test and serology testing are used for diagnosis. Triple, quadruple, sequential, salvage and levofloxacin, omeprazole, nitazoxanide, and doxycycline (LOAD) therapies are used for treatment of all H. pylori infections. Providing patient education regarding adherence, proper administration of drug and their adverse effects is one of the most important roles of pharmacists.
Key words: Helicobacter pylori, infection, levofloxacin, omeprazole, nitazoxanide, and doxycycline (LOAD) therapy, salvage therapy.
INTRODUCTION
Helicobacter pylori, negative spiral or curved microorganism has been widely studied after his discovery, by human gastric biopsy, in 1983. H. pylori is commonly associated with the gastritis, peptic and duodenal ulcer as well as cancer of the stomach. The most common disease caused by H.pylori is peptic ulcer (Magdalena et al., 1991).
Epidemiology
H. pylorus is the most common pathogenic organism worldwide. Overall, almost 50% population of the world is infected by this organism, while the occurrence in some developing countries is as high as 80 to 90%, whereas in the U.S., 35 to 40% of the population are infected (Brian et al., 2001).
Transmission of H. pylori
The exact route of transmission of H. pylori is not fully known. H. pylorus is mainly transmitted by oral ingestion and it is mostly transmitted within families in developed countries. In underdeveloped countries, the prominent routes are saliva, feces and gastro-oral route (Robert et al., 2001).
Pathogenesis
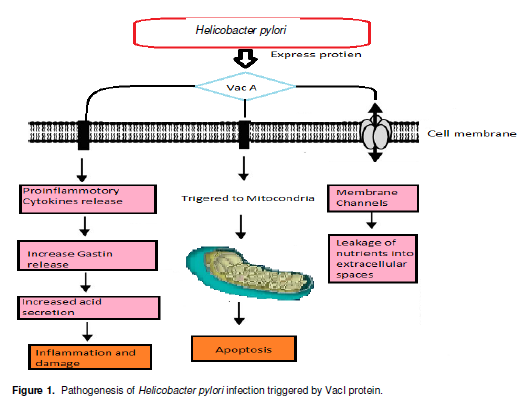
The gastric mucosa shows well protection against bacteriological infection. H. pylorus with distinctive properties enters into the mucus and get attached to the epithelial cells. H. pylori have potential to escape from the defense mechanism of the body due to which it shows persistent colonization (Sebastian and Pierre, 2002). After being entered to mucus layer, bacteria survive into the acidic pH which is due to hydrolysis of the urea by enzyme urease into ammonia and carbon dioxide. Urease activity is further regulated by urei, pH-gated urea channel (Sebastian and Pierre, 2002). Most of H. pylori strains discharge a 95-kDa protein named as VacA. The VacA protein plays an important role in the pathogenesis of both peptic ulceration and gastric cancer. VacA gets attach to the epithelial cell membranes and forms a voltage gated channels in the membrane, thus prompting the release of urea, bicarbonates and nutrients from the host cells (Johannes et al., 2006). Vac within the epithelial cell membrane release proinflammatory cytokines due to which there is an increase in the gastrin release and reduction in antagonist and inhibitor somatostatin. This in turns increases the acid secretion from the parietal cells and bicarbonates release is reduced which causes inflammation and damage that leads to ulcer and if untreated gastric carcinoma (Anahita and Emad, 2012). Vac also directly entered to the mitochondria where it releases cytochrome c which causes apoptosis and leads to carcinoma (Sebastian and Pierre, 2002) (Figure 1).
DIAGNOSIS
Different invasive and non-invasive diagnostic tests were performed for the detection of H. pylori infection. In non-invasive test for the initial diagnosis of the infection of H. pylori, urea breath test is performed. The specificity and sensitivity of the test is 90%. The test should be performed after 4 weeks otherwise it will give false results. Urea test can be done for children above 6 years. Another cheap and mostly used non-invasive test is serology testing. Its shows same specificity and sensitivity as urea breath test, but this test is not reliable in young children. Stool antigen test is also an alternative to urea breath test with 90% specificity and 89 to 98% sensitivity. Mostly, stool test is performed for the follow up of infection. It is the test of choice in almost all ages of children. An invasive test like endoscopy is preferred in patient with severe symptoms like gastrointestinal (GIT) bleeding as well as with age more than 50 years. An antibiotic sensitivity culture test is not routinely performed for the initial diagnosis of the infection (Sebastian and Pierre, 2002).
TREATMENT FOR H. PYLORI INFECTION
Triple therapy
For the treatment of H. pylori infection, first line recommended therapy is a proton pump inhibitor (PPI)-based triple therapy, that is, standard PPI dose twice daily + clarithromycin 500 mg twice daily + amoxicillin 1000 mg twice daily for 10 days (Calvet, 2006). From different studies and analysis, it is proven that triple therapy shows better results with twice daily dosing of proton pump inhibitor and clarithromycin is used twice in a dose of 500 mg, rather than 250 mg. Although recommended as an alternative to patients who are penicillin allergic; the combination of clarithromycin and metronidazole should be discouraged as there is currently no effective salvage therapy if such a combination fails (Silva et al., 2008). In triple therapy regimens, clarithromycin substitution with other macrolides (e.g., erythromycin or azithromycin) is not recommended due to low efficacy (Graham and Fischbach, 2010). From recent studies, increased resistance to metronidazole and clarithromycin up to 42 and 20%, respectively is shown and the cure rate of the standard triple therapy has fallen below the acceptable rate of >80% in many regions (Vaira et al., 2009). So this therapy is not recommended as first line nowadays except local susceptibility patterns show such a treatment regimen to be highly effective (Calvet, 2006).
Quadruple therapy
Quadruple therapy is used as an alternative to the triple therapy. It includes PPI or H2-blocker (U.S. Guidelines only) + bismuth+ tetracycline + metronidazole, that is, used for 10 to 14 days. Quadruple therapy is used as first-line therapy for eradication of H. pylori. Formerly, it was thought that the dosing of quadruple therapy is complex and less tolerated, so triple PPI therapy was considered the first line therapy for H. pylori infection treatment. Now quadruple therapy becomes first line treatment due to increased clarithromycin resistance. In standard quadruple therapy, the substitution of doxycycline for tetracycline is not recommended due to the lack of data (Calvet, 2006).
Sequential therapy
Sequential therapy is a 10 day course which starts with PPI twice daily and amoxicillin 1000 mg twice daily after which immediate 5-day course of tinidazole 500 mg twice daily, and a PPI twice daily or clarithromycin 500 mg twice daily, and metronidazole 500 mg (Calvet, 2006). European studies show a very high cure rate of this therapy, that is, 92% (Malfertheiner et al., 2012; Ruggiero, 2012). From two different analyses it is proved that this therapy is effective in macrolide resistant H. pylori (Calvet, 2006).
Salvage therapy
An eradication rate for H. pylori is ranging from 63 to 94% in Asian and European populations are shown with salvage therapy. Salvage therapy is a regimen of levofloxacin-based triple therapy. A meta-analysis including four randomized controlled trials showing that a 10-day levofloxacin-based triple therapy regimen had a superior eradication rate and was associated with fewer side effects as compared to a 7-day course of bismuth-based quadruple therapy. However, these results require validation in the North American population. Furthermore, the optimal levofloxacin dose 250 mg twice daily vs. 500 mg daily vs. 500 mg twice daily and duration of therapy either 7 or 10 days has yet to be determined. However, another meta-analysis did find a higher eradication rate with the 10-day over 7-day regimen. Unfortunately, resistance to fluoroquinolones is rapidly increasing. Experts now recommend using fluoroquinolone therapy only when susceptibility data are available (Calvet, 2006; Lacy et al., 2012)
Levofloxacin, omeprazole, nitazoxanide, and doxycycline (LOAD) therapy
A new four-drug regimen shows greater effectiveness with cure rate 88.9% with 10 days treatment and 89.4% with 7-day treatment in an open label study. LOAD therapy is levofloxacin 250 mg daily with breakfast + omeprazole 40 mg daily before breakfast + nitazoxanide 500 mg twice daily + doxycycline 100 mg daily for dinner. A larger randomized controlled trial is warranted to further evaluate the efficacy of this treatment regimen (Calvet, 2006; Malfertheiner et al., 2012).
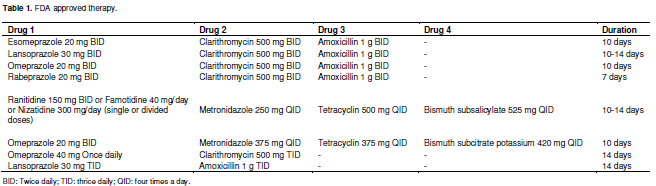
Food and drug administration (FDA) approved therapy
PPIs are taken before meal. Metronidazole recommended dose is 1500 mg/day to overcome metronidazole resistance and getting better efficacy. Avoid cimetidine to reduce drug interaction. Lansoprazole + Amoxicillin combination is used only in clarithromycin allergic or resistant patients. Calvet 2006 (Table 1).
PATIENT COUNSELLING (ROLE OF PHARMACIST)
Patient adherence is essential for successful eradication of H. pylori. Given the high pill burden, the increased frequency of administration and the prolonged duration of treatment, thorough understanding of the importance of completing the treatment regimen as prescribed is paramount. No adherence may be associated with awful outcomes, including treatment failure and antibiotic resistance. While adherence and proper administration of the regimen are crucial points of emphasis, patients should also be informed about potential treatment related adverse effects. Advanced notification about common adverse effects as well, providing suggestions for management may help to prevent premature discontinuation of the regimen.
(1) PPIs are well tolerated, but headache, dizziness, nausea, diarrhea, constipation and abdominal pain may occur. Patients should be instructed to take PPIs 30 to 60 min prior to a meal.
(2) Hypersensitivity to any component of the regimen may occur; however, this type of reaction is most likely with amoxicillin. Amoxicillin and clarithromycin are commonly associated with GI upset (nausea, vomiting, diarrhea and abdominal pain). Amoxicillin may also be associated with headache and clarithromycin may also be associated with taste disturbances, such as a bitter or metallic taste in the mouth.
(3) Metronidazole elicits adverse effects similar to clarithromycin (that is, GI upset and metallic taste in the mouth) but also may be associated with a disulfiram-like reaction with alcohol consumption.
(4) In patients on warfarin initiating metronidazole, international internalized ratio (INR) elevations are common and require close monitoring.
(5) Tetracycline is associated with GI upset, photosensitivity and tooth discoloration. Patients should be advised to wear sunscreen and avoid prolonged exposure to sunlight.
(6) Pregnant patients and children under the age of eight should not receive tetracycline. Certain medications and foods such as calcium, antacids, iron and milk, may reduce the absorption and, thus, the effectiveness of tetracycline. .
(7) Bismuth may cause GI upset and darkening of the tongue and stool. Bismuth containing regimens should be used with caution in patients with renal impairment as accumulation may occur. Patients with aspirin (salicylate) sensitivity should avoid the subsalicylate form of bismuth (Malfertheiner et al., 2012; Ruggiero, 2012; Lacy et al., 2012).
DISCUSSION
Patient adherence is essential for successful eradication of H. pylori. Providing patient education regarding adherence, proper administration of drug therapy and adverse effects is one of the most important roles that pharmacists provide in caring for patients with H. pylori (Anahita and Emad, 2012). Additionally, pharmacists with access to prescription and/or medical records can review those records for prior clarithromycin and/or metronidazole use, which may increase the likelihood of antibiotic resistance and treatment failure. Patient allergies identified during record review should be considered in choosing a regimen. For patients with allergies, regimens containing those antibiotics should be avoided. Other factors, such as drug interactions and contraindications to drug therapy, may influence treatment. Adverse effects, ease of administration and cost may also influence the choice of an initial eradication regimen. Finally, following completion of the eradication regimen, pharmacists may assist with monitoring of persistent or recurrent symptoms. Patients should be advised to contact a health care professional if symptoms persist or recur or if they experience alarm symptoms during treatment, such as blood in the stool. Pharmacists have the opportunity to fulfill many roles and have a valuable impact on patient care for H. pylori (Calvet, 2006; Silva et al., 2008; Graham and Fischbach, 2010; Vaira et al., 2009).
CONFLICT OF INTEREST
Authors declare that there are no conflicts of interest.
REFERENCES
| Magdalena K, Janice D, John W, Trevor J (1991). Identification, characterization and localization of two flagellin species in Helicobacter pylori flagella. J. Bact. 173(3):937-946. | ||||
| Brian E, Lacy R, Justin R, Brian E (2001). Helicobacter pylori: Ulcers and More: The Beginning of an Era. JJ Nutr. Sci. 131(10):1289-1292. | ||||
| Robert P, Logan H, Marjorie M (2001). Epidemiology and diagnosis of Helicobacter pylori infection. Brit. Med. J. 323(2):920-927. | ||||
| Sebastian S, Pierre M (2002). Helicobacter pylori infection. Nat. Eng. J. Med. 347(15):234-239. | ||||
|
Johannes G, Arnoud H, Vliet V, Ernst J (2006). Pathogenesis of Helicobacter pylori Infection. Clin. Microbiol. Rev. 19(3):449-452. crossref |
||||
| Anahita Dua, Emad M (2012). Helicobacter Pylori, peptic ulcers and gastric cancer. Understaning Med. Res. 11(2):191-198. | ||||
|
Calvet X (2006). Helicobacter pylori infection: treatment options. Digestion. 73(1):119-128. crossref |
||||
|
Silva FM, Eisig JN, Teixeira AC (2008). Short-term triple therapy with azithromycin for Helicobacter pylori eradication: low cost, high compliance, but low efficacy. BMC Gastroenterol. 8(2):20-24. crossref |
||||
|
Graham DY, Fischbach L (2010). Helicobacter pylori treatment in the era of increasing antibioticresistance. Gut. 59(3):1143-1153. crossref |
||||
|
Vaira D, Zullo A, Hassan C (2009). Sequential therapy for Helicobacter pylori eradication; the time is now! Therap Adv. Gastroenterol. 2(1):317-322. crossref |
||||
|
Malfertheiner P, Selgrad M, Bornschein J (2012). Helicobacter pylori: clinical management. Curr. Opin. Gastroenterol. 28(6):608-614. crossref |
||||
|
Ruggiero P (2012). Helicobacter pylori infection: what's new. Curr. Opin. Infect. Dis. 25(3):337-344. Pubmed |
||||
| Lacy BE, Talley NJ, Locke GR, Bouras EP, DiBaise JK, El-Serag HB, Abraham BP, Howden CW, Moayyedi P, Prather C (2012). Review article: current treatment options and management of functional dyspepsia. Aliment. Pharmacol. Ther. 36(1):03-15. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


