ABSTRACT
The teaching model based on objective, measurable, and linear knowledge no longer seems to be the most appropriate, given the new responsibilities of pharmacists, who should focus their practices on patient care. The objective of the present study was to analyze students' perception about preparedness to pharmacy practice and to patient-centered care, and identify experiential training barriers Two discussion groups were formed with 12 and 13 individuals to present their perceptions about teaching and learning for pharmaceutical care. The analysis followed the methodology of Bardin. The analysis of the answers indicates that there is a significant gap in the training of pharmacists, with a strong emphasis on theoretical issues and less focus on knowledge acquisition and interpersonal communication, generating poor professional training and relationship barriers. In general, students do not feel prepared to deal with patients. These students identify the lack of infrastructure, such as the lack of a pharmacy and underutilization of the hospital, deficiencies in the curriculum such as the lack of key subjects, lack of clinical practice, and lack of preparation of some teachers, with an excess of classes following the lecture format. These factors influence the teaching and learning of clinical and communication skills, which undermine the pharmacists' ability to carry out clinical interventions, as well as affect the pharmaceutical-patient and pharmaceutical-physician relationship. These results suggest that for the pharmacists' clinical training it is necessary to rethink whether the infrastructure, the curriculum, and the teaching method are adequate for the development of skills and competences.
Key words: Pharmaceutical care, pharmacy education, skills, competences.
Over the last two decades, pharmacy practice, which once focused primarily on medicines and their supply has been re-professionalized with patient-centered care as its focus (Bond, 2006; Hassali et al., 2011; Koster et al., 2014). As a result of the paradigm shift within the profession, pharmacists are now more involved in direct patient care (Academic Medical Centers, 2010). According to the literature, this shift to the social context requires rethinking the process of professional training (De Oliveira, 2011; Koster et al., 2014). Ivama (1999) and Nicoleti (2010) observed that pharmaceutical education must follow social and political trends. In this new scenario, the training of these professionals is a challenge that demands the competences required to enable the provision of patient-centered care (Fuhrman et al., 2001; Troncon, 2007). The WHO recommends that pharmacists should have specific knowledge, skills, and attitudes in this new role (Sarrif et al., 2012). In agreement with Hassali et al. (2011), to be effective in their actions, pharmacists need to be well prepared to deal with patients. Various studies have reported the positive role of clinically trained pharmacists as mentioned by other healthcare professionals (Hanlon et al., 1996; Papadopoulos et al., 2002; Krupicka et al., 2002; McKee et al., 2011).
For De Oliveira (2011), the teaching model based on objective, measurable, and linear knowledge no longer seems to be the most appropriate, given the new responsibilities of pharmacists, demanding changes in the educational model and curriculum of universities (Hassali et al., 2011). Undergraduate curricula have shifted towards the integration of science and practice, focused on clinical pharmacy as an instrument to attain higher quality in patient-centered care services (Earl and Reinhold, 2014), emphasizing pharmacists' skill development and assessment, including clinical decision making (Richir et al., 2008), which are essential for successful patient care. Previously, Wertheimer (1991) and Harding and Taylor (1997) had already discussed the importance and the need to include social pharmacy disciplines in the standard undergraduate curricula. In fact, the professional standard of pharmacy still varies significantly across the world (Azhar et al., 2009). Several countries have made changes to teaching for the acquisition of new competences by students of pharmacy (Hassali et al., 2011; Koster et al., 2014; Blom et al., 2011). In order to prepare professionals to deliver hospital pharmacy services with clinical pharmacy and pharmaceutical care, universities from many countries have included clinical pharmacy in their curricula (Hasan et al., 2013).
In the Netherlands, the changes made in the curriculum of Pharmacy have focused on improving the skills of the licensed to practice in community pharmacies andhospitals (Blom et al., 2011). In Brazil, changes were initiated by the establishment of the Curricular Guidelines (Resolution CNE/CES 02/2002) (Brasil, 2002) future pharmacist through the extensive training of the student. At the end of the course, the students are Replacing the Minimum Curricula. They replaced the list of skills and competences to be developed during the course, substantially altering the way of contextualizing higher education. The courses gradually lost their predominantly informative character and begin to be characterized as formative processes that aim at the development of skills necessary for mastery of knowledge and professional performance. Since then, there was flexibility for the institutions to elaborate their pedagogical projects considering their specificities, characteristics, and regions in which they are inserted, the profile of the faculty and students, social needs, among others (Brasil, 2002). Despite this, most schools and diploma in pharmacy courses do not include essentials for clinical practice (Brasil, 1996; Oliveira et al., 2005; Silva, 2009). Although a degree in pharmacy is completed in between 4 and 5 years, most supervised curricular stages occur in the last year of the course, delaying contact with their future work environment and the recognition of these professionals (Brasil, 2013).
The training profile of the future pharmacist should be consistent with the pharmacotherapy management practices, requiring the school to adjust its programs and stages, aiming at the general education of students and allowing them to perform competently and responsibly in the relationship with patients (Hassali et al., 2011; Blom et al., 2011; Fernandes, 2014). In this context, it is essential to understand the views of students on the preparation for the practice of clinical services as an extension of the functions of pharmacists. Therefore, the objective of this study is to evaluate the perception of pharmacy students about their training, focusing on the adequacy to professional practice focused on patient care.
To achieve the objective of the study, students of the pharmaceutical care course were assigned to focal groups (Krueger and Casey, 2000). Pharmaceutical care is a required 4-credit course (60 h) in the five-year Undergraduate Pharmacy Program of the Federal University of Sergipe, Brazil. The general objectives of the course include obtaining an understanding of the pharmaceutical care philosophy and developing the competencies necessary for practicing pharmaceutical care. All the students of the Pharmaceutical Care course were invited to participate in the focus group. Each participant signed a form of consent that described the project goals and notified them that the discussions would be recorded. The students were free to withdraw from the focus group at any time, and they were assured that their identity would remain confidential. Thus, of the 34 students enrolled in the course, 25 (73.53%) participated in the focus group. The sample was randomly subdivided into two focus groups containing 12 and 13 individuals, respectively.
The focus groups were conducted in a meeting room in the School of Pharmacy in São Cristovão, Sergipe, Brazil. During 120-min session, participants of each group were asked to provide their perceptions about their training for patient-centered practice. An interview guide for the focus group interviews was created and tested among a group of students (n = 7). The guide focuses on two key questions to motivate forward discussion by participants as follows: (1) In your opinion, does the course give you the right preparedness for pharmaceutical practice? (2) Does the course prepare you for patient-centered care? The focus groups were conducted by a PhD student acting as the moderator and another MSc student acted as the assistant moderator. The moderator initiated and maintained the discussion, added questions that followed the direction of the dialogue, and sought clarification as time permitted. The moderator was given the flexibility to redirect questions to allow individual participants to make comments and suggestions that were not directly related to the questions posed. It was also the role of the moderator to ensure that no person was able to dominate the conversation, as well as to ensure that all students were given the opportunity to state their opinions.
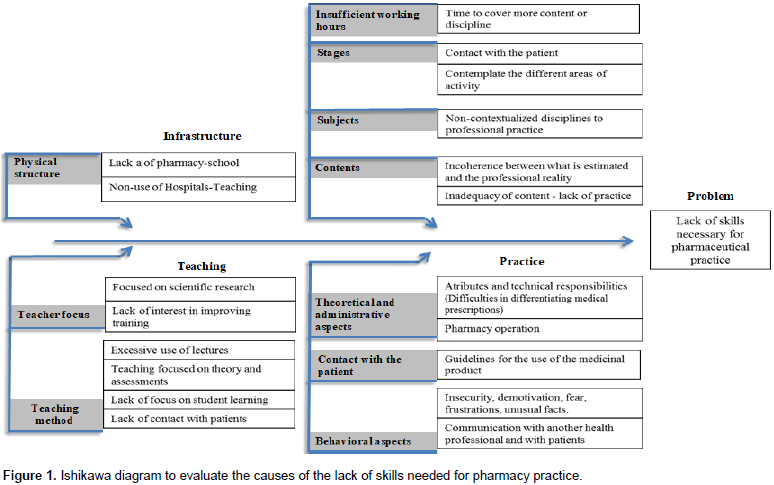
The assistant moderator observed the session, took notes, and monitored the recording device throughout the session. An audio-visual recording of the focus group session was taken and later transcribed, but the names of the students were not recorded with any of the responses. The responses of the students were transcribed, and the data were subjected to a content analysis based on the method of Bardin (Bardin, 1977). To ensure the quality of the data analysis, team members independently read a sub-sample of the transcripts and met regularly to discuss the data and emerging codes, ultimately identifying and agreeing on the main themes. Coding discrepancies were limited and those that occurred were resolved through discussion. For qualitative evaluation, responses to the questions were subjected to a content analysis based on Bardin’s methodology, according to the following steps: (1) pre-analysis consisting of an overview reading; (2) exploration of materials encompassing the identification of sense nuclei attached to the categories related to the central theme ("lack of preparedness for professional practice"), by stratifying data collected from the main pieces of speech and selecting those that better report the view point of respondents; and (3) processing and interpretation of results consisting of a comparison between the results and related works from the literature (Bardin, 2011). The main causes identified by the students as limiting pharmaceutical training for the practice of patient-centered care were obtained through a detailed analysis of participants' verbal comments and organized into the categories (Infrastructure, Curriculum, and Teaching) using the cause and effect diagram (Diagram of Ishikawa), as a way of organizing the reasoning for discussion of the main problems. This study was approved by the ethics and research committee of the Federal University of Sergipe.
The 25 participants actively participated in the discussions and contributed to the results of this study. Most of the individuals surveyed were female (73.33%), aged between 21 and 25 years (86.67%), attending the fourth year (96.67%). One of the students attended the third year of the course. The members of both focus groups identified various causes for the lack of skills needed for professional practice, which are as shown in Figure 1. Some of the perceptions of the students reinforce root causes and are evidenced as described in Table 1.
The trend towards a more humanistic training of the pharmacist should relate the development of competencies and skills applied to the study of the drug with concern for the patient and the responsibility to provide the appropriate pharmacotherapeutic guidelines, ensuring definitive results. The introduction of modern practices requires a better preparation of the pharmacist, so that he or she can provide more comfort and safety to patients. For this, the pharmacy degree curricula underwent changes and, in certain cases, increased the time to complete the training (Hanya et al., 2014). In Brazil, the minimum workload is 4,000 h, with the proportion of theoretical study ranging from 35 to 80% and practical study 20 to 65% (Brasil, 2013). Although, there is a slight increase in the disciplines considered in the area of ​​Human Sciences in the curricula of some Brazilian institutions (Brasil, 2013), other challenges and barriers that influence the domain of specific practical skills were also reported in the present research.
In the perception of these Brazilian students, some of the flaws in the process of preparing the pharmacist for patient-centered practice are the lack of practice scenarios, notably a teaching pharmacy and underutilization of the teaching hospital, the nature of the curriculum, teacher profile and in the choice of teaching method, culminating in failures in practical training for specific professional responsibilities. The teaching pharmacy is an extension of the pharmacy course, which functions as a mixed character space: a company laboratory, and can provide students with a variety of amenities, such as: teacher-led curricular stages, quality enhanced education, low-cost medication for university hospitals, integration of theory and practice, greater contact between students and the social reality of the community and the market, as well as the learning of responsibilities, skills, and creativity, both vital for the future of pharmacists (Rossignoli et al., 2004).
According to Mitre et al. (2008), in the teaching pharmacy environment, "the student ceases to be a passive recipient of content and the teacher assumes an educator, facilitator posture that allows and causes an active participation of the student in his learning process." There is a lack of a teaching pharmacy in 68% of the pharmacy courses, according to a report of the Advisory Commission of Pharmaceutical Education (Brasil, 2013). According to the report, this data allows us to infer that training in one of the areas that most employs pharmacists, when it happens, is being delegated to companies in industry, who may or may not be aware of their responsibility towards this future professional. Another teaching scenario demanded by the students was the University Hospital. In the analyzed institution, this scenario of practice is most effectively used by students of Medicine, Nursing, Physiotherapy, and Dentistry. Because pharmacy students study pharmacy and pharmacy, the respondents' claim is well-founded because they could integrate clinical teams, receive training, or even increase the number of classes in the hospital, have frequent and effective contact with patients, and access their records.
Regarding the specifications of the course analyzed, it was observed that in over 4,000 h, insufficient time is offered for some key disciplines, requiring more time to cover more content or more subjects, such as pharmacology and pharmaceutical care (much content and very little time). Lack of a professional discipline like pharmaceutical semiology was also treated as an opportunity less than acquiring skills and tailoring the students’ resumes. This discipline aims at enabling the application of previously acquired knowledge to the clinical investigation of signs and symptoms and in the resolution of minor disorders (Pedroso et al., 2014; Júnior et al., 2007). Blom et al. (2011) and Hassali et al. (2011) emphasize that often the curriculum needs to be renewed and updated for the current activities of the future pharmacist. Wertheimer (1991) and Harding and Taylor (1997) had already discussed the importance and necessity of including social pharmacy disciplines in the standard curriculum of universities. For Kassam and Volume-Smith (2003), the appropriate way to train pharmacists to satisfy the interests of society is through introducing the practice of pharmaceutical care into course programs.
Maynard et al. (2011) further suggest that students should be exposed to experiences and case studies in which patients suffer from multiple health problems, leaving students to identify untreated conditions and make appropriate treatment recommendations and develop monitoring plans for evolution of the clinical picture of the patient. Lyra Jr. (2005) emphasizes that clinical pharmaceutical practice associates clinical, communicative, critical, and informative knowledge necessary for the prevention, diagnosis, and treatment of problems related to medications. According to the International Pharmaceutical Federation (FIP), patient counseling could be seen as a pharmaceutical care activity, focusing on a patient-centered approach. This competence is even more required in countries such as the Netherlands, where pharmacists have patient consultations on topics related to drug safety (Kooy et al., 2007; Prideaux, 2007). It is emphasized that, although the tendency is to prepare the student to focus care on the patient, it is essential that the student has the competence to handle essential activities of the pharmacist in the day-to-day work of the community pharmacy, a fact pointed out by the students as one of the deficiencies of the analyzed course, with the perception that the course was very concerned with the technological and academic areas.
The curricular aspects mentioned demonstrate that the most reported problem is in fact the lack of practical experience and contact with real patients. Internships and professional disciplines have almost no practical focus or
contact with real patients, and there is sometimes an inconsistency between what is taught and the professional reality, according to interviewees, unlike what has been happening with pharmaceutical education in developed countries, such as the United States, European Union countries, and Malaysia, as reported by Scott et al. (2010) and Hasan et al. (2013). These two studies mention four-year courses, the fourth year being devoted to the practice of advanced pharmacy practice experiences (APPEs). In addition, it was reported that pharmacy students' confidence about the "knowledge" and "skills" aspects in pharmacotherapy increased during APPEs (Nykamp and Miller, 2011). The extension of pharmacy training to clinical pharmacy was also recommended by Ried et al. (2002) as an approach to improve the performance of pharmacists in patient-centered care activities, especially concerned with interaction, communication, and skills acquired after 9 weeks of work in hospital clinical pharmacy. Hanya et al. (2014) reported changes in 2006 in undergraduate pharmacy courses in Japan, an increase in duration of 4 to 6 years, after which the students performed a structured clinical examination objective (OSCE) to assess whether they had acquired clinical experience sufficient to participate in a clinical training for 5 months.
The students' statements included some behavioral factors, such as insecurity, fear, discouragement, frustration, and difficulty in dealing with unusual facts. It is clear that some of these aspects are interlinked, such as insecurity caused by lack of knowledge, generating anxiety, and even affecting verbal communication. Baldwin et al. (1979) found that more than 30% of pharmaceutical communication may be affected. The explanation for this problem was later presented by McCroskey (1984), who defined this phenomenon as the individual level of anxiety in actual communication, or anxiety in the case of potential communication, around being in contact with another person. The psychological barrier of pharmacy students in the contact with physicians and other health professionals is reported by Hasan et al. (2013) in a study involving community pharmacists. These authors call this feeling an uncomfortable situation arising from a psychosocial barrier that may be the result of an unfavorable hierarchical positioning of pharmacists versus physicians. In the same study, it was verified that the medical team showed a high rate of acceptance of interventions made by student pharmacists participating in the study. This shows that barriers may exist in the minds of pharmacists because they are not, or feel that they are not prepared, but can be eliminated as they gain experience and confidence.
It is important to emphasize that the skills of effective communication, both with patients and with other health professionals, are fundamental in pharmaceutical practice, as mentioned by Schwartzman et al. (2013) that place greater emphasis on communication as the focus of patient-centered courses of care. The students' claims are consistent with the recommendations of the World Health Organization, which argues that the pharmacist should be a knowledgeable and reliable communicator to establish a good relationship with other professionals and with the public in general (WHO, 1997). Communication training can be achieved by the simulation method known as role-playing, introduced by Barrows (1993) for the training of physicians, and currently used in other areas such as pharmacy, although it was not used as a methodology for the students interviewed. The practical experience of dealing with patients should be encouraged and trained throughout the course of pharmacy, occurring gradually from the beginning of the course and increasing year after year in a way that students could finish their course effectively prepared for the practice (Branch, 2014). At this point, it is essential that the internship can integrate skills and knowledge training, offering a real understanding of the profession based on practical experience (Hasan et al., 2013).
On the other hand, the internship is often seen as a requirement to fulfill a workload, without being aligned with the professional goals of graduation, causing a disconnection between what accumulates from experience and what one really wants to practice. For example, in a study by Maynard et al. (2011) at the Midwestern University Institutional Review Board, Chicago (USA), involving pharmacy students in their senior year, students spent 69% of the time practicing drug dispensing and only 10% practicing pharmaceutical care, and yet they wanted to work in the area for which they had less experience, as cited in Maynard et al. (2011). The profile of teachers has also been highlighted by students as one of the factors that hinder better preparation for patient-centered pharmaceutical practice. The crux of this problem may be in the hiring process. According to Rozendo et al. (1999), the criteria for teacher selection and employment consider only the teacher as a specialist in his or her field of knowledge and this teacher does not necessarily excel in pedagogical fields nor has a broader, more philosophical, or even more immediate point of view, technological point of view. Underlying this assertion is the assumption that didactic training is not so essential, because university students as adults subject to rigorous selection, are motivated to become professionals and so, a priori, are prepared to learn for themselves.
Teachers with advanced scientific abilities tend to teach their classes at a high level of abstraction and complexity, assuming that students are assimilating knowledge without worrying about real understanding or providing opportunities for students to participate in the construction of knowledge. This could require that the teacher leave his or her 'comfort zone,' and many are unwilling to compromise the accuracy of their formulations and adopt temporary and partial concepts that are closer to the students' knowledge (Villani and Pacca, 1997). The inadequate approach adopted by some teachers in presenting the program, and failing to emphasize practical applications, was among the students' complaints. In some ways, depending on the workload of the teachers and their teaching capacity, there is a tendency for the teacher to adopt a unilateral presentation of the content merely by lecturing, imposing the teacher’s "absolute truths," perpetuating the view of knowledge as a "copy" written in a tabula rasa according to Correia et al. (2001).
The statements of the interviewees show that there is dissatisfaction with the teaching method with excess theoretical lectures and as if the ultimate goal was to be successful in tests. The solid learning and conclusion in terms of theoretical content are questionable, in the opinion of the interviewees. This way of teaching, in fact, opposes learning that values ​​the student's role as an individual who has the ability to interact in the educational environment and needs to be "helped to discover for himself the knowledge he must learn and use the most adequate to the character and personality of each one" (Biggs, 1996). Contrasting this approach, the teacher can assume the role of mentor during learning, when strategies such as cooperative learning, case studies, or problem-based learning are used. The interrelationship between participants' points of view and consistency with the results of various studies leads us to the believe that students need to improve their skills. Information about pharmacy seniors' views on their education may be helpful in explaining the observed inconsistencies between pharmaceutical education and the realities of professional practice. Since the study involved only seniors on the pharmacy course, it can be concluded that almost all chances of acquiring the skills needed to tackle the job market have been exhausted. Solving the problem at source requires curricular reform.
LIMITATIONS AND PRACTICE IMPLICATIONS
The sample was not uniform in terms of gender. There was a female predominance among the participants by the very nature of the population. Furthermore, there is no guarantee that respondents were representative of their peers. In studies using the technique of focus groups the sessions should allow the doubts and opinions to be expressed. This can lead to a loss of focus and control in the discussions and, therefore, there is no way to predict the consequences; there is absolutely no determinism in this type of study. It is impossible to know whether participants express what they really think about the matter. In addition, there are cultural aspects that limit the scope of the study, because the way of thinking depends on ethical, moral, and religious values as well as on the family financial income or even broadly on country development level. Although the work has only involved students of pharmacy, the results can be useful for other professions, not only for university education but also for training in other healthcare settings.
The results achieved in this study revealed the main causes of the lack of skills needed for the pharmacy practice of pharmacy students, such as insufficient infrastructure, lack of a teaching pharmacy, and underutilization of the University Hospital, according to the pharmacy students who participated in the focus groups. On the other hand, the excess of theoretical concepts in the disciplines and the didactic and pedagogical shortcomings of teachers also contribute to overshadow the practical objectives of the pharmacy course. Despite the importance of managing the acquisition of skills identified for professional competence, the training of higher education teachers, especially outside their specializations, inappropriate teaching methods, and lack of focus on student learning, show that teaching is little systematic, far from the steps and strategies recommended and therefore highly likely to result in poor learning. By the present result, academic-professional development only occurs with the assimilation of knowledge, integration of abilities, and the adoption of relevant attitudes to provide a high professional performance. These qualities require curricular reformulation for the improvement of practical content in professional disciplines, making it possible to understand situational and experiential workplace factors, and to combine clinical and communication skills to make decisions and deal with patients' unpredictable behavior.
The authors have not declared any conflict of interests.
REFERENCES
|
Academic Medical Centers (2010). Pharmacy Practice Model.
|
|
|
|
Azhar S, Hassali MA, Ibrahim MIM, Ahmad M, Masood I, Shafie AA (2009). The role of pharmacists in developing countries: The currents cenario in Pakistan. Hum. Resour. Health 7(1):54.
Crossref
|
|
|
|
|
Baldwin HJ, McCroskey JC, Knutson TJ (1979). Communication apprehension in the pharmacy student. Am. J. Pharm. Educ. 43(2):91-3.
|
|
|
|
|
Bardin L. (1977).L'Analyse de contenu. Editora: Presses Universitaires de France.
|
|
|
|
|
Bardin L. (2011). Ánálise de conteúdo. SP: Edições 70.
|
|
|
|
|
Barrows HS (1993).An overview of the uses of standardized patients for teaching and evaluating clinical skills. Acad. Med. 68(6):443-51.
Crossref
|
|
|
|
|
Biggs JB (1996). Enhancing teaching through constructive alignment. Higher Educ. 32(3):47-364.
Crossref
|
|
|
|
|
Blom L, Wolters M, Ten Hoor-Suykerbuyk M, Van Paassen J,Van Oyen A (2011). Pharmaceutical education in patient counseling: 20 h spread over 6 years? Patient Educ Couns. 83(3):465-71.
Crossref
|
|
|
|
|
Bond C (2006).The need for pharmacy practice research. Int. J. Pharm. Pract. 14(1):1-2.
Crossref
|
|
|
|
|
Branch C (2014). An assessment of students' performance and satisfaction with an OSCE early in an undergraduate pharmacy curriculum. Curr. Pharm. Teach. Learn. 6(1):22-31.
Crossref
|
|
|
|
|
Brasil (2013). Conselho Regional de Farmácia do Estado de São Paulo.. Estudos de Matrizes Curriculares dos Cursos de Farmácia do Estado de São Paulo/ Conselho Regional de Farmácia do Estado de São Paulo. – São Paulo: Conselho Regional de Farmácia do Estado de São Paulo. 47p.
|
|
|
|
|
Brasil (1996). Lei Federal nº 9394, de 20 de dezembro de 1996.. Available at:
View.
|
|
|
|
|
Brasil (2002). Ministério da Educação e Cultura. Resolução CNE/CES 2, de 19 de fevereiro de 2002. Available at:
View.
|
|
|
|
|
Correia MFB, Lima APB, Araújo CR (2001). As contribuições da psicologia cognitiva e a atuação do psicólogo no contexto escolar. Psicol Reflex Crit. 14(3):553-61.
Crossref
|
|
|
|
|
De Oliveira RD (2011). Por uma formação crítico-humanista do profissional da atenção farmacêutica: Um ensaio reflexivo. Red Sudam Aten Farm. Available at:
View
|
|
|
|
|
Earl G, Reinhold JA (2014). Approach to the patient and patient-centered care process. In: Earl, G, Reinhold, JA (Eds.) Clinical Therapeutics Primer: Link to the Evidence for the Ambulatory Care Pharmacist. Jones & Bartlett Publishers: United States of American. 300p. Available at:
View).
|
|
|
|
|
Fernandes ZC (2014). Diretrizes Curriculares: Necessidade de ajustes. Pharm Bras. 88 (1):25-28. Available at:
View
|
|
|
|
|
Fuhrman Jr LC, Buff W, Baddy M, Dollar M (2001). Utilization of an integrated interactive virtual patient database in a web-based environment for teaching continuity of care. Am. J. Pharm. Educ. 65(3):271-275.
|
|
|
|
|
Hanlon JT, Weinberger M, Samsa GP, Schmader KE, Uttech KM, Lewis IK, Cowper PA, Landsman PB, Cohen HJ, Feussner JR (1996). A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am. J. Med. 100(4):428-437.
Crossref
|
|
|
|
|
Hanya M, Yonei H, Kurono S, Kamei H (2014). Development of reflective thinking in pharmacy students to improve their communication with patients through a process of role-playing, video reviews, and transcript creation. Curr. Pharm. Teach. Learn. 6(1):122-129.
Crossref
|
|
|
|
|
Harding G, Taylor K (1997). Responding to change: the case of community pharmacy in Great Britain. Sociol Health Illn. 19(5):547-60.
Crossref
|
|
|
|
|
Hasan SS, Wong PS, Ahmed SI, Chong DWK, Mai CW, Pook P, Kairuz T (2013). Perceived impact of clinical placements on students' preparedness to provide patient-centered care in Malaysia. Curr Pharm Teach Learn. 5(4):303-310.
Crossref
|
|
|
|
|
Hassali MA, Shafie AA, Al-Haddad MS, Abduelkarem AR, Ibrahim MI, Palaian S, Abrika OS (2011). Social pharmacy as a field of study: The needs and challenges in global pharmacy education. Res. Social Adm. Pharm. 7(4):415-420.
Crossref
|
|
|
|
|
Ivama AM (1999). La Educación y La Práctica Farmacéutica en Brasil y Espa-a e nel Contexto de La Globalización. Alcalá de Henares: Universidad de Alcalá; [tesis doctoral]
|
|
|
|
|
Júnior DPL, Kheir N, Abriata JP, Rocha CE, Santos CB, Pelá IR (2007). Impact of Pharmaceutical Care interventions in the identification and resolution of drug-related problems and on quality of life in a group of elderly outpatients in Ribeirão Preto (SP), Brazil. Ther. Clin. Risk Manag. 3(6):989-998.
|
|
|
|
|
Kassam R, Volume-Smith CI (2003). Focus group methodology to develop a community pharmaceutical care clerkship program. Am. J. Pharm Educ. 67(3):1-20. Available at: http://archive.ajpe.org/aj6703/aj670388/aj670388.pdf.
Crossref
|
|
|
|
|
Kooy MJ, Dessing, WS, Kroodsma EF, Smits SR, Fietje EH, Kruijtbosch M, De Smet PA (2007). Frequency and determinants of pharmaceutical consultations provided in private by Dutch community pharmacists. Pharm. World Sci. 29:81-9.
Crossref
|
|
|
|
|
Koster ES, Blom L, Philbert D, Rump W, Bouvy ML (2014) The Utrecht pharmacy practice network for education and research: A network of community and hospital pharmacies in the Netherlands. Int. J. Clin. Pham. 36(4):669-674.
Crossref
|
|
|
|
|
Krueger RA, Casey MA (Eds.) (2000). Focus groups: A practical guide for applied research London: Sage. 3rd ed. 215p.
Crossref
|
|
|
|
|
Krupicka MI, Bratton SL, Sonnenthal K, Goldstein B (2002). Impact of a pediatric clinical pharmacist in the pediatric intensive care unit. Crit. Care Med. 30(4):919-921.
Crossref
|
|
|
|
|
Lyra Junior DP (2005). Impacto de um programa de Atenção Farmacêutica, no cuidado de um grupo de idosos atendidos na Unidade Básica Distrital de Saúde Dr. Ítalo Baruffi, Ribeirão Preto (SP) [tese]. [Ribeirão Preto]: Faculdade de Ciências Farmacêuticas de Ribeirão Preto/USP. Available at:
View
|
|
|
|
|
Maynard RA, Wagner ME, Winkler SR, Montuoro JL (2011). Assessment of student pharmacists' perceptions on participating in clinical services in the community pharmacy setting. Curr. Pharm. Teach. Learn. 3(2):123-136.
Crossref
|
|
|
|
|
McCroskey JC. (1984). The communication apprehension perspective. In: Dally JA, McCroskey JC (Eds.), Avoiding Communication: shyness, reticence, and communication apprehension. Sage, Beverly Hills, CA. 296p. Available at:
View.
|
|
|
|
|
McKee M, Frei BL, Garcia A, Fike D, Soefje SA (2011). Impact of clinical pharmacy services on patients in an outpatient chemotherapy academic clinic. J. Oncol. Pharm. Pract. 17(4):387-394.
Crossref
|
|
|
|
|
Mitre SM, Siqueira-Batista R, Girardi-de-Mendonça JM, Morais-Pinto NM, Meirelles CAB, Pinto-Porto C, Moreira T, Hoffmann LMA (2008). Metodologias ativas de ensino-aprendizagem na formação profissional em saúde: debates atuais. Cienc Saude Colet. 13(2):2133-2144.
Crossref
|
|
|
|
|
Nicoleti MA (2010). O ensino Farmacêutico Atual: Uma Reflexão. Revista Educação 5(2):5-15
|
|
|
|
|
Nykamp D, Miller SW (2011). Pharmacy student and preceptor perceptions for the first advanced pharmacy practice experience. Curr. Pharm. Teach. Learn. 3(1):9-16.
Crossref
|
|
|
|
|
Oliveira AB, Oyakawa CN, Miguel MD, Zanin SMW, Montrucchio DP, Prehs D (2005). Obstáculos da atenção farmacêutica no Brasil. Braz J. Pharm. Sci. 41(4):409-413. Available at:
View
|
|
|
|
|
Papadopoulos J, Rebuck JA, Lober C, Pass SE, Seidl EC, Shah RA, Sherman DS (2002). The critical care pharmacist: An essential intensive care practitioner. Pharmacotherapy 22 (11):1484-1488.
Crossref
|
|
|
|
|
Pedroso TM, Mastroianni PC, Santos JL (2014). Semiologia Farmacêutica e os desafios para sua consolidação. Rev. Eletronica Farm. pp. 55-69.
Crossref
|
|
|
|
|
Prideaux D (2007). Curriculum development in medical education: from acronyms to dynamism. Teach. Teach. Educ. 23(3):294-302.
Crossref
|
|
|
|
|
Richir MC, Tichelaar J, Geijteman ECT, De Vries TPGM (2008). Teaching clinical pharmacology and therapeutics with an emphasis on the therapeutic reasoning of undergraduate medical students. Eur J. Clin. Pharmacol. 64 (2):217-24.
Crossref
|
|
|
|
|
Ried LD, Brazeau GA, Kimberlin C, Meldrum M, McKenzie M (2002).Students' perceptions of their preparation to provide pharmaceutical care. Am. J. Pharm. Educ. 66(4):347-3.
|
|
|
|
|
Rossignoli P, Correr CJ, Fernández-Llimós F (2004). Interés de los alumnos en las actividades de prácticas tuteladas en farmacia escuela en Curitiba-Brasil. Seguim Farmacoter 1(2): 62-8. Available at:
View.
|
|
|
|
|
Rozendo CA, Casagrande LDR, Schneider JF, Pardini LC (1999). Uma análise das práticas docentes de professores universitários da área de saúde. Rev Latino-Am Enfermagem. 7(2):15-23.
Crossref
|
|
|
|
|
Sarrif A, Nordin N, Hassali MAA (2012). Extending the roles of community pharmacists: Views from general medical practitioners. Med. J. Malays. 67(6):577-781.
|
|
|
|
|
Schwartzman E, Chung EP, Sakharkar P, Law AV (2013). Instruction and assessment of student communication skills in US and Canadian pharmacy curricula. Curr. Pharm. Teach. Learn. 5(6):508-517.
Crossref
|
|
|
|
|
Scott DM, Friesner DL, Miller DR (2010). Pharmacy students' perceptions of their preparedness to provide pharmaceutical care. Am J Pharm Educ. 74 (1): 8.
Crossref
|
|
|
|
|
Silva WB (2009). A emergência da atenção farmacêutica: Um olhar epistemiológico e contribuições para o seu ensino.Florianópolis. 2009. 305p. [Thesis of PhD degree. Federal University of Santa Catarina]. Available at:
View.
|
|
|
|
|
Troncon LEA (2007). Utilization of simulation patients for clinical skills teaching and assessment. Medicina Ribeirão Preto 40:180-191. Available at:
View
|
|
|
|
|
Villani A, Pacca JLA (1997). Construtivismo, conhecimento científico e habilidade didática no ensino de ciências. Rev. Fac. Educ. 23(1-2):1-12. Available at:
View.
|
|
|
|
|
Wertheimer A (1991). Social/behavioural pharmacy: The Minnesota experience. J. Clin. Pharm. Ther. 16(6):381-383.
Crossref
|
|
|
|
|
World Health Organization (WHO) (1997). The role of the pharmacist in the health care system: preparing the future pharmacist. Vancouver: WHO. Available at:
View.
|
|