Full Length Research Paper

ABSTRACT
The objective of this study was to contribute to the improvement of medical prescription of antimalarials at Kisangani University Clinics. This a cross-sectional study with retrospective data collection, based on 200 medical prescriptions from patients aged 3 days to 80 years, treated for malaria from March to December 2019. The study took place between March and May, 2020. Sixty one percent of patients suffered from uncomplicated malaria and 39% from severe malaria. Information on the total quantity of medicines to be taken, the dose, the rate of administration and the duration of the treatment were not mentioned respectively in 6.5, 15.5, 5.5 and 14.5% of prescriptions. No prescription mentioned the qualification of the prescriber or his phone number. The prescribed antimalarial was not appropriate in 15.5% of prescriptions in that artesunate and artemether were used to treat uncomplicated malaria. Artesunate was slightly more prescribed than quinine for severe malaria (55.4 versus 44.6%). The prescribed dose and duration of treatment were inadequate in 4.7 and 0.6% of the prescriptions, respectively. Twenty point seven percent (20.7%) of the overall prescriptions were found to be non-compliant. The medical prescriptions of antimalarial drugs issued to patients at the university clinics of Kisangani do not always comply with national regulations and directives in this area. Although these deficiencies appear to be minimal, they might lead to ineffective treatment, treatment failures and recurrence of malaria. Prescribers should be regularly retrained as to this.
Key words: Malaria, prescription practices, antimalarials, treatment guidelines, policy adherence, Tshopo, Democratic Republic of Congo.
INTRODUCTION
Malaria is endemic in the Democratic Republic of Congo (DRC), where it is the main cause of morbidity and mortality (NMCP, 2017; PMI, 2019; SMO, 2019). In 2018, the DRC was in second place in terms of the number of malaria cases and associated death worldwide (12% cases and 11% deaths), and accounted for 54.6% of cases in Central Africa (WHO, 2019). The 2019 annual report of National Malaria Control Program (NMCP) reports more than twenty-one million cases of malaria including nineteen million cases of uncomplicated malaria and two million cases of severe malaria as well as thirteen thousand and seventy-two deaths related to malaria (Lusimana, 2020). The curative treatment of malaria involves the use of antimalarial drugs, and World Health Organization (WHO) and the NMCP recommend protocols for the management of this disease (NMCP, 2016 ; NMCPsn, 2018; WHO, 2018a). However, despite the availability of these protocols, the burden of morbidity and mortality from malaria remains significant. According to WHO estimates, more than half of drugs, including antimalarials, are not prescribed, dispensed or sold properly. In developing countries, only 30 to 40% of patients are treated according to official guidelines. In addition, only 50% of people suffering from malaria receive the recommended first-line antimalarials (Soumana et al., 2016). The study conducted by Kangudia et al. (2017) in Kinshasa has shown, concerning the prescription of antimalarials in early pregnancy, that many doctors ignore and/or do not respect the recommendations of the NMCP. Indeed, different problems can arise when prescribing an antimalarials, for instance the non-compliance with regulations, the prescription of a molecule that is not recommended or not appropriate, the prescription of an appropriate molecule but at an inadequate dose, the prescription of molecule that is unsuitable for the patient because of an adverse reaction or the prescription of a molecule not justified because not indicated for the patient.
In order to preserve the efficacy of antimalarial and reduce the morbidity and mortality associated with malaria, it is important that the prescription of antimalarials be in accordance with established protocols, since non-compliant prescribing can be responsible for treatment failures and the phenomenon of malaria resistance (Kamuhabwa and Silumbe, 2013 ;WHO, 2015). The development of resistance to antimalarial drugs which poses as one of the greatest threats to malaria control and results in increased malaria morbidity and mortality (Menard and Dondorp, 2017).
Studies on the compliance of antimalarial prescriptions with national regulations and guidelines in the province of Tshopo are scarce. In order to contribute to the awareness of prescribers in the DRC in general and in the province of Tshopo in particular, we carried out the present study on the analysis of medical prescriptions of antimalarials to investigate whether the prescription of antimalarials to patients consulting at Kisangani university clinics do comply with national regulations and guidelines. The overarching goal of the study was to contribute to the improvement of medical prescriptions of antimalarial drugs at the Kisangani university clinics (KisUC).
POPULATION AND METHODS
Type of study and period
This is a crossing-sectional study with retrospective data collection that took place between March and May 2020, in the KisUC archives service. The KisUC constitute a university hospital center, the only tertiary level medical training in the city of Kisangani.
Population and study sample
The study comprised patients aged from 3 days to 80 years, who consulted during the period from March to December 2019 for malaria and who received at least one antimalarial. Inclusion criteria were included the medical files of patients who consulted in internal medicine, gynecology-obstetrics and pediatrics departments of the KisUC for malaria and who received at least one antimalarial. Non-inclusion criteria were medical files with illegible drug names were discarded.
Two hundred and fifty patient medical files containing antimalarial prescriptions were consulted and 190 files were retained.
Data collection
Files of patients who consulted for malaria were used to collect information. The socio-epidemiological and clinical data of the patient, the drugs prescribed to the patient as well as the qualification of the prescriber were collected. Age and sex of patient, clinical status (type of malaria), medication prescribed, dose prescribed, duration of treatment, and prescriber qualification were the variables studied.
Verification of compliance with the regulations
Compliance with the regulations was attested by the presence of the following information: qualification of the prescriber, his signature and his phone number, date of prescription, age, sex and weight of the patient, name of drug prescribed in the international nonproprietary name (INN), strength, pharmaceutical form, total amount, dose, rate and route of administration of the prescribed drug, and duration of treatment.
Criteria for non-compliance of the antimalarial prescription
The prescription was deemed to be inconsistent with established protocols in one of the following cases: prescription of an inappropriate antimalarial; prescription of an unjustified molecule; prescription of an unsuitable molecule; prescription of an antimalarial in inadequate doses: under dosage or overdosage; duration of treatment not observed: less than three days for artemisinin-based combinations therapy (ACT) and five days for quinine.
Treatment protocol recommended by the National Malaria Control Program
In the case of uncomplicated malaria, both recommended ACTs are artemether- lumefantrine or artesunate-amodiaquine; they must be prescribed for three days. The recommended doses are as follows:
1. Artemether-lumefantrine: 1.7 mg/kg/day for artemether and 12 mg/kg/day for lumefantrine.
2. Artesunate-amodiaquine: 4 mg/kg/ day of artesunate and 10 mg/kg/day of amodiaquine.
In severe malaria, injectable artesunate is prescribed at a dose of 2.4 mg/kg on admission (t = 0), then 12 h and 24 h later and, thereafter, once a day until the patient can take their oral medication. The follow-up treatment is quinine tablet at a dose of 10 mg/kg three times a day every 8 h. Quinine infusion is prescribed if artesunate is not available.
Definition of concepts
An inappropriate antimalarial is defined as an antimalarial not recommended by the national malaria management protocol. An unsuitable molecule is defined as a molecule that can cause an adverse reaction in the patient.
An unjustified molecule is defined as a molecule indicated for pathology other than that from which the patient suffers.
Ethical aspects
An authorization from the KisUC management has been obtained. In addition, anonymity and confidentiality have been guaranteed for all information collected.
Statistical analysis of data
Data processing and analysis was performed using Excel 2010 and IBM SPSS Statistics version 23 software. The qualitative variables are expressed as a proportion and quantitative variables as the mean ± standard deviation. For socioepidemiological and clinical characteristics, the chi-square test was used to compare the proportions. P < 0.05 was considered to be statistically significant.
The average number of drugs per prescription was determined by the formula below:

RESULTS
Socioepidemiological and clinical characteristics
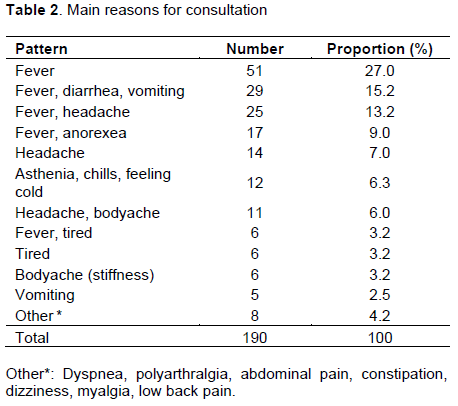
The files of 190 patients were consulted. These patients came from 4 communes in the city of Kisangani. Among them, 15.8% were aged from 0 to 5 years; 15.3% were aged 6 to 15 years and 68.9% were aged 16 years and over. The average age was 18.2 ± 13.1 years old with extremes of 3 days and 80 years. The sex ratio was 0.54 M/F. Of the 84 adult female patients 19 were pregnant and 23 were breastfeeding. Malaria was confirmed by microscopic examination, with a positive thick film or by a positive rapid diagnostic test (RDT). Sixty-one percent of patients suffered from uncomplicated malaria and 39.0% from severe malaria. These data are displayed in Table 1. Fever was the main reason for consultation. Table 2 shows different reasons for consultation.

Verification of compliance with regulations
Two hundred medical prescriptions containing antimalarial treatment were retrieved from patient files. In all these prescriptions, mentions such as the signature of the prescriber, the date of the prescription, the age, sex and weight of the patient were mentioned. However, none of them indicated the qualification of the prescriber. More than 80% of drugs were prescribed in INN, the pharmaceutical forms and the routes of administration were always indicated. However, the total quantity of drugs to be taken, the dose, the rate of administration and the duration of treatment were mentioned in 93.5, 84.5, 94.5, and 85.5% of prescriptions respectively. The proportion of prescriptions bearing the particulars required by the regulations is shown in Table 3.

Conformity of antimalarial prescriptions
Out of the 200 antimalarial prescriptions analyzed, 79.3% were found to comply with the treatment protocol recommended by the NMCP and 20.7% were non-compliant. The prescription of antimalarial drugs was based, in 62.6%, on the results of the thick drop analysis and in 37.5% on the RDT. Table 3 shows that the errors encountered are the prescription of inappropriate antimalarial drugs (15.5%), prescription of inadequate doses (4.7%) and non-compliance with the duration of treatment (0.6%). We listed 63.0% of prescriptions for uncomplicated malaria and 37% for severe malaria. In 75.4% of prescriptions for uncomplicated malaria, ACT, artemether-lumefantrine was prescribed; artemether, 23.8%; and artesunate, 0.8% were prescribed. In contrast, in severe malaria, artesunate or quinine were prescribed, and an antibiotic was associated in 90.5% of prescriptions for severe malaria. Artesunate was prescribed in 55.4% of prescriptions and quinine in 44.6%. In 84.5% of prescriptions, the prescribed molecule was appropriate. The prescribed dose was correct in 161/169 prescriptions (95.3%) and inadequate in 8/169 (4.7%). More than 3/4 of the inadequate doses were for under dosage (87.5%) versus (12.5%) for the overdose. The duration of treatment was respected in 99.4% of the prescriptions (170/171 prescriptions) and not respected in 0.6% (Table 4).

The average number of drugs per prescription was 2.3 with ranges of extremes of 2 to 4. Twenty-seven point five (27.5) percent of prescriptions contained more than 3 drugs. Prescriptions with 4 drugs were established for severe malaria. In 55.0% of prescriptions, the tablet form was prescribed the most, followed by the solution for injection form (45.0%).
DISCUSSION
The patients included in this study came from 4 out of the 6 communes of the city of Kisangani. Unlike other authors who have reported a predominance of children under 5 years of age in the population of patients with malaria (Djire, 2009; Soumana et al., 2016), in this study, 2/3 of the patients were adults (69%). This difference could be due to the fact that the present study was carried out in 3 departments of KisUC namely internal medicine, pediatrics and gynecology, whereas the above-mentioned authors conducted their studies in the pediatric department and targeted children aged 0 months to 15 years. Different symptoms prompted patients to consult, but fever alone or in combination with other symptoms was the main reason for consultation (67.4%). In fact, malaria begins with a fever, which may or may not be accompanied by headaches, muscle pain, weakness, vomiting (Menan, 2007; Pastor Institute, 2019). The proportion of 67.4% is slightly higher than that of Djire who also found that fever was the first reason for consultation for 46.7% of patients (Djire, 2009). This difference could be due to the characteristics of the study population. Regarding the type of malaria, 61% of patients consulted for uncomplicated malaria and 39% for severe malaria. Our results are close to those of Soumana et al who reported 86% cases of uncomplicated malaria cases and 24% cases of severe malaria in their study carried out in Niger (Soumana et al., 2016). However, they are far different from those reported in our previous study carried out at the Makiso-Kisangani General Referral Hospital (GRH/Makiso-Kisangani), where the number of severe malaria cases was higher than that of uncomplicated malaria, respectively 71.5 and 28.5%. Sixty nine point nine percent of patients were children (Nsuadi-Manga et al., 2020). We would like to point out that unlike KisUC which are located at the tertiary level of the health pyramid, the GRH/Makiso-Kisangani is located at the secondary level. The number of uncomplicated and severe malaria cases in the present study is also different from those found by Tené et al. in a study carried out in Burkina-Faso, in a reference university hospital center. The latter targeted children aged 0 months to 15 years and reported 97.22% of cases of severe malaria and 2.78% of cases of uncomplicated (Tené et al., 2015). The difference could be due to the characteristic of our sample of which 69% of the patients were aged over 15 years, whereas in the above-mentioned studies it was the children who were more numerous. In addition, 52.6% of the patients in the present study lived in Makiso commune, a municipality where many intellectuals reside. It is possible that they get proper treatment as soon as they have malaria symptoms. However, no statistically significant difference was observed between the type of malaria and the commune of residence (P = 0.182, data not shown). The high proportion of uncomplicated malaria cases in this study could mean that patients consult directly when different symptoms appear or when fever persists and they do not wait for the situation to worsen. This retrospective study was carried out from medical files; we were not in direct contact with patients to obtain information such as the level of education, the occupation, the monthly income, the health insurance that could help us to identify the main contributory factors to these differences.
Analysis of the form of the prescriptions established at KisUC informs that the particulars required by the regulations such as the signature of the prescriber, the prescription date, the age, sex and the weight of the patient, the name of drug prescribed, the pharmaceutical form, the quantity of drug, the route and rate of administration were included in almost all prescriptions. However, no prescriber had mentioned his qualification. Although in this study all the prescribers were doctors, it’s important for the prescriber to state his or her qualification or specialization. The qualification of the prescriber is important especially for drugs with limited prescription. Otherwise, this study was carried out in internal medicine, gynecology-obstetrics and pediatrics departments of the KisUC but no prescriber reported his specialization. Information on duration of treatment, dose and dosage were not reported in 14.5%, 15.5 and 38.0% of prescriptions, respectively. These routine elements are important in preventing and combating abuse (Calop et al., 2012). In 81.0% of the medical prescriptions, the drugs were prescribed in INN versus 19.0% of prescriptions where they were prescribed under the trade name or the specialty name. This percentage of INN prescriptions is slightly lower than that reported in our previous study where 93.2% of antimalarial drugs were prescribed under their INN (Nsuadi-Manga et al., 2020). Indeed, the INN prescription is the recommended one (WHO, 2013). Specialties are expensive; their prescription to a poor population prevents them from obtaining them with the consequence of non-compliance with treatment and progression of the disease to severe forms. The prescription of antimalarial in INN should be encouraged, since malaria is endemic in the DRC, a country characterized by the poverty of its population (WHO, 2018b). These drugs are indeed effective and their very advantageous cost allows the population to obtain them and to follow the treatment. Also, prescribing in INN limits the risks of confusion between several substances, facilitates the identification of duplicate and cumulative doses and offers the patient the possibility to benefit from his treatment without risk of error (Ministry of Solidarity and Health, 2016). This analysis reveals that the standard rules for writing medical prescriptions are not always followed by KisUC prescribers and that effort must be made by the latter to comply with legal requirements when prescribing. Failure to respect the duration of treatment in the prescriptions that mentioned it was observed in 1 prescription of artesunate. In 84.5% of prescriptions, the prescribed antimalarial was appropriate, that is it conforms to that recommended by the NMCP for the type of malaria and not appropriate in 15.5%. This proportion of inappropriate antimalarial prescriptions is almost double that found in our previous study (8.9%) (Nsuadi-Manga et al., 2020). This could be due to the fact that the prescribers of KisUC use to treat uncomplicated malaria not only artesunate, a drug recommended for severe malaria, but also artemether (not recommended by the NMCP), a drug widely available in many Africans countries (Esu et al., 2019).
Of the 200 prescriptions, 63% were for uncomplicated malaria and 37% for severe malaria. In the DRC, national guidelines recommend the use of injectable artesunate and quinine in cases of artesunate deficiency for severe malaria, and ACTs (artesunate-amodiaquine and artemether-lumefantrine) for uncomplicated malaria (Losimba-Likewla et al., 2018; NMCP, 2016; NMCP, 2017). In this study, injectable artesunate or quinine was prescribed for all patients with severe malaria. Artesunate was prescribed slightly more than quinine (55.4 versus 44.6%). This could be understood from the fact that artesunate injection is recommended to treat adults and children with severe malaria (Esu et al., 2019), while quinine is an alternative and a relay treatment. This shows that many prescribers comply with national guidelines for the management of severe malaria. In 90.5% of the prescriptions for severe malaria, an antibiotic was added to the antimalarial treatment. This proportion is far greater that found in the study by Diallo et al. (2017) carried out in Mali where an antibiotic was associated in 55% of antimalarial prescriptions for severe malaria. This strong use of antibiotics could be justified by the presence of bacterial co-infections in patients consulting KisUC for severe malaria. Moreover, the literature reports that severe malaria can promote bacterial co-infections which themselves complicate severe malaria (Bruneel et al., 2010). For treatments against uncomplicated Plasmodium falciparum malaria in most malaria endemic areas, artemisinin-based combination therapies (ACT) are used (WHO, 2018a). Two ACTs are recommended in the DRC, namely “artemether-lumefantrine” and “artesunate-amodiaquine”. In this study, only artemether-lumefantrine was used as a recommended ACT in uncomplicated malaria, artemether but also injectable artesunate were prescribed in proportions of 75.4, 23.8 and 0.8% respectively. And yet, artesunate and artemether are not recommended in the protocol for the management of uncomplicated malaria in DRC (Losimba-Likewla et al., 2018; WHO, 2018a). The combination “artemether-lumefantrine” was also the most commonly prescribed combination in the management of uncomplicated malaria in a study carried out in Mali (Doumbia, 2019). This high frequency could be explained by the fact that this combination is slightly better tolerated than the “artesunate-amodiaquine” combination (Ibrahima et al., 2020). Artesunate is reserved for severe cases, its use in uncomplicated malaria may lead to treatment failure when the same molecule must be used for severe cases of malaria. Artemether, an alternative artemisinin drug, is used in many African countries for the treatment of severe malaria although it is not specifically recommended by the WHO (Esu et al., 2019). The use of these molecules in uncomplicated malaria does not comply with the NMCP guidelines which stipulate that 100% of patients with confirmed malaria should receive treatment in accordance with national guidelines at all levels of health facilities (Losimba-Likewla et al., 2018). This study shows that national guidelines are not always followed by certain prescribers of KisUC. We also found dose mismatch in 4.7% of prescriptions. This inadequacy was observed in the management of uncomplicated malaria and concerned both under dosage and overdose, but the under dosage was predominant (that is 4.1 versus 0.6%). The under dosing was due to the fact that the prescribers did not take the patient's weight into account. Compared to the 18.6% of prescriptions with inadequate doses found by Soumana et al. (2016) and at 9.8% reported in our previous study (Nsuadi-Manga et al., 2020), the percentage of prescriptions with inadequate dose found in the present study is relatively low. However, there is still room for improvement because to cure malaria a sufficient dose of antimalarials is recommended. When a patient receives less medication than expected, treatment may fail. On the other hand, a higher dose than can be tolerated by the body could exacerbate its side effects and cause the patient to stop treatment.
As for the duration of treatment, it was not always indicated. In the prescriptions where it was mentioned, we found 1 prescription out of 171 with an incorrect duration of treatment. This was artesunate prescribed for 3 days without being followed by ACT treatment. This proportion is low compared to that found by Soumana et al. (10.46%) and that in our previous study (8.8%) (Soumana et al., 2016; Nsuadi-Manga et al., 2020); it indicates that the vast majority of prescribers of KisUC respect the duration of antimalarial treatment. This should be encouraged because non-compliance can be at the origin of resistance and repeated crises of malaria. The tablet and injectable solution forms were the most prescribed forms, respectively in 55 and 45% of prescriptions. These results corroborate those found in our previous study where we found 54.8% for tablets and 44.9% for injectable solutions. The significant use of the injectable solution form could be explained by the prescription of injectable artemether in uncomplicated malaria, and that of the tablet form, by the fact that it is used in uncomplicated malaria but also in severe malaria in relay to parenteral treatment. Note that in this study, the number of cases of severe malaria is about half that of simple malaria (39 versus 61%). The average number of drugs per prescription was 2.3. This number is close to and is roughly in line with the International Network for Rational Use of Drugs (INRUD) indicators which state that a good medical prescription should have an average number of 1.2 to 2 drugs (Nzolo and Mulongo, 2013) and far better than the averages of 4.8 and 8 drugs per prescription found respectively by Nsuadi et al. (2020), and Tsakala et al in a study carried out in Kinshasa on the evaluation of prescriptions in the treatment of malaria and gastroenteritis in hospitals, which reported an average of 8 drugs per prescription (Tsakala et al., 2005). Twelve out of 74 prescriptions for severe malaria included 4 products. The literature reports that taking four or more drugs can have negative consequences, due to the accumulation of potential side effects and interactions. Although not all drug interactions are clinically problematic, their number increases exponentially with the amount of drugs prescribed (Neuner-Jehle, 2016).
Analysis of the antimalarial prescriptions indicates that 20.7% of prescriptions were non-compliant. These results corroborate those of Soumana et al. in the study carried out at the Lamordé National Hospital in Niamey, and of Nsuadi et al. in the study conducted at the GRH/Makiso-Kisangani. They found 29.3 and 27.5% respectively of non-compliant prescriptions (Soumana et al., 2016; Nsuadi-Manga et al., 2020). The non-compliant prescription of antimalarials has several negative consequences, including treatment failure, waste of material and financial resources, with patient dissatisfaction. It is also a factor favoring the development of resistance of Plasmodium falciparum to antimalarials. Although no prescription of an unsuitable molecule or unjustified molecule was found in the antimalarial prescriptions established at KisUC, this study shows that these prescriptions have, in addition to regulatory non-compliance issues, drug therapy-related issues that can affect the efficacy and safety of treatment. These problems mainly relate to the inadequacy of doses and regimen, and failure to respect the duration of treatment.
This study complements the first study carried out in the city of Kisangani on the analysis of medical prescriptions, and contributes to enriching the limited amount of data that exist on the compliance of antimalarial prescriptions with national regulations and guidelines in health institutions in the city of Kisangani. This study focused on medical files, and therefore we were not able to come into direct contact with the nursing staff or the patients, to have more information, in particular on the choice of antimalarial prescribed and the achievement of pharmacotherapeutic results.
CONCLUSION
This study shows that the medical prescriptions of antimalarial issued to patients at Kisangani University Clinics do not always comply with national regulations and guidelines in this area. Although the problems identified appear to be small in magnitude, they should not be minimized because these deficiencies in the prescriptions can lead to ineffective treatment, the occurrence of treatment failures and recurrence of malaria. Prescribers should do more to improve their practice.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGMENTS
The authors are grateful to the managers of the University Clinics of Kisangani who allowed this study within their institution and to the administrative staff of the archives service for their collaboration.
REFERENCES
|
Bruneel F, Tubach F, Corne P, Megarbane B, Mira JP, Peytel E, Camus C, Schortgen F, Azoulay E, Cohen Y, Georges H, Meybeck A, Hyvernat H, Trouillet JL, Frenoy E, Nicolet L, Roy C, Durand R, Le Bras J, Wolff M (2010). Severe imported falciparum malaria: a cohort study in 400 critically ill adults. PloS One 5(10):e13236. |
|
|
Calop J, Limat S, Fernandez C, Aulagner G (2012). Clinical and Therapeutic Pharmacy. 4th edition. Elsevier-Masson: 1336 pp. |
|
|
Diallo T, Denou A, Coulibaly BF, Dakouo B, Coulibaly B (2017). Dispensing of antimalarial drugs in private pharmacies in the district of Bamako, Mali. Anthropo 37: 161-168. |
|
|
Djire A (2009). Study of antimalarial drugs used in the pediatric department of the CHU Gabriel Touré from September 2008 to February 2009. Thesis. Faculty of Medicine, Pharmacy and Ondostomatology, University of Bamako. |
|
|
Doumbia M (2019). Analysis of the prescription and dispensing of therapeutic combinations based on artemisinin (CTA in 6 pharmacies in the district of Bamako). Thesis. Faculty of Pharmacy. University of Sciences, Techniques and Technologies of Bamako. |
|
|
Esu EB, Effa EE, Opie ON, Meremikwu MM (2019). Use of artemether in the treatment of severe malaria. |
|
|
Ibrahima I, Laminou IM, Adehossi E, Maman D, Boureima S, Harouna HK, Hamidou HH, Mahamadou A, Yacouba I, Hadiza J, Tidjani IA (2020). Safety and Efficacy of Artemether-Lumefantrine and Artesunate-Amodiaquine in Niger. Bulletin de la Societe de Pathologie Exotique (1990), 113(1):17-23. |
|
|
Kamuhabwa AAR and Silumbe R (2013). Knowledge among drug dispensers and antimalarial drug prescribing practices in public health facilities in Dar es Salaam. Drug, Healthcare and Patient Safety 5:181-189. |
|
|
Kangudia MJ, Mbanzulu PN, Bangambe BJ, Kabala D, Messia G, Monzango GL, Mangbele JA (2017). Compliance with prescriptions for antimalarial drugs in the first trimester of pregnancy by doctors in Kinshasa. Kisangani Médical 7(2):296-300. |
|
|
Losimba-Likewla J, Emina J, Begu-Mbolipay J, Karamere J, Kakesa O, Nana I, Humes M, Ye Y (2018). Assessment of the impact of malaria control interventions on all-cause mortality among children under five in the Democratic Republic of the Congo from 2005 to 2015. Report. DRC Impact Assessment Group. |
|
|
Lusimana B (2020). Fight against malaria: the DRC has finalized its strategic plan 2020-2023. |
|
|
Menard D, Dondorp A (2017). Antimalarial Drug Resistance: A Threat to Malaria Elimination Cold Spring Harbor Perspectives in Medicine 7(7):a025619 |
|
|
Menan EIH., Yavo W, Oga SSA, Kiki-Barro PC, Kassi RR, Evi JB, Ewussi L, Kone M (2007). Presumptive clinical diagnosis of malaria: actual part of the disease. Médecine d'Afrique Noire 5403:139-44. |
|
|
Ministry of Solidarity and Health (2016). Prescription under international nonproprietary name (INN). |
|
|
Neuner-Jehle S (2016). Polypharmacy: a new epidemic. Revue médicale Suisse 12:942-947. |
|
|
National Malaria Control Program (NMCP) (2016). National guidelines for the management of malaria Ministry of Public Health, Democratic Republic of Congo. |
|
|
National Malaria Control Program (NMCP) (2017) Rapport d'activités 2016. |
|
|
National Malaria Control Program Senegal (NMCPsn) (2018). Practical guide to the fight against malaria in the compagny. |
|
|
Nsuadi-Manga F, Kabwayi-Mulema P, Juakali-SKV JJ (2020). Analysis of medical prescriptions for antimalarials at the general referral hospital of Makiso-Kisangani. Kisangani Médical 10(2):432-435. |
|
|
Nzolo D, Mulongo R (2013). Evaluation of drug use in six pilot hospitals where CPTs are operational in the Democratic Republic of the Congo. United States Agency for International Development Report by the Systems for Improved Access to Pharmaceuticals and Services Program (SIAPS). |
|
|
Pastor institute. Malaria (2019). |
|
|
President's Malaria Initiative (PMI) (2019). Democratic Republic of the Congo Abbreviated Malaria Operational Plan FY 2019 |
|
|
Severe Malaria Observatory (SMO) (2019). Assessment of the management of severe malaria cases in the DRC. Preliminary study report, 2019. |
|
|
Soumana A, Kamaye M, Issofou B, Dima H, Daouda B, N'Diaye O, Sall G (2016). Prescription of Antimalarial Drugs in the Pediatric Ward of the National Hospital of Lamordé in Niamey. Bulletin de la Société de pathologie exotique 109(5):353-357. |
|
|
Tené MY, Tapsoba SP, Issiaka S, Tinga RG (2015). Evaluation of application of national guidelines for the management of malaria in Bobo-Dioulasso university hospital. Santé Publique 2(2)7:265-273. |
|
|
Tsakala TM, Tona GL, Mesia GK, Mboma JC, Vangu JM, Voso SM., Kanja GL, Kodondi FKK, Mabela M, Walo R (2005). Assessment of prescriptions in the treatment of malaria and gastroenteritis in hospitals: Case of Bondeko and St Joseph hospitals in Kinshasa (Democratic Republic of the Congo). Cahiers d'études et de recherches francophones/Santé 15(2):119-124. |
|
|
World Health Organization (WHO) (2013). A generic name for active pharmaceutical substances around the world. |
|
|
World Health Organization (WHO) (2015). Malaria. World Malaria Report 2015. WHO reference number: WHO/HTM/GMP.2016.2 (summary). |
|
|
World Health Organization (WHO) (2018a). Malaria. Malaria treatment - an overview. |
|
|
World Health Organization (WHO) (2018b). Democratic Republic of Congo. Cooperation Strategy. An overview. |
|
|
World Health Organization (WHO) (2019). World Malaria Report 2019. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


