Full Length Research Paper

ABSTRACT
Historically Artemisia herba alba (AHA) is widely used in traditional Moroccan medicine. Few studies have been carried out to confirm its traditional use, in particularly immunological studies and to the authors’ knowledge; no study has treated the in vivo immunomodulatory effect of AHA aqueous extracts. This work was established to assess the immunological effects of AHA, including the humoral and cellular immunity effects in vivo. The immunomodulatory effect was assessed by measuring the titer of specific antibodies by the agglutination technique after immunization of Wistar rats with sheep red blood cells, while the pro-inflammatory effect was performed using a carrageenan-induced rat paw edema model. Administered AHA’s aqueous extract (AE) appears to have significantly (p < 0.01) stimulated the production of anti-SRBC antibodies with a dose-dependent effect compared to the control. These results were confirmed by a significant increase in the levels of white blood cells in particular neutrophils, lymphocytes, monocytes and eosinophils (p<0.05) for the doses 0.5 and 1 g/ml/bw. For the same doses of the extract, a proinflammatory effect was observed by the size of edema and the presence of very dense inflammatory infiltrate made up of lymphocytes, plasma cells and polymorphonuclear neutrophils. The AHA’s AE have shown an important immunomodulatory and pro-inflammatory activities in vivo by enhancing the production of antibodies and the inflammatory reaction.
Key words: Artemisia herba alba, Immunomodulatory effect, In vivo, pro-inflammatory effect, antibodies production, aqueous extract.
INTRODUCTION
Artemisia herba-alba (AHA) or Wormwood, known in Morocco as "Cheih", is a highly aromatic medicinal plant characteristic of the steppes and mountain ranges of the Moroccan high Atlas. It is well known in the world especially in Morocco in herbal medicine to treat various diseases.
AHA has antimicrobial activity well known in Jordanian folk medicine (Aburjai et al., 2001; Darwish and Aburjai, 2010) and herbal tea prepared from AHA has been used as an antibacterial agent in Algerian folk medicine (Laid et al., 2008). It also showed anti-leishmanian activity against L. tropica and L. major promastigotes (Hatimi et al., 2001).
AHA is used as an anti-diabetic (Kamal et al., 2007; Ashraf et al., 2010); indeed it is a very popular remedy for the treatment of diabetes mellitus, and many researchers, in particular, in Morocco have studied its hypoglycemic activity (Jouad et al., 2001; Eddouks et al., 2002). In addition to its hypoglycemic activity, Al-Waili has reported that the aqueous extract of AHA has a role in reducing high blood pressure, and also has anti-arrhythmic and anxiolytic actions (Al-waili, 1986, 1988). On the other hand, Skiker has shown that the aqueous extract of AHA induces a dose-dependent vasorelaxant action in aortic preparations isolated in rats (Skiker et al., 2010).
In Jordan, AHA is widely used in traditional medicine to relieve stomach and intestinal pain, cough, fever and in the treatment of inflammation and eye disease (Abu-Irmaileh and Afifi, 2003). In Tunisia, AHA is widely used in traditional medicine to treat several diseases such as diabetes, hypertension, neuralgia, and to relieve bronchitis and diarrhea (Marrif et al., 1995; Said et al., 2002; Tahraoui et al., 2007).
In Morocco, infusions of AHA have also been used as analgesic, antibacterial, and hemostatic agents. AHA’s essential oil has been used as a disinfectant, anthelmintic, and antispasmodic agent (Aehh et al., 2010). The concocted of AHA have been used to treat menstrual disorders, fever (Abad et al., 2012) and in the treatment of nervous disorders (Alzweiri et al., 2011).
In this context, phytochemical studies of the composition of AHA in the different countries of origin and even in the different localities of the same country have shown great diversity and the presence of several chemo types (Belhattab et al., 2014; Zouari et al., 2010; Salido et al., 2004).
However and despite its great use in traditional phytotherapy, few studies have been carried out to confirm the traditional use of AHA, in particular immunological studies and to our knowledge, no study has treated the in vivo Immunomodulatory effect of AHA’s AE and only a small number of studies have treated its anti-inflammatory effect in vivo. The authors work was established to assess the immunological effects of AHA AE in vivo, including the effect on humoral and cellular immunity responses.
MATERIALS AND METHODS
Plant material
AHA was harvested at the end of May, each year (for more than 60 years), in the Souss-Massa-Daraa region, particularly in the mountain ranges of the Grand Atlas of the province of Taroudant. After washing with distilled water the sample of AHA was dried for 21 days in the open air, protected from light to preserve the integrity of the molecules as much as possible, avoiding alterations and proliferation microorganisms. After drying the aerial part of the plant was collected, stored in hermetically sealed jars and placed in a place protected from light and heat (4ºC) to avoid any risk of contamination, degradation or denaturing until it is used. Just before the preparation of the extract, a quantity of the plant was grinded in an electric grinder to very fine powder for a high extraction yield.
Preparation of the aqueous extract:
The extraction of bioactive substances contained in the aerial part of AHA was carried out by maceration-infusion in boiled distilled water. 25 g of the powder obtained were added to 250ml of boiled distilled water and then left for 30 min for infusion with stirring. The mixture obtained was filtered on Wattman paper and the filtrate obtained represented a 10% stock solution (100 g/L) which was concentrated in a Rotavapor under vacuum (water bath set at 40-50ºC). After concentration, the extract was collected in a volume (selon la quantité de l’extrait) of distilled water and stored at in the dark at -20ºC.
Animals
Adult male rats of the Wistar Albino strain weighing between 220 and 270 g from breeding at the animal facility of the Ain Chock Faculty of Science at Hassan-II University. The rats were housed in cages and divided into several batches. Each group has free access to water and food. The rats were kept at room temperature 22-25°C. They were treated in accordance with the principle and directive set out in the manual on the care and use of test animals.
Evaluation of the humoral immune response by the hemagglutination test
The rats were divided into four groups as follows: Group 1 (3 rats): "Control Rats" received daily by gastric gavage 1 ml of distilled water for 10 days. Groups 2, 3 and 4 (3 rats each) received by gastric gavage daily 1 ml of the aqueous extract of AHA at the dose 250 mg/kg bw; 500 mg/kg bw and 1000 mg/kg bw, respectively for 10 days. On the fourth day of gastric gavage, the rats of the four batches received an intraperitoneal injection of 0.5 ml of sheep red blood cells (SRBC) at 1% in 0.9% NaCl and at the end of the 10 days were sacrificed to recover the blood.
The Titration of antibodies anti-SRBC was done on a 96-well microplate. A serial dilutions in 0.9% NaCl (1/2, 1/4; 1/8; 1/16 ;…) of the immune serum were made for a final volume of 25μl. A 25µl volume of the 1% SRBC solution was added to all the wells, followed by 2-h incubation at room temperature. At the end of the incubation, the hemagglutinating capacity of the anti-SRBC was read visually. Antibody titers were determined to be the reciprocal of the maximum dilution with a positive hemagglutination reaction.
Evaluation of the AHA AE effect on the induced inflammatory edema by Carrageenan
According to the method of Winter et al. (1962); a carrageenan solution (1% in 0.9% NaCl) at a dose of 0.2 ml / rat paw was injected. The carrageenan was injected into the fascia of the right leg plank, and into the fascia of the left leg (control) the same volume of 0.1 ml of physiological water was injected. 30 min before the injection of the carrageenan, the different batches of rats received the different treatments orally. The measurements of the volumes of the edema of each paw were carried out before the induction of the edema and after the injection of the carrageenan at T=0 min (time of injection), T = 30 min, T = 60 min, T = 120 min, and T = 180 min. The legs were weighed after sacrificing the animals by cerebral dislocation and cutting the legs at the level of the taxo-articulation.
The rats were divided into five groups of 3 rats as follows: Group 1: Control group; injection of 0.5 ml of NaCl. Group 2; injection of 0.5 ml of 1% carrageenan without any treatment, groups 3: injection of 1% carrageenan preceded by treatment with Diclofenac (100 mg/kg), groups 4 and 5 injection of 1% carrageenan preceded by treatment with aqueous extract of AHA at a dose of 500 mg/kg bw or 1g/kg bw, respectively.
The increase in paw edema (AUG) was calculated using the following equation:
AUG = Size of edema (cm) of swollen leg (Right) - Size of edema (cm) of healthy leg (Left)
RESULTS
Evaluation of the humoral immune response by the hemagglutination test
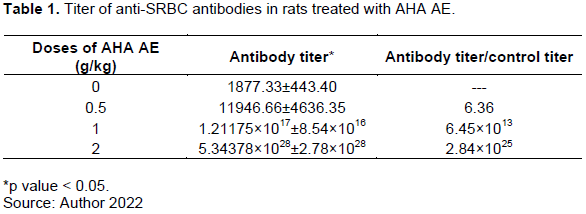
Compared to control, the titer of anti-SRBC antibody in rats treated with AHA extract was significantly higher (p<0.05). This titer was proportional to the injected dose; it went from 1/2048 to 1/524248, to 1/8388608, then to 1/8589934592 for the respective doses of 0.5 , 1, and 2 g/kg (Table 1). The administered extract appears to have stimulated the production of the anti-SRBC antibodies in dose-dependent manner.
Evaluation of the AHA AE effect on the induced inflammatory edema by Carrageenan
Assessment of the increase in the size of the paw edema (% AUG)
For the control group (AHA AE 0 g/kg), it was observed that the injection of carrageenan resulted in a significant increase (p < 0.05) in edema of the legs of the rats from the second hour of treatment (35.95 ± 13.46) to the third (46.12 ± 15.72), fourth (50.5 ± 13.49), and fifth hour (66.77 ± 9.25). Figure 1 shows variation of the percentage of increase in paw edema (% AUG) in the treated rats with aqueous extracts of Artemisia herba alba.

For the standard or positive control group, which received an anti-inflammatory treatment with Diclofenac at 0.1g/kg, the results showed a very significant decrease (p < 0.01) of the edema of the paws of the rats from the 1st hour following the induction of the edema by carrageenan (from 33.76 ± 6.2 to 23.08 ± 5.75), followed by another very significant (p<0.01) decrease after the 2nd (16.54 ± 5.77) and 3rd hour (16.58 ± 6.53) of induction of edema. After the 4th hour of the experiment, a very significant increase (p < 0.01) in the % AUG (AUGmentation in edema size) of the paws of the rats (23.2±5.05) was observed and which continues at the 5th hour (53.85±3.1) then wait for it to reach its maximum after 24 h of the experiment (65.3±5.15). At the end of the experiment (48 h) the % AUG was 19.67 ± 55.22.
However, in the group treated with AHA’s AE at dose of 0.5 g/kg of bw, a significant increase (p < 0.05) of the edema of paws of the rats from the second hour treatment (33.34 ± 7.43). This increase continues to be observed in the third (44.09 ± 6.09), the fourth (45.33 ± 6.6), the fifth hour (78.22 ± 14.41).
The results observed in the group treated with 1 g/kg/bw of the extract showed a significant (p < 0.01) increase in the % AUG of the paws of the rats at the second hour (48.88 ± 9.08), third (54.56 ± 6.63), fourth (61.85±4.44), fifth (71.52 ± 5.96), and also after 24 h (80.32 ± 6.37) of the treatment. For the 2 g/kg/bw a significant increase (p < 0.05) in % AUG was observed after fourth hour of treatment (49.51 ± 14.96) and which progressed and reached its maximum at the fifth hour (67.6 ± 11.95). The pro-inflammatory effect observed with induction of the edema by carrageenan was confirmed with significantly higher level of white blood cells (p > 0.05) in the rats treated with AHA AE at the doses of 0.5 g/kg and 1 g/kg/bw compared to the negative and positive control. Whereas this level is slightly lower in the group of rats treated with AHA AE at 2 g/kg bw compared to the two control groups (Figure 2A).
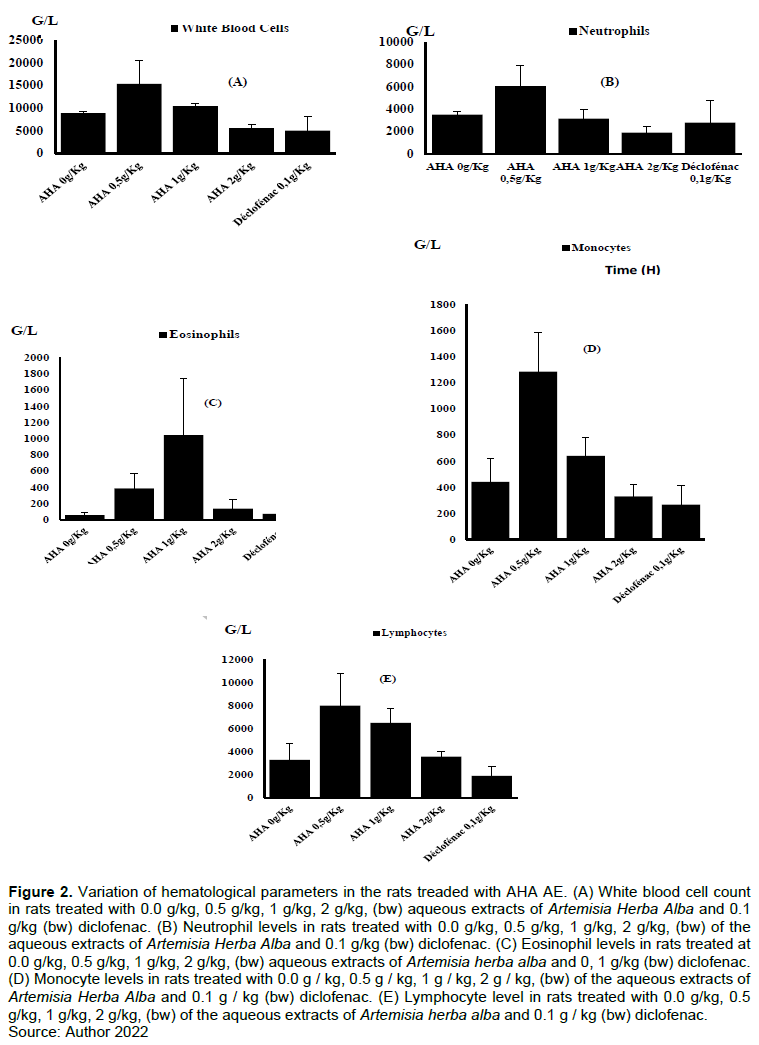
Number of neutrophils (Figure 2B), of eosinophils (Figure 2C), monocytes (Figure 2D), and of the lymphocytes (Figure 2E) was significantly higher (p > 0.05) in the group the rats treated with AHA AE at 0.5 and 1 g/kg bw than those treated at 2 g/kg bw compared to the negative and positive control.
The histological study confirmed a pro-inflammatory effect of AHA AE. In the negative control group, a very edematous and congestive fibrous tissue with a polymorphic inflammatory infiltrate and some polymorphic neutrophils of lymphocytes and plasma cells was observed (Figure 3A). For positive control group (Diclofenac 0.1 g/kg) an inflammatory infiltrate of low intensity was observed with fibro-fatty tissue and a striated muscle tissue dissociated by fibrosis as well as rare lymphocytes (Figure 3B).
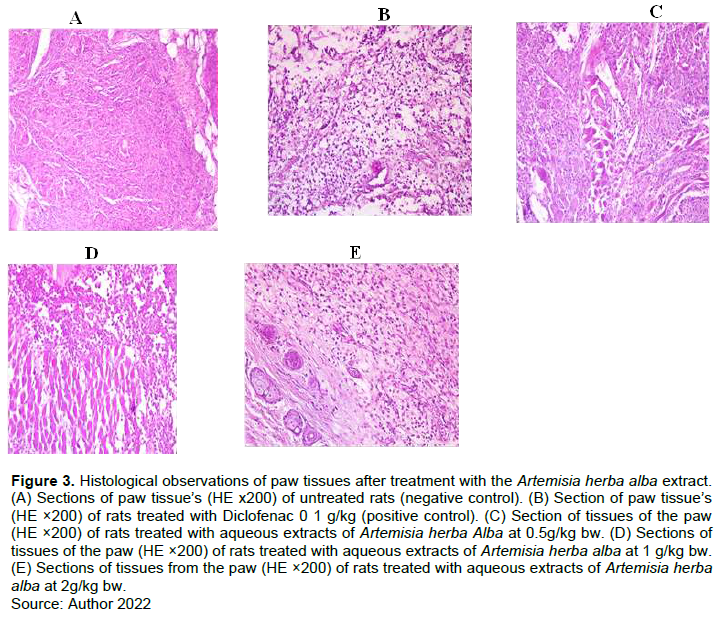
In the Group treated with AHA AE at 0.5 g/kg bw a very intense inflammatory polymorphic pseudo-follicular infiltrate was observed (Figure 3C).
Tissues of paws of rats from the group treated with AE-AHA at 1 g/kg bw showed a fibro-fatty striated muscle tissue dissociated by intense diffuse inflammation made up of macrophage plasma cells lymphocytes with histiocytes sometimes centered with a necrotic suppurative focus (Figure 3D). Group treated with AHA AE at 2 g/kg/bw showed a fibro-fatty and striated muscle tissue dissociated by intense diffuse inflammation made up of lymphocytes plasma cells, histiocyte macrophages sometimes centered with necrot suppurative focus (Figure 3E).
DISCUSSION
Studies have revealed the presence of several molecules known for their immunostimulatory effects, such as tannins, triterpenes, coumarins and flavonoids as well as several other phenolic compounds (Saleh et al., 1987). Likewise, the use of immunomodulators has an important place in the current development of immunotherapy. Immunomodulatory agents of plant and animal origin trigger the body's immune reactivity against active agents by activating the non-specific immune system (Kulkarni et al., 2001). On the other hand, innate and adaptive immunity depends on the activity of white blood cells. Innate immunity largely depends on the activity of granulocytes and macrophages, while the adaptive immune response depends on lymphocytes, which provide long-term memory immunity (Raphael et al., 2000).
The results obtained in the present study showed that the daily administration of AHA’s AE at doses of 0.5, 1, and 2 g/kg for 10 days made it possible to increase in a very significant way (p < 0.01) the level of antibodies in healthy rats immunized by the SRBC compared to control rats. This reveals the important immunostimulating effect of AHA’S AE and this can be the result of the richness of this plant in immunoactive molecules as revealed by several other studies such as the immunomodulatory action of inulin which activates the complement and the immunostimulatory action of alkyl amides on innate immunity (Faivre, 2012; Wamine, 2012).
These results lead us to suggest that AHA's AE contains one or more immunostimulatory molecules, whose immunostimulating effect can be explained by better recognition of the antigen given by activated T lymphocytes, which then proliferate and release cytokines (Smith and Kroes 2000). Or by the activation of complement and the release of reactive oxygen or nitrogen species by activated phagocytes and pro-inflammatory cytokines (Smith and Kroes 2000). This immunostimulatory effect can also be attributed to efficient macrophage function or improved lymphokine synthesis. On the other hand the increase of the humoral response as evidence by the improvement of the reactivity of the anti-SRBC antibodies in vivo as a consequence of immunization indicates an improved response of the macrophages and the subsets of B lymphocytes involved in the synthesis of antibodies (Patwardhan et al., 1990).
Finally, this immunostimulating effect of AHA’S AE can be used to strengthen immunity against many microorganisms.
The injection of carrageenan causes the release of several chemical mediators responsible for the inflammatory process. Indeed, this inflammatory response is biphasic: the initial phase of which lasts about an hour is due to the release of histamine and serotonin, bradykinin is released during the second phase (1.5 - 3 h), and the biosynthesis of prostaglandins takes place beyond the third hour (Reanmongkol et al., 2009). After carrageenan induces an inflammatory edema; the results of the evolution of edema and the histological studies showed that the AHA AE extract increased the inflammatory reaction in a dose dependent manner during the 5-6 h until 24h after treatment compared to the non-treated groups.
These results can be explained in part by the presence of polyphenolic compounds such as tannins and flavonoids (Bruneton, 1999). On the other part by the activation of chemical mediators, that increases the permeability of local capillaries and cause exudate to escape from the bloodstream into the interstitial space. This exudate is the cause of localized edema, which in turn compresses nerve endings thus causing a sensation of pain (Devulder et al., 2002; Rousselet et al., 2005). Other studies seem to indicate that flavonoids have the ability to modulate the functioning of the immune system by inhibiting the activity of enzymes that may be responsible for inflammation, they can also modulate the adhesion of monocytes during inflammation by inhibiting the expression of inflammatory mediators (Gallego et al., 2007) other flavonoids are able to inhibit histamine (Kim et al., 2004) or even prevent the formation of prostaglandins which cause inflammation. Such effects have been described (Yin et al., 2008) and which are due to the presence of flavones. Numerous studies seem to indicate that flavonoids capable of modulating the functioning of the immune system (Da-Silva, 2004; Middleton et al., 2000) effects on B or T lymphocytes can be variable, for example flavones (apigenin, luteolin and 7, 3’, 4’hydroxyflavone) and the flavones (kaempferol, quercetin and myricetin) inhibit the proliferation of T lymphocytes while myricetin activates B lymphocytes (Mookerjee et al., 1986). On the other hand during the inflammation process, NO is produced from L-arginine by inducible NO synthase (iNOS), the rapid reaction between superoxide and NO induces the formation of peroxynitrite which is a toxic substance that contributes to tissue damage in inflammatory diseases (Szabo, 2003).
CONCLUSION
The results obtained in the study showed that the daily administration of aqueous extracts of AHA at doses between 0.5 to 2 g/kg for 10 days made it possible to significantly increase the level of antibodies in healthy rats immunized with SRBC compared to healthy control rats. This reveals the important immunestimulating effect of these aqueous extracts of AHA and this can only be the result of the richness of this plant in immuno-active molecules as described by several other works. This increase in the level of antibodies as a function of the concentration of the aqueous extracts of AHA administered proves the existence of a significant dose-effect ratio on the humoral immune response.
On the other hand, the results of the test of the induced inflammatory state revealed that the aqueous extracts of AHA had a significant pro-inflammatory effect for the dose of 0.5 and 1 g/kg/bw which lasted four hours, the higher the dose, the more the pro-inflammatory effect is delayed. The EA of AHA would act more on the humoral immune response by increasing the rate of antibody production whereas for the dose of 1 g/kg/p.c.
The important immunomodulatory and pro-inflammatory activity of the AHA AE could be explained by this richness in flavonoids . It will be interesting to determine the mechanisms by which these active ingredients present in these extracts of AHA would strengthen the immune system and increase the humoral and cellular responses.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abad MJ, Bedoya LM, Apaza L, Bermejo P (2012). The Artemisia L. genus: a review of bioactive essential oils. Molecules 17(3):2542-66. |
|
|
Aburjai T, Darwish RM, Al-Khalil S, Mahafzah A, Al-Abbad A (2001). Screening of antibiotic resistant inhibitors from local plant materials against two different strains of Pseudomonas aeruginosa. Journal of Ethnopharmacology 76(1):39-44.. |
|
|
Abu-Irmaileh BE, Afifi FU (2003). Herbal medicine in Jordan with special emphasis on commonly used herbs. Journal of Ethnopharmacology 89(2-3):193-197. |
|
|
Aehh M, El-Sayed MA, Hegazy ME, Helaly SE, Esmail AM, Mohamed NS (2010). Chemical constituents and biological activities of Artemisia herba alba. Records of Natural Products 4(1):1-25. |
|
|
Al-waili NS (1986). Treatment of diabetes mellitus by Artemisia herba-alba extract: preliminary study. Clinical and Experimental Pharmacology and Physiology 13(7):569-573.. |
|
|
Al-Waili NS (1988). Artemisia herba-alba and diabetes mellitus. Clinical and Experimental Pharmacology and Physiology 15(6):497. |
|
|
Alzweiri M, Sarhan AA, Mansi K, Hudaib M, Abuijai T (2011). Ethnopharmacological survey of medicinal herbs in Jordan, the Northern Badia region. Journal of Ethnopharmacology 137(1):27-35.. |
|
|
Ashraf M, Hayat MQ, Jabeen S, Shaheen N, Khan MA, Yasmin G (2010). Artemisia L. species recognized by the local community of northern areas of Pakistan as folk therapeutic plants. Journal of Medicinal Plant Research 4(2):112-9. |
|
|
Belhattab R, Amor L, Barroso JG, Pedro LG, Figueiredo AC (2014). Essential oil from Artemisia herba-alba Asso grown wild in Algeria: Variability assessment and comparison with an updated literature survey. Arabian Journal of Chemical 7 (3):243-251. |
|
|
Bruneton J (1999). Pharmacognosie, phytochimie, plantes médicinales. 3ème ed. Ed. Tec et Doc, 1120 p. |
|
|
Da-Silva JA (2004). Mining the essential oils of the Anthemideae. African Journal of Biotechnology December 3(12):706-720. |
|
|
Darwish RM, Aburjai, TA (2010). Effect of ethnomedicinal plants used in folklore medicine in Jordan as antibiotic resistant inhibitors on Escherichia coli. BMC Complementary and Alternative Medicine 10(1):1-8. |
|
|
Devulder B, Hatron PY, Hachula (2002) Medicine interne. Masson paris. |
|
|
Eddouks M, Maghrani M, Lemhadri A, Ouahidi M.L, Jouad H (2002). Ethnopharmacological survey of medicinal plants used for the treatment of diabetes mellitus, hypertension and cardiac diseases in the south-east region of Morocco (Tafilalet). Journal of Ethnopharmacology 82(2):97-103. |
|
|
Faivre C (2012). Les plantes immunomodulatrices. Wamine. (Communication personnelle). |
|
|
Gallego G, Mediavilla G, Crespo V, Collado I, Pilar S, Esteller A, Campos S, Tunon S, María J (2007). The anti-inflammatory flavones quercetin and kaempferol cause inhibition of inducible nitric oxide synthase, cyclooxygenase-2 and reactive C-protein, and down-regulation of the nuclear factor kappaB pathway in Chang Liver cells. European Journal of Pharmacology 557(2-3):221-229. |
|
|
Hatimi S, Boudouma M, Bichichi M, Chaib N, Idrissi NG (2001). In vitro evaluation of antileishmania activity of Artemisiaherba alba Asso. Bulletin de la Société Pathologique Exotique 94(1):29-31. |
|
|
Kamal M, Masalmeh A, Hamzah N (2007). The hypolipidemic effects of Artemisia sieberi (A. herba-alba) in alloxan induced diabetic rats. International Journal of Pharmacology 3(6):487-91. |
|
|
Kim TH, Ito H, Hatano T, Taniguchi S, Khennouf S, Yoshida T (2004). Chemical constituents of Artemisia herba-alba Asso. Natural medicines 58(4):165. |
|
|
Jouad H, Haloui M, Rhiouani H, El Hilaly J, Eddouks M (2001). Ethnobotanical survey of medicinal plants used for the treatment of diabetes, cardiac and renal diseases in the North centre region of Morocco (Fez-Boulemane). Journal of Ethnopharmacology 77(2-3):175-182. PMID: 11535361. |
|
|
Laid M, Hegazy MEF, Ahmed AA (2008). Sesquiterpene lactones from Algerian Artemisia herba-alba. Phytochemistry Letter 1(2):85-88.. |
|
|
Marrif HI, Ali BH, Hassan KM (1995). Some pharmacological studies on Artemisia herba-alba (Asso) in rabbits and mice. Journa of Ethnopharmacology 49(1):51-55. |
|
|
Middleton EJr, Kandaswami C, Theoharides TC (2000). The effects of plant flavonoids on mammalian cells: implication for inflammation, heart disease, and cancer. Pharmacological Reviews 52(4):673-751. |
|
|
Mookerjee BK, Lee TP, Logue GP, Lippes HA, Middleton E (1986). The effects of flavonoids on human lymphocyte proliferative responses. Progress in Clinical and Biological Research 213:511-520. |
|
|
Patwardhan B, Kalbag D, Patki PS, Nagsampgi BA (1990). Search of immunomodulatory agents: A review, Indian Drugs 28(2):56-63. |
|
|
Reanmongkol W, Noppapan T, Subhadhirasakul S (2009). Antinociceptive, antipyretic, and anti-inflammatory activities of Putranjiva roxburghii Wall. leaf extract in experimental animals. Journal of natural medicines 63(3):290-296. |
|
|
Rousselet MC, Vignaud JM, Hofman P, Chatelet FP (2005). Inflammation et pathologie inflammatoire AFECAP pp. 1-57. |
|
|
Said O, Khalil K, Fulder S, Azaizeh H (2002). Ethnopharmacological survey of medicinal herbs in Israel, the Golan Heights and the West Bank region. Journal of Ethnopharmacology 83(3):251-265. |
|
|
Saleh NAM, El-Negoumy SI, Abou-Zaid MM (1987). Flavonoids of Artemisia judaica, A. monosperma and Artemisia herba-alba. Phytochemistry 26:3059-3064. |
|
|
Salido S, Valenzuela L.R, Altarejos J, Nogueras M, Sánchez A, Cano E (2004). Composition and infraspecific variability of Artemisia herba-alba from southern Spain. Biochemistry and Systemic Ecology 32(3):265-277. |
|
|
Skiker M, Mekhfi H, Mohamed A, Benyounes H, Lahlou S, Legssyer A, Bnouham M and Ziyyat A (2010). Identification of Artemisia campestris L. subsp. glutinosa (Besser) Batt. from Oriental Morocco based on its morphological traits and essential oil profile. Journal of Materials and Environmental Science 8(1):180-187. |
|
|
Smith HF, Kroes BH (2000). Immunomodulatory and antiinflamatory activity of Picrorhiza scrophulariflora, J Ethnopharmacol, 73:101-109. |
|
|
Szabo C (2003). Multiple pathways of peroxynitrite cytotoxicity. Toxicology letters, 140:105-112. |
|
|
Tahraoui A, El-Hilaly J, Israili ZH, Lyoussi B (2007). Ethnopharmacological survey of plants used in the traditional treatment of hypertension and diabetes in south-eastern Morocco (Errachidia province). Journal of Ethnopharmacology 110(1):105-117.. |
|
|
Wamine (2012). Monographies abrégées à l'usage des praticiens vétérinaires. (Communication personnelle). |
|
|
Yin Y, Gong FY, XinWu X, Sun Y, Li Y, Chen T, Xu Q (2008). Anti-inflammatory and immunosuppressive effect of flavones isolated from Artemisia vestita. Journal of Ethnopharmacology 120(1):1-6. |
|
|
Zouari S, Zouari N, Fakhfakh N, Bougatef A, Ayadi MA, Neffati M (2010). Chemical composition and biological activities of a new essential oil chemotype of Tunisian Artemisia herba alba Asso. Journal of Medicinal Plants Research 4(10): 871-880. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


