Full Length Research Paper

ABSTRACT
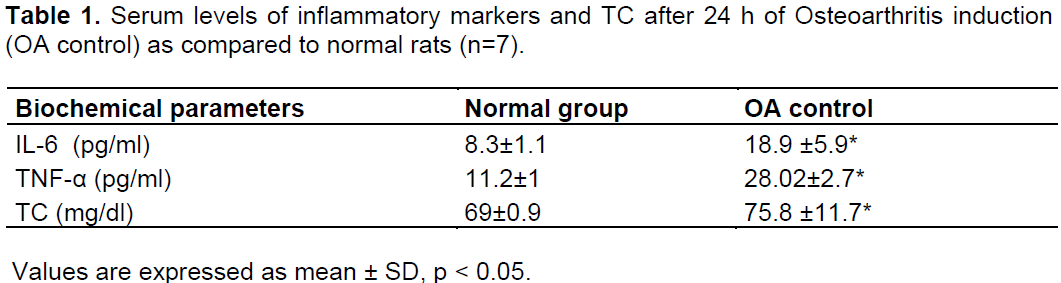
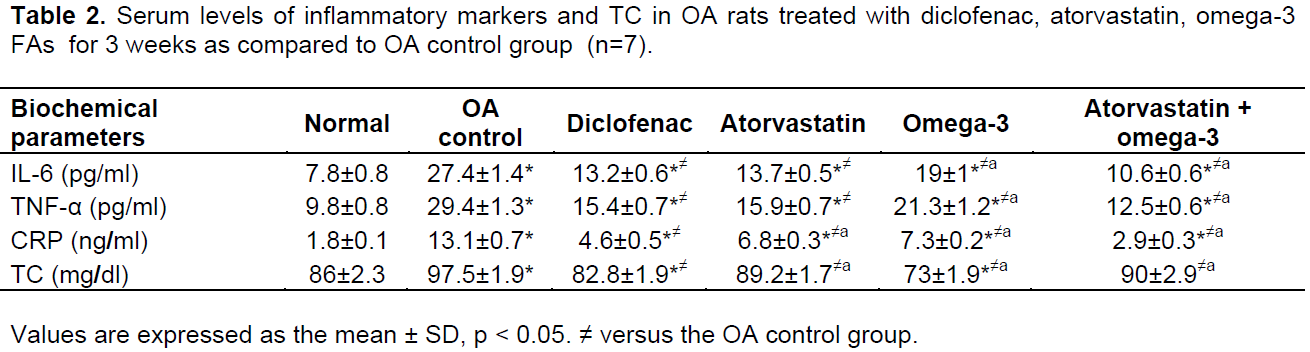
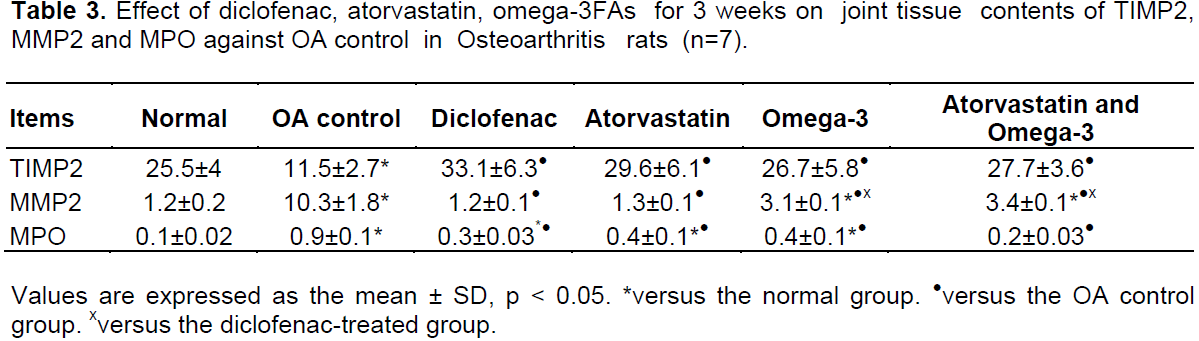
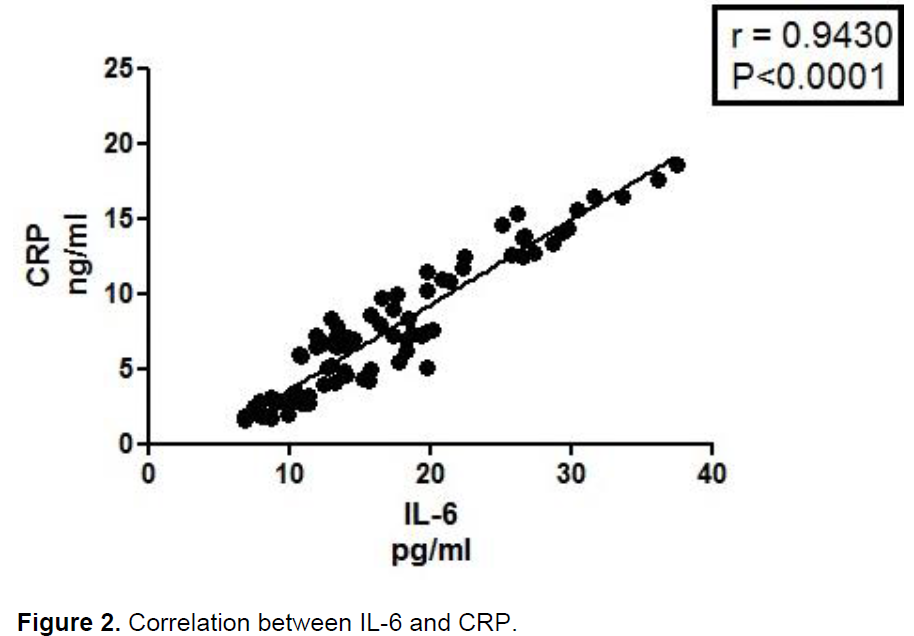
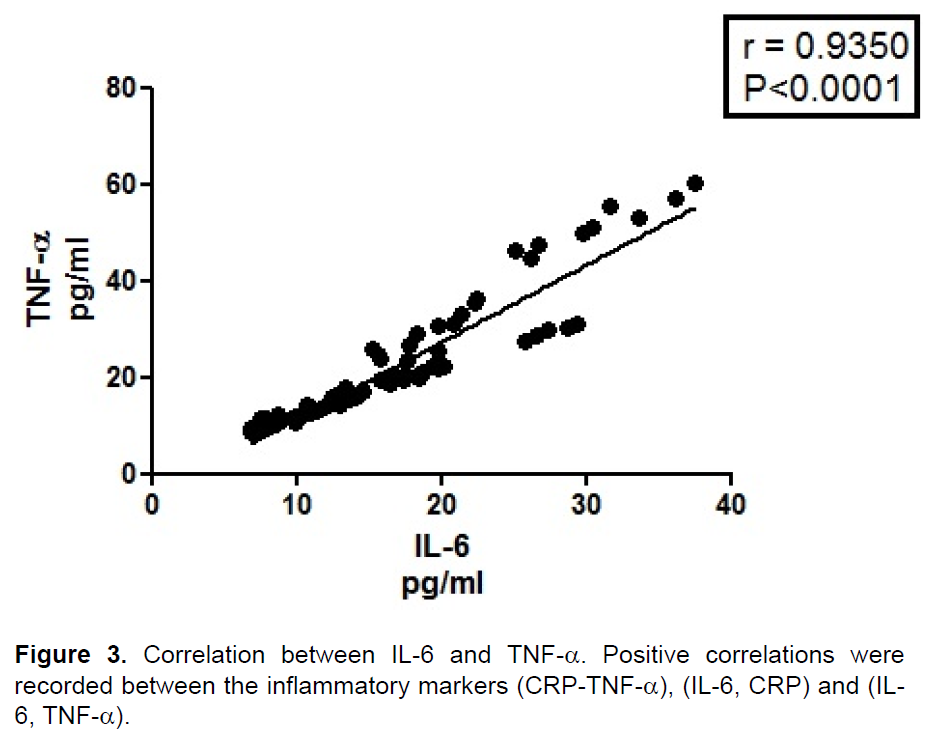
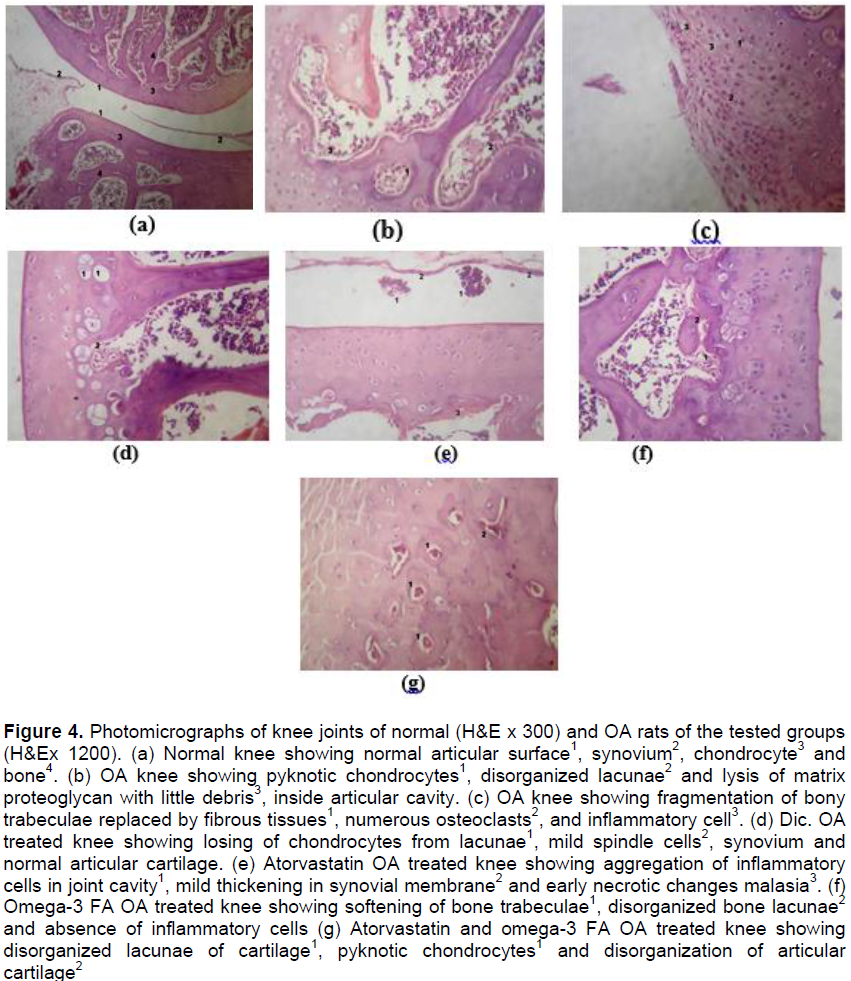
Antiinflammatory properties of statins and omega-3 fatty acids are well known and documented before. Present work aimed mainly to demonstrate their effects on inflammatory pattern of osteoarthritis (OA) induced in rats. Osteoarthritis was induced by single intraarticular injection of monosodium iodoacetate (MIA) in the right knee joints in a dose level of 24.6 mg/kg body weight. Omega 3 fatty acids and atorvastatin were applied topically(cream form) in a dose levels 1 g/kg and 10 mg/kg body weight respectively either individually or in combination versus diclofenac sodium in a dose level 5 mg/kg body weight for comparison. The treatment started after 24 h of OA induction, daily for 3 weeks. Collective results indicated that the drugs under study significantly decreased serum interleukine-6 (IL-6), tumor necrosis factor-α (TNF-α), C-reactive protein (CRP) and total cholesterol (TC). Joint tissue contents showed significant decrease in myeloperoxidase (MPO), matrix metalloproteinase2 (MMP2) along with an increase in tissue inhibitor metalloproteinase2 (TIMP2). Combined form of atorvastatin and omega 3 fatty acids demonstrated marked effects than their individual use as compared to Diclofenac.
Key words: Osteoarthritis, monosodium iodoacetate, atorvastatin, omega-3 fatty acids, diclofenac.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
ACKNOWLEDGEMENTS
REFERENCES
|
Alam R, Ji JR, Kim MS, Kim NS (2011). Biomarkers for identifying the early phases of osteoarthritis secondary to medial patellar luxation in dogs. J. Vet. Sci. 12(3):273-280. |
|
|
Allian CC, Roon LS, Chan CS (1974). Enzymatic determination of total serum cholesterol. Clin. Chem. 20:470. |
|
|
Al-Saffar FJ, Ganabadi S, Yaakub H, Fakurazi S (2009). Collagenase & sodium iodoacetate-indeuced experimental osteoarthritis model in sprague Dawley rat. Asian J. Sci. Res. 2(4):167-179. |
|
|
Banerjee M, Tripathi LM, Srivastava VM, Puri A, Shukla R (2003). Modulation of inflammatory mediators by ibuprofen and curcumin treatment during chronic inflammation in rat. Immunopharmacol. Immunotoxicol. 25(2):213-224. |
|
|
Barrios-Rodiles MG, Tiraloche MG, Chadee K (1999). Lipopolysaccharide modulates cyclooxygenase-2 transcriptionally and posttranscriptionally in human macrophages independently from endogenous IL-1 beta and TNF-alpha. J. Immunol. 163:963-969. |
|
|
Barsante MM, Roffe E, Yokoro CM, Tafuri WL, Souza DG, Pinho V, Castro MS, Teixeira MM (2005). Antiinflammatory and analgesic effects of atorvastatin in a rat model of adjuvant-induced arthritis. Eur. J. Pharmacol. 516:282-289. |
|
|
Benito MJ, Veale DJ, Fitzgerald O, Vanden Berg WB, Bresnihan B (2005). Synovial tissue inflammation in early and late osteoarthritis. Ann. Rheum. Dis. 64:1263-1267. |
|
|
Burke A, Smyth E, Fitzgerald GA (2006). Analgesic antipyretic agents pharmacotherapy of goat. In: Brunton LL, Lazo JS, Parker KL, editors. Good man & Gilman's the Pharmacological Basis of Therapeutics, 11th edition New York, Ny: McGraw-Hill. pp. 673-715. |
|
|
Caughey GE, Mantzioris E, Gibson RA, Cleland LG, James MJ (1996). The effect on human tumor necrosis factor alpha and interleukin 1 beta production of diets enriched in n-3 fatty acids from vegetable oil or fish oil. Am. J. Clin. Nutr. 63:116-122. |
|
|
Chapkin RS, AKoh CC, Lewis RE (1992). Dietary fish oil modulation of in vivo peritoneal macrophage leukotriene production and phagocytosis. J. Nutr. Biochem. 3:599-604. |
|
|
Curtis CL, Rees SG, Little CB, Flannery CR, Hughes CE, Wilson C, Dent CM, Otterness IG, Harwood JL, Caterson B (2002). Pathologic indicators of degradation and inflammation in human osteoarthritic cartilage are abrogated by exposure to n-3 fatty acids. Arthritis Rheum. 46(6):1544-53. |
|
|
Dalcico R, de Menezes AM, Deocleciano OB, Oria RB, Vale ML, Ribeiro RA, Brito GA (2012). Protective mechanisms of simvastatin in experimental periodontal disease. J. Periodontol. 84(8):1145-1157. |
|
|
Dwyer JH, Allayee H, Dwyer KM, Fan J, Wu H, Mar R, Lusis AJ, Mehrabian M (2004). Arachidonate 5-lipoxygenase promoter genotype, dietary arachidonic acid, and atherosclerosis. N. Engl. J. Med. 350:29-37. |
|
|
Kris-Etherton PM, Harris WS, Appel LJ (2002). Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation. 106: 2747-2757. |
|
|
Farid R, Rezaieyazdi Z, Mirfeizi Z, Hatef MR, Mirheidari M, Mansouri H, Esmaelli H, Bentley G, Foo Y, Watson RR, Lu Y (2010). Oral intake of purple passion fruit peel extract reduces pain and stiffness and improves physical function in adult patients with knee osteoarthritis. Nutr. Res. 30:601-606. |
|
|
Gierman LM, Kuhnast S, Koudijs A, Pieterman EJ, Kloppenburg M, van Osch GJ, Stojanovic-Susulic V, Huizinag TW, Princen HM, Zuurmond AM (2014). Osteoarthritis development is induced by increased dietary cholesterol and can be inhibited by atorvastatin in APOE*3Leiden.CETP mice: A translational model for atherosclerosis. Ann. Rheum. Dis. 73(5):921-7. |
|
|
Goldring MB (2000). Osteoarthritis and cartilage: The role of cytokines. Curr. Rheumatol. Rep. 2:459-465. |
|
|
Goldring MB, Goldring SR (2007). Osteoarthritis. J. Cell Physiol. 213:626-634. |
|
|
Goldring SR, Goldring MB (2006). Clinical aspects, pathology and pathophysiology of osteoarthritis. J. Musculoskelet. Neuronal. Interact. 6(4):376-378. |
|
|
Grossin L, Cournil-Henrionnet C, Pinzano I, Gaborit N, Dumas D, Etienne S, Stoltz JF, Terlain B, Netter P, Mir LM, Gillet P (2006). Gene transfer with HSP 70 in rat chondrocytes confers cytoprotection in vitro and during experimental osteoarthritis. FASEB J. 20:65-75. |
|
|
Guzman RE, Evans MG, Bove S, Morenko B, Kilgore K (2003). Monoiodoacetate-induced histologic changes in subchondral bone and articular cartilage of rat femorotibial joints: An animal model of osteoarthritis. Toxicol. Pathol. 31:619-624. |
|
|
Hussein N, Ah-Sing E, Wilkinson P, Leach C, Griffin BA, Millward DJ (2005). Long-chain conversion of [13C]linoleic acid and alpha-linolenic acid in response to marked changes in their dietary intake in men. J. Lipid Res. 46:269-280. |
|
|
Joe B, Lokesh BR (1997). Prophylactic and therapeutic effects of n-3 polyunsaturated fatty acids, capsaicin, and curcumin on adjuvant-induced arthritis in rats. J. Nutr. Biochem. 8:397-407. |
|
|
Kwak BR, Mulhaupt F, March F (2003). Atherosclerosis: Anti-inflammatory and immunomodulatory activities of statins. Autoimmune. Rev. 2:332-338. |
|
|
Lapillonne A, Clarke SD, Heird WC (2004). Polyunsaturated fatty acids and gene expression. Curr. Opin. Clin. Nutr. Metab. Care 7:151-156. |
|
|
Lee HB, Alam MR, Seol JW, Kim NS (2008). Tartrate-resistant acid phosphatase, matrix metalloproteinase-2 and tissue inhibitor of metalloproteinase-2 in early stages of canine osteoarthritis. Vet. Med. (Praha). 53:214-220. |
|
|
Lees P (2003). Pharmacology of drugs used to treat osteoarthritis in veterinary practice. Inflammopharmacol. 11:385-399. |
|
|
Mahdy AM, Galley HF, Abdel Wahed MA, Korny KF, Sheta SA, Webster NR (2002). Differential modulation of interleukin-6 and interleukin-10 by diclofenac in patients undergoing major surgery. Br. J. Anaesth. 88(6):797-802. |
|
|
Maher BM, Dhonnchu TN, Burke JP, Soo A, Wood AE, Watson RW (2009). Statins alter neutorphil migration by modulating cellular Rho activity: A potential mechanism for statins-mediated pleotropic effects. J. Leukoc. Biol. 85:186-93. |
|
|
Martel-Pelletier J, Boileau C, Pelletier JP, ROughley PJ (2008). Cartialge in normal and osteoarthritis conditions. Best Pract. Res. Clin. Rheumatol. 22:351-84. |
|
|
McCarey DW, McInnes IB, Madhok R, Hampson R, Scherbakov O, Ford I, Capell HA, Sattar N (2004). Trial of atorvastatin in rheumatoid arthritis (TARA): Double-blind, randomized placebo-controlled trial. Lancet 363:2015-21. |
|
|
Mitchell JA, Warner TD (2006). COX isoforms in the cardiovcular system: Understanding the activities of non-steroidal anti-inflammatory drugs. Nat. Rev. Drug Discov. 5:75-86. |
|
|
Okouchi M, Okayama N, Omi H, Imaeda K, Shimizu M, Fukutomi T, Itoh M (2003). Cerivastatin ameliorates high insulin-enhanced neutrophil-endothelial cell adhesion and endothelial intercellular adhesion molecule 1 expression by inhibiting mitogen-activated protein kinase activation. J. Diabetes Complicat. 17:380-386. |
|
|
Pfaffl MW (2001). A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 29:e45. |
|
|
Pischon T, Hankinson SE, Hotamisligil GS, Rifai N, Willett WC, RImm EB (2003). Habitual dietary intake of n-3 and n-6 fatty acids in relation to inflammatory markers among US men and women. Circulation 108:155-160. |
|
|
Raatz SK, Redmon JB, Wimmergren N, Donadio JV, Bibus DM (2009). Enhanced absorption of omega-3 fatty acids from emulsified compared with eucapsulated fish oil. J. Am. Diet. Assoc. 109(6):1076-1081. |
|
|
Simopoulos AP (2002). Omega-3 fatty acids in inflammation and autoimmune diseases. J. Am. College Nutr. 2(6):495-505. |
|
|
Wahane VD, Kumar VL (2010). Atorvastatin ameliorates inflammatory hyperalgesia in rat model of moon-articular arthritis. Pharmacol. Res. 51:329-333. |
|
|
Xu J, Nakamura MT, Cho HP, Clarke SD (1999). Sterol regulatory element binding protein-1 expression is suppressed by dietary polyunsaturated fatty acids: A mechanism for the coordinate suppression of lipogenic genes by polyunsaturated fats. J. Biol. Chem. 274:23577-2583. |
|
|
Yang S, Hsieh Y, Lue K, Chu S, Chang I, Lu K (2011). Effects of non-steroidal anti-inflammatory drugs on the expression of urokinase plasminogen activator and inhibitor and gelatinases in the early osteoarthritic knee of humans. Clin. Biochem. 41:109-116. |
|
|
Youssef S, Stuve O, Patarroyo JC, Ruiz PJ, Radosevich JL, Hur EM, Bravo M, Mitchell DJ, Sobel RA, Steinman L, Zamvil SS (2002). The HMG-CoA reductase inhibitors, atorvastatin, promotes a Th2 bias and reverse paralysis in central nervous system autoimmune disease. Nature 420:78-84. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


