Full Length Research Paper

ABSTRACT
The COVID-19 disease has triggered the death of millions of people worldwide and has been the cause of 4,281 deaths in Bangladesh since 8th March 2020 till 31st August 2020. This cross-sectional study was aimed at discerning the pattern of COVID-19 among the people of this country the testing response, the recovery pattern of the patients and the effect of co-existing conditions on their recovery. An online questionnaire was made and distributed among 565 randomly selected patients for their responses and statistical analysis was performed on those responses. Each participant described multiple symptoms and the most frequently described symptoms were fever, cough and loss of smell (described by 446, 225 and 171 participants, respectively). The majority of the participants (47.16) received their test reports within 3 to 5 days whereas 27.01, 10.76 and 15.07% participants got their reports within 1-2 , 6-10 and in more than 10 days, respectively and their residence area did not affect this time interval in getting the report. Overall 90% recovery rate was found which was different in different age groups being lowest in the group of people aged 70 years or more. Recovery seemed to be influenced by educational level, but not influenced by gender, residence level or professional educational background. Co-morbidities increased the likelihood of getting the disease and some of them (diabetes, hypertension, kidney diseases, cancer and HIV) interfered with the normal recovery process. More extensive studies with larger sample sizes are needed to conclusively discern the COVID-19 disease pattern among Bangladeshi people.
Key words: COVID-19, cross-sectional study, sign and symptom, convalescent, co-morbidity, Bangladesh
INTRODUCTION
The COVID-19 disease (Coronavirus Disease 2019), first diagnosed in Wuhan, China in December 2019 (Hui et al., 2020), has been on the pathway towards the largest global pandemic (Spinelli and Pellino, 2020) the 21st century has ever witnessed causing over 25,085,685 confirmed cases and 843,927 deaths worldwide until 31st August 2020 (WHO, 2020). It is caused by SARS-CoV-2 (The Severe Acute Respiratory Syndrome Coronavirus 2), also familiar in the name of 2019-nCoV (2019 novel Coronavirus), which resides taxonomically in the subgenus Sarbecovirus, genus Betacoronavirus, family Coronaviridae, order Nidovirales and has a positive-strand RNA as well as an envelope, taking bats as likely hosts and reservoirs (Bonilla-Aldana et al., 2020; Millán-Oñate et al., 2020; Rodriguez-Morales et al., 2020). This virus is usually 0.06-0.14 µm in diameter and displays a crown-like appearance under an electron microscope with spike-like projections on the surface resulting in having the name ‘coronavirus’ (Latin ‘corona’ means crown) (Al-Kuraishy and Al-Gareeb, 2020; Singhal, 2020). This disease, with a mean incubation time of 6.5 days, attacks people of all ages being transmitted via cough- and sneeze-generated large droplets from both symptomatic and asymptomatic patients and the virus in these droplets on the surface can remain infectious for days but becomes non-infectious in the presence of regular disinfectants (Hoehl et al., 2020; Kampf et al., 2020; Lai et al., 2020; Rothe et al., 2020). Initial symptoms include fever, fatigue, cough, headache, difficulty breathing, diarrhea and opaque lung in computer tomography (CT) imaging and these have been reported to proceed towards acute kidney injury, acute cardiac injury or acute respiratory distress syndrome (ARDS) in some cases which ultimately turned deadly for the patients (Chen et al., 2020a; Huang et al., 2020; Jiang et al., 2020; Song et al., 2020; Wang et al., 2020). It was reported that the most likely group of people to get COVID-19 was male and adult (aged between 34-59 years) while children were less at risk and the most vulnerable people were adults aged over 60 years irrespective of gender. Co-morbidities, specially diabetes, cardiac problems and cerebrovascular conditions, were found to increase the likelihood of infection and fatality significantly (Bai et al., 2020; Chang et al., 2020; Li et al., 2020; Liu et al., 2020; Shen and Yang, 2020).
Bangladesh has been battling with this disease since 8th March 2020 when the first 3 cases were reported and since then COVID-19 has spread in almost all the districts resulting in a nationwide lockdown from the 17th March which has not yet been completely lifted (Hridoy et al., 2020b). As of 21st July 2020, the mean reproduction number of SARS-CoV-2 in Bangladesh is 1.32 (Hridoy et al., 2020a) and as of 31st August 2020, there have officially been 312,996 cases and 4,281 deaths due to COVID-19 in this country (Bangladesh Coronavirus- Worldometer, 2020). With the existing health policy and structures, battling COVID-19 has been a mammoth task for Bangladesh and people are still facing obstacles to ensure appropriate treatment for themselves (Khan et al., 2020; Shammi et al., 2020). In spite of there being only one testing facility for whole Bangladesh initially, the number had grown considerably since then, which was still considered inadequate as the number of tests to the population ratio was still low resulting in doubts regarding the real situation of the country (Cousins, 2020; Islam et al., 2020). Very few studies done on COVID-19 disease pattern and recovery status in this country (Masrur et al., 2020).This study was aimed to determine the COVID-19 disease pattern, testing response, recovery status and the effect of co-morbidities on recovery among Bangladeshi people.
METHODOLOGY
Study in site
The study was coordinated as an online-based survey, where patients were provided with the questionnaire forms to fill up. The survey lasted for about one month ranging from July 1 to July 28, 2020.
Study population and sampling
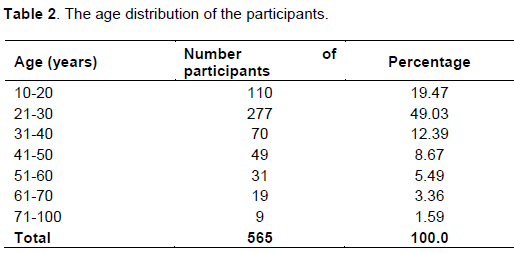
The study population consists of people who suffered from COVID-19 until July 28, 2020, and became corona negative or died due to COVID-19 within this period. The selection was random. The population was classified into the following age groups: 10-20 years; 21-30 years; 31-40 years; 41-50 years; 51-60 years; 61-70 years and 71-100 years. The study was conducted among people living in rural, suburban, and urban areas throughout Bangladesh. A total of 565 people participated in this study.
Study design
The study was a retrospective study. A questionnaire was made following established rules (Sakib et al., 2020) based on questions that lead to the study and research about the most susceptible population towards COVID-19 in Bangladesh based on age, location, gender, knowledge and their recovery status based on demographic factors. Moreover, the study was designed to know the COVID-19 pattern in Bangladesh.
Data collection and analysis
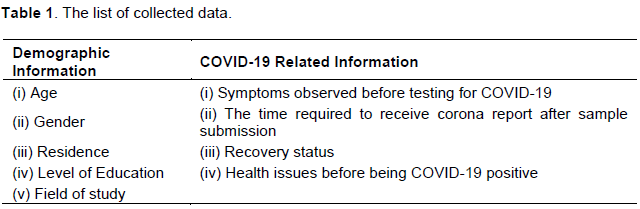
The data were collected via pharmacy students from different locations around the country who knew about corona patients and randomly sent them the questionnaire as an online form under their supervision. It consisted of questions that are enlisted in Table 1. Data were analyzed using Microsoft Office Excel 2013 and IBM SPSS Statistics 20 software.
Ethical issues
The patients’ informed consent was ensured. Their information was kept confidential and the names of the patients were not used in the questionnaire forms as a way to maintain the anonymity of the patients and dissolve any raising ethical questions.
RESULTS AND DISCUSSION
Participants’ information
A total of 565 people participated in the study. Among them, 294 (52.04) were male, 269 (47.61) were female and the rest (0.35%) were others. The age distribution of the participants is displayed in Table 2. 162 participants (28.67) lived in villages, 100 participants (17.70) lived in a semi-city level and the majority of them, 303 participants (53.63%), lived in a city. The education levels of the partakers are displayed in Table 3. Among the participants who responded to the question regarding their field of study (n=553), 143 people (25.86) were from medicine or related background (Pharmacy, medical science and so on), 181 people (32.73) were from a science background (but not medicine) and the rest (41.41%) were from a non-science background.

Symptoms
COVID-19 disease may be symptomatic or non-symptomatic. The symptoms include fever, sore throat, fatigue, cough, loss of smell and taste, headache, breathlessness and muscle pain, resulting in ARDS and multi-organ failure (Chen et al., 2020b; Gautier and Ravussin, 2020; Jin et al., 2020). In our study, most participants described multiple symptoms and fever, cough and loss of smell were found to be the most frequent symptoms, described by 446, 225 and 171 participants, respectively. Similar results were reported in other studies too (Yang et al., 2020).The findings are shown in Figure 1.

Delay between Corona testing and receiving the report
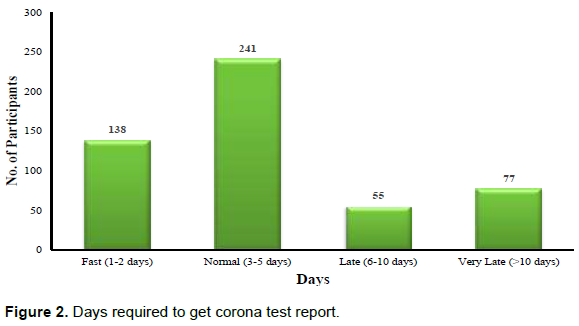
In Bangladesh, laboratory testing (RT-PCR- real-time reverse transcription polymerase chain reaction) is the only way to confirm if anyone has COVID-19 (Alam et al., 2020). There are many institutions that, at present, are performing the test, but due to the huge number of samples and low manpower, it takes a few days to get the report. From our study, it is evident that most people (47.16%) received the report within 3-5 days (Figure 2). It may be denoted as the normal time period required to get the report. 27.01% responders told us that they received the report within 1-2 days, which was fast compared to the normal time period. 10.76% of participants received the report within 6-10 days and 15.07% had to wait for more than 10 days to get the report. Two participants even told us that they had to wait for 30 days-which was much longer than the incubation period of SARS-CoV-2 and the test result was meaningless when they got result. Studies have attributed this delay to the deficiency of testing facilities and the huge population of this country (Anwar et al., 2020) which was also noticed in our study. Besides, the residence of the patients (city, semi-city or village) did not affect the time required to get the test report although this independence was not statistically significant (p= 0.06), according to our study.
Recovery
For this study, recovery was defined as being tested negative in RT-PCR testing. The Recovery rate from COVID-19 varies depending on the region and the age of the patients (Hamzah et al., 2020; Khafaie and Rahim, 2020). One study reported that the rate is 96.6% which is more than that of SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome) (De Wit et al., 2016; Sohrabi et al., 2020). In our study, a 90% recovery rate was seen overall. 28% of participants had been tested negative yet had symptoms of COVID-19 and the rest were corona-negative and symptom-free. The findings are shown in Figure 3. The recovery rate was found different in different age groups as other published works and the lowest of them was seen in people over 70 years of age (33.33%) (Liu et al., 2020; Onder et al., 2020). It is shown in Figure 4.


We attempted to identify whether some parameters influenced the recovery status. We found that gender, residence level (city, semi-city or village) or educational background (medicine-related, science or non-science) were not influencing factors for recovery, but those results were not statistically significant (p values of 0.44, 0.25 and 0.25, respectively). Most studies reported that men were at greater risk than women (de Groot and Bontrop, 2020; J.-M. Jin et al., 2020; Porcheddu et al., 2020), but we found no difference, which might have happened because of the small sample size. However, the patients’ age and educational level influenced their recovery and these results were statistically significant (p < 0.001 and p = 0.02, respectively). Younger patients were found to be more likely to recover from COVID-19 than older ones and it was in line with other studies (Promislow, 2020; Zhang et al., 2020). Again, the higher the educational level the patients were in, the more likely they were to recover from this disease.
Co-existing conditions
Previous studies found out that people with co-existing conditions were more likely to get COVID-19 (Guan et al., 2020). Our study found that 72.92% of the people suffering from COVID-19 were also suffering from other co-existing conditions, including asthma, hepatitis, hypertension etc. It is shown in Figure 5.

These co-morbidities were a huge and statistically significant influencing factor for the recovery of the patients (p = 0.008) as other studies reported (Kang, 2020; Guan et al., 2020). Also, they attempted to distinguish which co-existing conditions influenced the recovery individually and the result is displayed in Table 4. Diabetes, hypertension, kidney disease, cancer and HIV were found to lower the likelihood of recovery in a statistically significant manner, like other studies reported (Guan et al., 2020; Pal and Bhadada, 2020; Schiffrin et al., 2020), whereas asthma, hepatitis and tuberculosis showed no statistically significant interference in this regard.

CONCLUSION
COVID-19 is still ravaging Bangladesh and more and more people are dying every day. The study wanted to determine the pattern of COVID-19 disease conditions in this country’s people. This disease was not confined to urban areas; rural people were also falling victims to it. Its symptoms could easily be confused with those of common cold or respiratory problems and this fact had been making the diagnosis more difficult. RT-PCR testing was the only approved way for diagnosing and confirming COVID-19, but due to the deficiency of adequate testing facilities and the huge population, people were not receiving the results quickly. The recovery rate found in this study was lower than national and global statistics, which might happen because of the low sample size. Age and education were found to influence the recovery. Therefore, older people should be more careful regarding this disease. Co-morbidities played a vital role in the acquiring and worsening of this disease and among them, diabetes, hypertension and kidney diseases were found to be more influencing. It is expected that this study would help the physicians and the regulatory bodies planning and implementing necessary steps to remove this disease completely from Bangladesh. However, it should be mentioned that this study was preliminary in nature and there might have been limitations regarding the sample size. Hence, more extensive studies should be conducted to get a conclusive idea about COVID-19 in Bangladesh.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Alam MS, Alam MZ, Nazir KNH, Bhuiyan MAB (2020). The emergence of novel coronavirus disease (COVID-19) in Bangladesh: Present status, challenges, and future management. Journal of Advanced Veterinary and Animal Research 7(2):198-208. |
|
|
Al-Kuraishy HM, Al-Gareeb AI (2020). From SARS-CoV to nCoV-2019: Ruction and argument. Archives of Clinical Infectious Diseases 15:e102624. |
|
|
Anwar S, Nasrullah M, Hosen MJ (2020). COVID-19 and Bangladesh: Challenges and How to Address Them. Frontiers in Public Health 8 p. |
|
|
Bai Y, Yao L, Wei T, Tian F, Jin D-Y, Chen L, Wang M (2020). Presumed asymptomatic carrier transmission of COVID-19. Jama 323(14):1406-1407. |
|
|
Bangladesh Coronavirus (2020). 312,996 cases and 4,281 deaths - Worldometer]. URL |
|
|
Bonilla-Aldana DK, Dhama K, Rodriguez-Morales AJ (2020). Revisiting the one health approach in the context of COVID-19: a look into the ecology of this emerging disease. Advances in Animal and Veterinary Sciences 8(3):234-237. |
|
|
Chang D, Lin M, Wei L, Xie L, Zhu G, Cruz CSD, Sharma L (2020). Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. Jama 323(11):1092-1093. |
|
|
Chen L, Liu HG, Liu W, Liu J, Liu K, Shang J, Deng Y, Wei S (2020a). Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Zhonghua jie he he hu xi za zhi= Zhonghua jiehe he huxi zazhi= Chinese journal of tuberculosis and respiratory diseases 43:E005-E005. |
|
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y (2020b). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet 395(10223):507-513. |
|
|
Cousins S (2020). Bangladesh's COVID-19 testing criticised. The Lancet 396(10251):591. |
|
|
de Groot NG, Bontrop RE (2020). COVID-19 pandemic: is a gender-defined dosage effect responsible for the high mortality rate among males? Springer. |
|
|
De Wit E, Van Doremalen N, Falzarano D, Munster VJ (2016). SARS and MERS: recent insights into emerging coronaviruses. Nature Reviews Microbiology 14(8):523. |
|
|
Gautier J-F, Ravussin Y (2020). A New Symptom of COVID-19: Loss of Taste and Smell. Obesity 28(5):848-848. |
|
|
Guan W, Liang W, Zhao Y, Liang H, Chen Zi-sheng Li Y, Liu, Chen R, He J (2020). Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. European Respiratory Journal 55(5). |
|
|
Hamzah FB, Lau C, Nazri H, Ligot DV, Lee G, Tan CL (2020). CoronaTracker: worldwide COVID-19 outbreak data analysis and prediction. Bull World Health Organization 1:32. |
|
|
Hoehl S, Rabenau H, Berger A, Kortenbusch M, Cinatl J, Bojkova D, Behrens P, Böddinghaus B, Götsch U, Naujoks F (2020). Evidence of SARS-CoV-2 infection in returning travelers from Wuhan, China. New England Journal of Medicine 382(13):1278-1280. |
|
|
Hridoy AEE, Naim M, Alam E, Emon NU, Tipo IH, Tusher SMSH, Alam S, Islam MS (2020a). Estimation of Effective Reproduction Number for COVID-19 in Bangladesh and its districts. medRxiv. |
|
|
Hridoy AEE, Naim M, Emon NU, Tipo IH, Alam S, Al Mamun A, Islam MS (2020b). Forecasting COVID-19 Dynamics and Endpoint in Bangladesh: A Data-driven Approach. medRxiv. |
|
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet 395(10223):497-506. |
|
|
Hui DS, Azhar EI, Madani TA, Ntoumi F, Kock R, Dar O, Ippolito G, Mchugh TD, Memish ZA, Drosten C (2020). The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health-The latest 2019 novel coronavirus outbreak in Wuhan, China. International Journal of Infectious Diseases 91:264-266. |
|
|
Islam MS, Ira JI, Kabir KA, Kamrujjaman M (2020). COVID-19 Epidemic Compartments Model and Bangladesh. |
|
|
Jiang F, Deng L, Zhang L, Cai Y, Cheung CW, Xia Z (2020). Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). Journal of General Internal Medicine 35(5):1545-1549. |
|
|
Jin JM, Bai P, He W, Wu F, Liu XF, Han DM, Liu S, Yang JK (2020). Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. medRxiv. |
|
|
Jin X, Lian JS, Hu JH, Gao J, Zheng L, Zhang YM, Hao SR, Yang Y (2020). Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 69:1002-1009. |
|
|
Kampf G, Todt D, Pfaender S, Steinmann E (2020). Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. Journal of Hospital Infection 104(3):246-251. |
|
|
Kang YJ (2020). Mortality Rate of Infection With COVID-19 in Korea From the Perspective of Underlying Disease. Disaster Medicine and Public Health Preparedness pp. 1-3. |
|
|
Khafaie MA, Rahim F (2020). Cross-Country Comparison of Case Fatality Rates of COVID-19/SARS-COV-2. Osong Public Health and Research Perspectives 11(2):74-80. |
|
|
Khan HR, Howlader T, Islam MM (2020). Battling the COVID-19 Pandemic: Is Bangladesh Prepared? medRxiv 2020.04.29.20084236. |
|
|
Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR (2020). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. International Journal Of Antimicrobial Agents 55(3):105924. |
|
|
Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, Ren R, Leung KS, Lau EH, Wong JY (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. England Journal of Medicine. |
|
|
Liu K, Chen Y, Lin R, Han K (2020). Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. Journal of Infection 80(6):e14-e18. |
|
|
Liu W, Zhang Q, Chen J, Xiang R, Song H, Shu S, Chen L, Liang L, Zhou J, You L (2020). Detection of Covid-19 in children in early January 2020 in Wuhan, China. England Journal of Medicine 382(14):1370-1371. |
|
|
Masrur A, Yu M, Luo W, Dewan A (2020). Space-time patterns, change, and propagation of COVID-19 risk relative to the intervention scenarios in Bangladesh. International Journal of Environmental Research and Public Health 17(16):5911. |
|
|
Millán-Oñate J, Rodriguez-Morales AJ, Camacho-Moreno G, Mendoza-Ramírez H, Rodríguez-Sabogal IA, Álvarez-Moreno C (2020). A new. emerging zoonotic virus of concern: the 2019 novel Coronavirus (SARS CoV-2). Infectious 24(3):187-192 |
|
|
Onder G, Rezza, G, Brusaferro S (2020). Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 323(18):1775-1776. |
|
|
Pal R, Bhadada SK (2020). COVID-19 and diabetes mellitus: An unholy interaction of two pandemics. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 14(4):513-517. |
|
|
Porcheddu R, Serra C, Kelvin D, Kelvin N, Rubino S (2020). Similarity in Case Fatality Rates (CFR) of COVID-19/SARS-COV-2 in Italy and China. The Journal of Infection in Developing Countries 14(02):125-128.. |
|
|
Promislow DEL (2020). A Geroscience Perspective on COVID-19 Mortality. The Journals of Gerontology: Series A 75(9):e30-e33. |
|
|
Rodriguez-Morales AJ, Bonilla-Aldana DK, Balbin-Ramon GJ, Rabaan AA, Sah R, Paniz-Mondolfi A, Pagliano P, Esposito S (2020). History is repeating itself: Probable zoonotic spillover as the cause of the 2019 novel Coronavirus Epidemic. Infez Med 28(1):3-5. |
|
|
Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, Zimmer T, Thiel V, Janke C, Guggemos W (2020). Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. New England Journal of Medicine 382(10):970-971. |
|
|
Sakib N, Bhuiyan AI, Hossain S, Al Mamun F, Hosen I, Abdullah AH, Sarker MA, Mohiuddin MS, Rayhan I, Hossain M (2020). Psychometric validation of the Bangla Fear of COVID-19 Scale: Confirmatory factor analysis and Rasch analysis. International Journal of Mental Health and Addiction, pp. 1-12. |
|
|
Schiffrin EL, Flack JM, Ito S, Muntner P, Webb RC (2020). Hypertension and COVID-19. American Journal of Hypertension. 33:373-374. |
|
|
Shammi M, Bodrud-Doza M, Islam AR, Rahman MM (2020). Strategic assessment of COVID-19 pandemic in Bangladesh: comparative lockdown scenario analysis, public perception, and management for sustainability. Environment, Development and Sustainability 23(4):6148-6191. |
|
|
Shen KL, Yang YH (2020). Diagnosis and treatment of 2019 novel coronavirus infection in children: a pressing issue. Springer. com/content/pdf/10.1007/s12519-020-00344-6. pdf. |
|
|
Singhal T (2020). A review of coronavirus disease-2019 (COVID-19). The Indian Journal of Pediatrics 87(4):281-286. |
|
|
Sohrabi C, Alsafi Z, O'Neill N, Khan M, Kerwan A, Al-Jabir A, Iosifidis C, Agha R (2020). World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). International Journal of Surgery 76:71-76. |
|
|
Song F, Shi N, Shan F, Zhang Z, Shen J, Lu H, Ling Y, Jiang Y, Shi Y (2020). Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 295(1):210-217. |
|
|
Spinelli A, Pellino G (2020). COVID?19 pandemic: perspectives on an unfolding crisis. British Journal of Surgery 107(7):785-787. |
|
|
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y (2020). Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. Jama 323(11):1061-1069.. |
|
|
WHO Coronavirus Disease (COVID-19) (2020). URL |
|
|
Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, Ji R, Wang H, Wang Y, Zhou Y (2020). Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. International Journal of Infectious Diseases 94:91-95. |
|
|
Zhang J, Wang X, Jia X, Li J, Hu K, Chen G, Wei J, Wang G, Dong W, (2020). Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clinical Microbiology and Infection 26(6):767-772. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


