Full Length Research Paper

ABSTRACT
This study aimed to characterize the profile of medication consumption by low risk pregnant women and to correlate it with sociodemographic characteristics of this population. A cross-sectional descriptive study was conducted in the Reference Center of Women's Health in the Brazilian municipality of Ribeirão Preto. This study included women which were at least in the 32nd week of the gestation period. Data related to sociodemographic characteristics of the pregnant women and to their pregnancy and medication consumption were collected from June, 2008 to November, 2008. A total of 699 pregnant women were included. About 20% of the pregnant women began prenatal care in the 12th week of gestation and 75.3% had at least six antenatal visits. The use of at least one drug during pregnancy was reported by 98% of the participants. The mean number of medications used was 4.35. According to the Food and Drug Administration (FDA) risk classification, 14.07% of the medication belonged to C category, 1.85% to D and 0.03% to X, and 38.30% were not identified or not classified by the FDA. When correlating the number of prenatal visits with the amount of medication used, it was verified that pregnant women who underwent less than six visits during pregnancy used a higher number of medications. Pregnant women have been exposed to a variety of medications and there is a need to improve the quality of care in order to prevent potential risks to the fetus, especially in relation to the use of medications.
Key words: Drug utilization, fetus, pregnant women, prenatal care.
INTRODUCTION
Proper use of medications during pregnancy is an essential part of prenatal care, since it can affect not only the health of the pregnant woman but also the developing fetus, which is exposed to a wide range of adverse effects (Daw et al., 2011; Mitchell et al., 2011). Before the disaster caused by the use of thalidomide in the late 1950s and early 1960s, placenta was considered a barrier capable of protecting the fetus from any pharmacological damage (Lenz, 1962; Martinez-Frias et al., 2012; Oliveira et al., 1999; Papaseita et al., 2013). However, currently it is known that most drugs, as well as various substances present in the environment have the ability to cross the placental barrier and reach the bloodstream of the fetus, exposing it to pharmacological and/or teratogenic effects (Berglund et al., 1984; Giaginis et al., 2012; Myren et al., 2007; Schantz, 1996; Swan, 2000; Tilson et al., 1998; West and Blake, 2005). Non-steroidal anti-inflammatory drugs (NSAIDs), for example, widely prescribed in pregnancy to treat fever, pain and inflammation may cause embryo-fetal and neonatal adverse effects. Exposure to NSAIDs in early pregnancy is associated with increased risks of miscarriage and malformations and after 30 weeks of gestation is related with an increased risk of premature closure of the fetal ductus arteriosus and oligohydraminios (Antonucci et al., 2012). Additionally, fetal and neonatal adverse effects in brain, kidney, lung skeleton, gastrointestinal tract and cardiovascular system have also been reported after the use of NSAIDs during prenatal (Antonucci et al., 2012; Boubred et al., 2006). Other drugs used by pregnant women during prenatal, like immunosuppressive drugs, are not associated with higher risk of congenital anomalies but can be associated with an increased incidence of prematurity, intrauterine growth retardation and low birth weight (Prévot et al., 2002).
According to literature, a recent systematic review of drug utilization studies showed a wide variation of drug use during pregnancy in developed countries, which was from 27 to 93% (Daw et al., 2011). The prevalence of medication use among pregnant women in Brazil varied from 80 to 94.6% (Brum et al., 2011; Fonseca et al., 2002; Geib et al., 2007). In some specific conditions, as in the cases of women that have acute or chronic comorbidities, therapeutic intervention becomes a crucial option (Lupattelli et al., 2013; Orbach et al., 2013; Torres and Moayedi, 2012). Therefore, it is essential to ensure the safety of both mother and fetus in these situations. However, pregnant women without comorbidities, that is, low risk pregnant women are also likely to use some medication. It is important to investigate the use of medication among this population since pregnancy may lead to some situations that require medication. In addition, the low risk pregnant women may lack some important information about the risk and benefits of the use of the medication during pregnancy.
In this context, drug utilization studies are important tools to identify the drugs used and which of them are the most commonly used during pregnancy and its effects on the pregnant woman and the fetus, mainly due to ethical impediments to conducting clinical trials with pregnant women (Baylis, 2010; Mitchell, 2000; Ward, 2001) and the lack of knowledge about the real impact of drugs on the fetus (McCarter-Spaulding, 2005). A study by the Food and Drug Administration (FDA) in the United States, for example, noted that 91.2% of the 486 drugs approved between 1980 and 2000 had indeterminate risk of teratogenicity (Lo, 2002).
Aim of the study
This study aimed to characterize the profile of medication consumption by pregnant women in the antenatal period and to correlate it with socio-demographic characteristics of this population.
Ethical approval
This study was approved by the Ethics Committee of School of Pharmaceutical Sciences of Ribeirão Preto, University of São Paulo CEP/FCFRP-USP, protocol no. 115.
METHODOLOGY
Study design and data collection
This descriptive study was conducted in the Brazilian city of Ribeirão Preto from the state of São Paulo. We collected information about medication used by pregnant women outpatients assisted by the Brazilian public health system called SUS in the Reference Center of Women's Health of Ribeirão Preto called MATER. This center is a reference for low-risk births and the only center that attends the population of Ribeirão Preto and 26 other cities covering an estimated population of 3,000,000.
From June, 2008 to November, 2008, pregnant women were invited to participate in the study when they come to MATER for their medical appointment. The inclusion criteria were pregnant women in routine antenatal care at MATER that were at least in 32nd gestational week and that have availability of time of an average of 20 min to answer the collection form. Exclusion criteria were women with pregnancy complications such as chronic comorbidities, infectious diseases, fetal malformation, twin pregnancy and risk of preterm delivery, as the target population of this study was low risk pregnant women. All data related to the exclusion criteria were retrieved from their medical records. On average, 2,800 women gave birth at the hospital each year and the studied population represented 25% of the pregnant attended by MATER in one year.
After acceptance, they were interviewed using a data collection form developed following the standards of the World Health Organization (WHO) as described by Lockerbie and Lutz (1986). Data collection form was previously standardized through a pilot study conducted with 53 pregnant women from MATER in order to verify their comprehension. The results obtained with these patients were excluded from the final analyses. Only one interviewer made all the interviews and his interference was none since the questions were objective. We collected sociodemographic data (age, ethnicity, educational level, marital status, employment situation, number of family members); clinical data (general state of health, number of medical appointments, number of pregnancies); and data about the pharmacotherapy used (name and number of medications being used at the moment of the interview and consumed since the beginning of pregnancy, both with and without medical prescription).
Medication was defined according to Oxford Dictionaries in this study as a drug or other form of medicine that is used to treat or prevent disease (Oxford Dictionaries, 2014). Therefore salts of iron, folic acid, vitamins and vaccines were also included in this definition. All consumed medications were classified according to FDA of the United States into one of the five categories A, B, C, D, and X according to potential fetal risk during pregnancy (Pangle, 2006). The over the counter (OTC) drugs were identified by Resolution nº 138/2003 (Brasil, 2003) and its updates according to National Health Surveillance Agency (ANVISA).
Data analysis
In this study, polytomous logistic regression (Hosmer et al., 2013) was used to determine the associations between the number of medications used by pregnant women as the dependent variable (three categories: zero, 1 to 4 and 5 or more) and a set of exposure variables, which were the sociodemographic and clinical data that were selected based on the literature (Baraka et al., 2014; Busuff and Omarusehe, 2011). The strength of the associations between each exposure variable with the number of medications was measured by odds ratios (OR) with 95% confidence intervals (95% CI). Univariate and multivariate regression models were used to estimate crude and adjusted OR measures, respectively. The model was adjusted for all variables used. The SAS software was used for all statistic procedures and the significance level was set to 0.05.
RESULTS
During the period of data collection, 952 pregnant women had their prenatal visits in MATER. However, 243 did not fulfill the inclusion criteria since they lacked availability of time to answer the collection form. Among the remaining 709 pregnant women that were eligible for this study, 10 declined to participate, being 699, the total number of participants in the study. All the 699 participants completed the entire form; therefore, the response rate was 73.42%. Table 1 presents the sociodemographic and clinical data of the participants. The age ranged from 13 to 48 years (mean 24.9 years) and the majority of them were between 20 and 39 (79.54%). Considering the ethnicity, most interviewees stated themselves as of mixed-race (49.36%). Most of the women (99.71%) can read and write and had more than one year of study. In relation to the occupation, 5.72% of the women were students and 47.35% performed remunerated activity. Regarding the marital status, 80.11% of the women were married or living with a partner. The number of children ranged from 0 to 7 (average of 1.6 children per woman). The majority (47.07%) had no children, and 43.8% were in their first pregnancy. As also shown in Table 1, most pregnancies (62.52%) were unplanned and 73.39% of the respondents did not use any contraceptive method. At the diagnosis of pregnancy, 86.98% of pregnant women were between the 1st and 12th week of gestation. In relation to the gestational age at the time prenatal care began, 66.81% of the women were between the 1st and 12th week of pregnancy and 33.19% were in the 12th week or above. Additionally, up to the time of the interview, 50.5% of women had experienced seven or more prenatal visits.
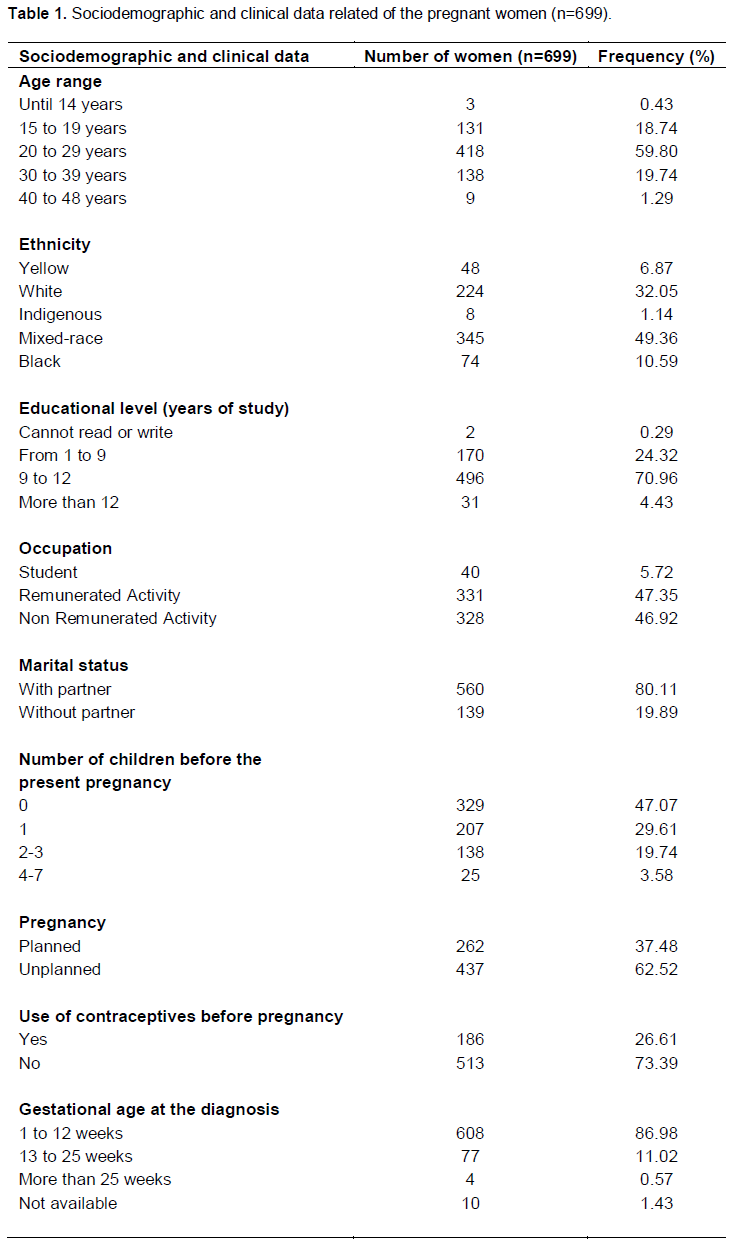
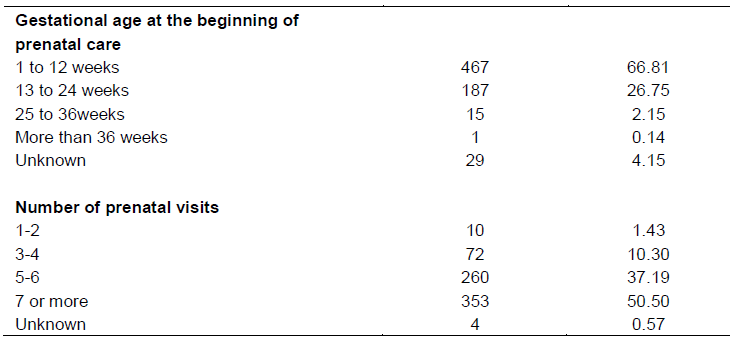
Table 2 shows the most common drugs used by pregnant women until the time of the interview. Each participant used from zero to 34 active moieties (average of 7) and 98.0% of them used at least one active ingredient. When iron salts, folic acid, vitamins and vaccines were excluded, 91.0% of the respondents continued to use at least one active moiety during pregnancy, however the average for pregnant women decreased to three, with a range of zero to 19. As shown in Table 3, 13.69% of the medications were used without prescription and the majority of them were classified as OTC medication. The medications were classified according to the risk classification of drugs during pregnancy of FDA (Pangle, 2006). As shown in Table 4, 14.07% of the drugs used belonged to C category. Medications not identified or classified in the FDA risk classification accounted for 38.3% of the medication used by this population.
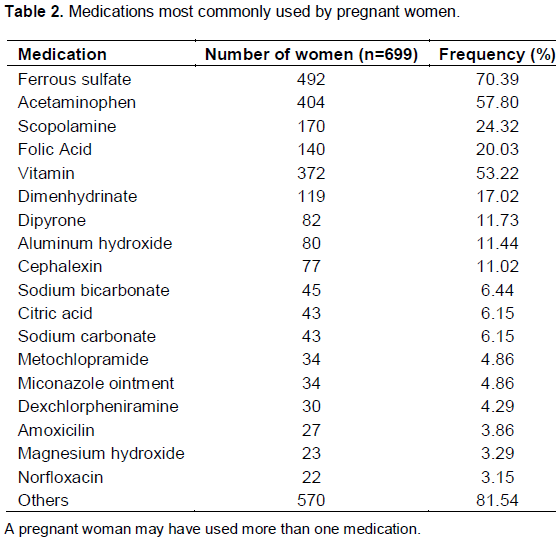
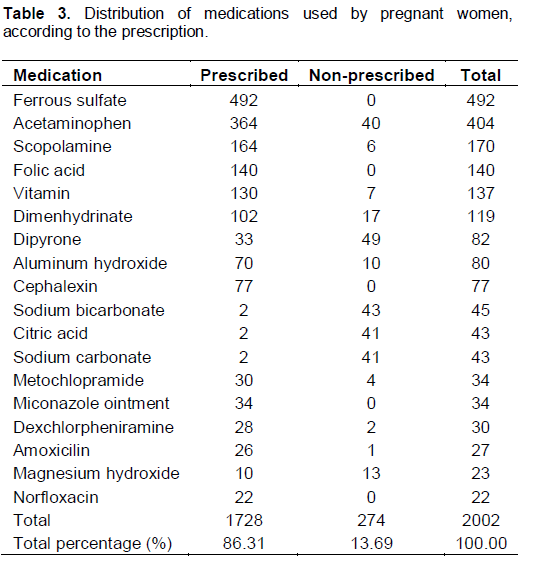
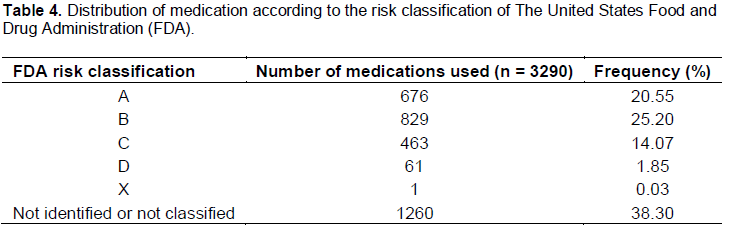
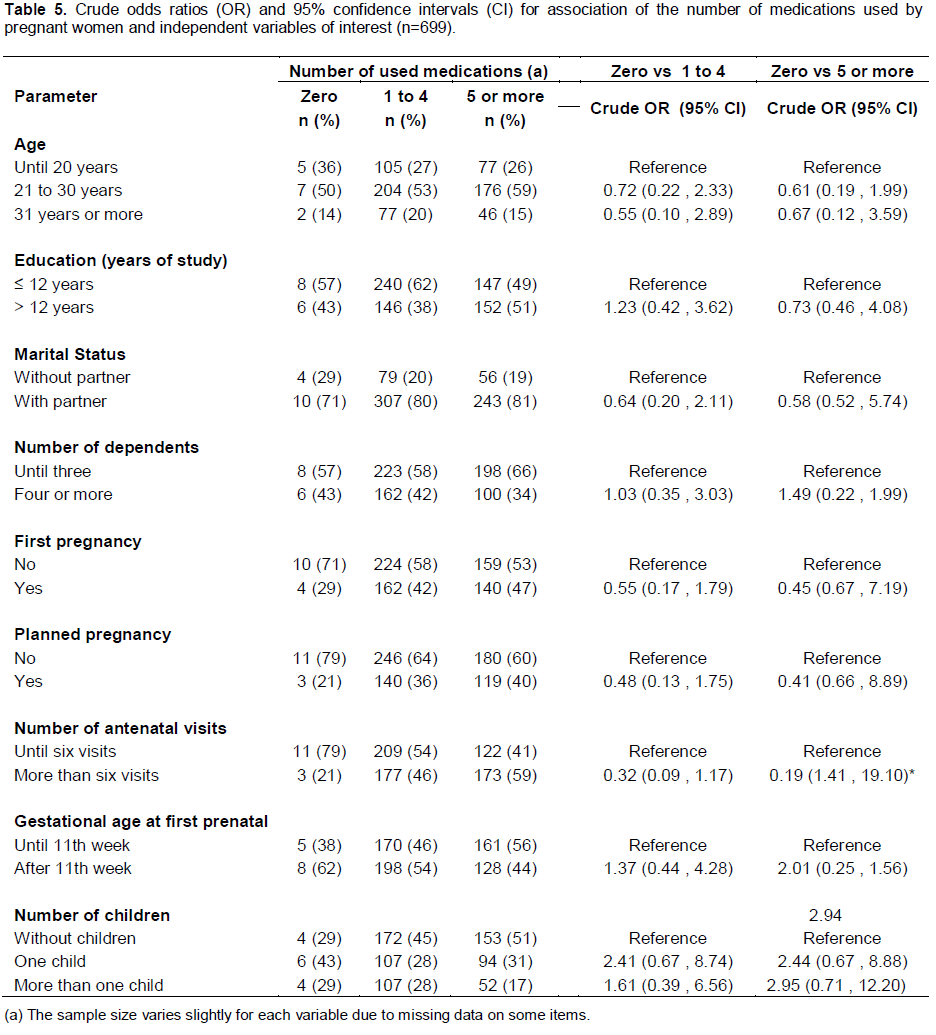
Table 5 shows crude odds ratios with their respective 95% CI for each of the exposure variables of interest. Confidence intervals not including the value of 1 indicate a significant difference toward the reference category (similar to p < 0.05). Thus, only the variable indicating the number of antenatal visits have association with the number of medications used by pregnant women (OR 0.19, when compared zero versus 5 or more medications). Table 6 shows that the number of antenatal visits is also the only variable in the set of exposures that was statistically significant according to a multivariate polytomous logistic regression analysis. This statistical model considered all the exposures described in the Table 5 as possible confounding factors. Thus, an adjusted OR of 0.15 suggests that a pregnant woman that reported more than six antenatal visits have a minor chance of using five or more medications when compared with woman that reports until six antenatal visits (Table 6).

DISCUSSION
Our study showed that 98.0% of the participants used at least one medication, being 91.0% when iron salts, folic acid, vitamins and vaccines were excluded. Over the last three decades, the use of medication during pregnancy increased by about 60% (Mitchell et al., 2011). Therefore, the identification of patterns of drug utilization among pregnant women is important as it provide helpful information to establish strategies to prevent the indiscriminate use of medications. We could observe with this study that the majority of the women (62.52%) reported they had unplanned pregnancy. Another Brazilian study showed a similar prevalence (66.7%) (Borges et al., 2011). This finding is important since women that have not planned pregnancy are more likely to use medications than those that did, since the women that planned their pregnancy are more aware of the harm some medications can cause to their fetus. The low prevalence of planned pregnancy may have also influenced on the low consumption of the antianemic folic acid (20.03%), which is recommended to all pregnant women. In addition, the periconceptional use of folic acid in preventing birth defects during pregnancy is also important important as observed in a randomized clinical trial (Czeizel and Dudás, 1992; McNulty et al., 2013; Olney and Mulinare, 2002; Smithells et al., 1980).
Ferrous sulphate use, another antianemic, was reported by 70.39% of the patients. Similarly, Lunet et al. (2008) and Domingues et al. (2012) observed that 81.9 and 90% of pregnant women used iron during pregnancy in studies performed in Portugal and Brazil, respectively. Additionally, an intercontinental corporative study showed that 80% of Brazilian women included in the study used ferrous sulphate and folic acid (Collaborative Group on Drug use in Pregnancy - CGDUP, 1992). However, the use of iron salts indiscriminately during pregnancy has been questioned. Evidence on the effectiveness of improvement in hematological indices in pregnant women are concrete, however, information about the clinical benefits for the mother and/or newborn, both in anemic women as in non-anemic women, are controversial (Cogswell et al., 2003; Milman et al., 2005; Reveiz et al., 2011).
Approximately 87.0% (n = 608) of the respondents had their diagnosis of pregnancy between the first and twelfth week of pregnancy and 50.5% (n = 353) had seven or more prenatal visits, which is in accordance with the pro-gram of humanization in birth and prenatal care (PHPN) from the Brazilian ministry of health that recommends that the women must have at least six prenatal visits during pregnancy. Considering the educational level, 70.96% of the women had from 9 to 12 years of education. Guerra et al.(2008) found that the higher the education level and the family income of the pregnant women, the greater was the use of medications (We ob-served that there is not reference in this point). However, this relation was not observed in our study. Regarding the most commonly used drugs by the pregnant women interviewed, they are similar to data from other studies in the literature (Table 2) (Andrade et al., 2004; Brum et al., 2011; Fonseca et al., 2002; Rashmi et al., 2006). Among the drugs mentioned by pregnant women, 13.69% (n = 448) were used without medical prescription and the majority of them are classified as OTC drugs. Antacids were used by 4.9% of pregnant women. Among them, aluminum hydroxide, which belongs to the risk category C, showed the highest prevalence of use (11.44%).
In a study conducted in Fortaleza (Brazil) with pregnant women, self-medication was reported by 11.3% of their sample and during the first trimester the highest prevalence was of anti-inflammatory drugs (Rocha et al., 2013). Self-medication, in the present study, may have been underestimated due to the embarrassment of the user in admitting the consumption of medication without the knowledge of the physician to interviewer. Self-medication is a common practice in Brazil, however the use of medications without the doctor's consent can be extremely dangerous, especially during pregnancy.
According to the FDA risk classification for medications used during pregnancy, 14.07% (n = 463) of the drugs were classified as risk category C and 1.85% (n = 61) risk category D. Higher medication consumption was des- cribed by Gagne et al. (2008) and Kebede et al. (2009) as 19.0 and 2.0%, and 15.2 and 3.3% risk categories C categories C and D, respectively. Carmo and Nitrini (2004) suggested that about 40% of the drugs prescribed for pregnant women are drugs whose safety of use during pregnancy can be questioned.
Studies show that the rate of use of vitamins during pregnancy varies considerably. In this study, 53.22% of the pregnant women used vitamin supplements. Pouchieu et al. (2013) realized a study in France and found that 64.9% of the pregnant women that participated in the research consumed vitamin supplements. In another study conducted in Brazil, Oliveira and Fonseca (2007) found that 16.7% of pregnant women used vitamins. In the intercontinental study CGDUP (1992), the use of vitamins by pregnant women from 22 different countries ranged from 4 to 100%. Due to the metabolic changes that occur during pregnancy, the need for vitamins by pregnant women increases by 50%. Thus, health professionals recommend the use of vitamin complexes to supplement the demand of micronutrients (British Nutrition Foundation - BNF, 2013; Nakamura et al., 2008; Williamson and Wyness, 2013). It is important to highlight that vitamins, when not used in excess, are included in the risk category A. However, when used in excess, these micronutrients become part of the risk category C, except the vitamin A, which is classified as risk category X. Vitamin A combined to vitamin D is part of the risk category B (Lacy et al., 2008). Thus, the ne-cessity of using vitamin complex during pregnancy should be carefully analyzed. The composition, doses and real need should be always revised before prescribing these drugs to pregnant women.
Analgesics were the drugs most commonly used by pregnant women and acetaminophen was the most con-sumed (57.8%). Similarly, Thorpe et al. (2013) found in a case control study that analgesics are largely consumed by pregnant women and acetaminophen was the most used. The use of this medicine during pregnancy is not associated with increased risk of abortion, stillbirth, low weight birth or increased prevalence of congenital ano-malies (Rebordosa et al., 2008; Rebordosa et al., 2009). However, an association between use of acetaminophen during pregnancy and the prevalence of childhood asthma has been demonstrated (Henderson and Shaheen, 2013; Persky et al., 2008; Rebordosa et al., 2008a). Therefore, the prescription of this drug for preg-nant women should be done with caution. Antibiotics are drugs widely used in pregnancy (de Jonge et al., 2013; Fonseca et al., 2002; Mengue et al., 2001). In this study, amoxicillin, cephalexin and norfloxacin were used by 18% of patients. Fonseca et al. (2002) observed a similar rate of use of antibiotics for systemic use in pregnant women (15.8%) and similar data (20.8%) were also observed in a study conducted by de Jonge et al. (2013). It should be noted that antibiotics that act by inhibiting bacterial cell wall synthesis have great selective toxicity and therefore, low potential toxicity to the pregnant woman and the fetus. Penicillins and cephalosporins exhibit this mecha-nism being the most suitable for use during pregnancy (Fonseca et al., 2002).
In therapeutic subgroup of antiemetics and antinauseants, the most commonly used drug by pregnant women was scopolamine (24.32%) classified as risk category C. These results are in accordance with other studies of literature (Brum et al., 2011; Fonseca et al., 2002). When we associate the number of medications used by women during pregnancy with the independent variables studied, using both univariate and multivariate polytomous logistic regression, we can observe that most of them showed no association. The number of prenatal visits was the only variable that presented association with the amount of used drugs. Pregnant women who underwent more than six prenatal visits during pregnancy used a lower number of drugs in both statistical analyzes than those that had less than six prenatal visits (univariate p = 0.01, multivariate p = 0.02). This asso-ciation may be due to a higher concern by physicians in prescribing medications to this population and also because pregnant women that have more prenatal visits present a better awareness about the risks of taking medications than the women that have fewer visits. In contrast, other studies have observed an increased number of drugs used by pregnant women who had a greater number of prenatal visits (Brum et al., 2011; Fonseca et al., 2002). This fact may occur since these women have more health problems during pregnancy than the women that have fewer visits or also due to a belief that the patient needs always to leave the medical appointment with a medical prescription.
It is important to highlight that the U.S. Food and Drug Administration (FDA) pregnancy risk classification (A, B, C, D, X) is not a golden standard. It is an imprecise risk category system that renders risk versus benefit assessment difficult. Since 2008, the FDA is implementing a new pregnancy and lactation labeling rule with the purpose of improving risk versus benefit assessment of drugs used during pregnancy and lactation. This new rule will provide detailed and clear information for both patients and health care providers and will contain three main categories: risk summary, clinical considerations and data (Ramoz and Patel-Shori, 2014). However, as the new rule is still being developed and the previous classification (A, B, C, D, X) is widely known and used to classify drugs used by pregnant women, we chose this categorization.
One strength of the study is that it is representative, since the majority of low risk pregnant women attending the Brazilian public health system receive similar treatment as that provided by MATER. In Brazil, about 80% of the population depends exclusively on the public health, which might be the same for pregnant women. This study has some limitations. Since data were collec-ted via interviews after the 32nd week of pregnancy, some of the pregnant women were unable to recall all the medications taken during pregnancy. Sometimes they did remember they used a medication but they could only remember the indication, not the correct name. Some women had their diagnosis of pregnancy after the 12th week of the gestation period (13.02%), which may indicate that they probably did not pay much attention to the use of medication before that period.
This study showed a high prevalence of medication use among pregnant women and it was possible to identify the medications that are most widely used among this population. This information shows there is a need to continuously investigate the risks and benefits of the use of some medications during pregnancy and also its consequences after the childbirth. There is also a need to provide accurate information about the medications that are required or should be avoided during pregnancy. Continuous education by health professionals are essential tools to provide better quality information to the pregnant women and consequently improve their awareness of the harm some medications can cause to the fetus.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGMENTS
The authors would like to thank School of Pharmaceutical Sciences of Ribeirão Preto - University of São Paulo and the Center of Reference of Women's Health of Ribeirão Preto – MATER (CRSMRP- MATER) for its support and the Coordenação de Aperfeicoamento de Pessoal de Nível Superior (CAPES) for funding the research.
REFERENCES
|
Andrade SE, Gurwitz JH, Davis RL, Chan KA, Finkelstein JA, Fortman K, McPhillips H, Raebel MA, Roblin D, Smith DH, Yood MU, Morse AN, Platt R (2004). Prescription drug use in pregnancy Am. J. Obstet. Gynecol. 191:398-407. Crossref |
||||
|
Antonucci R, Zaffanello M, Puxeddu E, Porcella A, Cuzzolin L, Pilloni MD, Fanos V (2012). Use of non-steroidal anti-inflammatory drugs in pregnancy: impact on the fetus and newborn. Curr. Drug Metab. 13(4):474-90. Crossref |
||||
|
Baraka M1, Steurbaut S, Coomans D, Dupont AG (2014). Determinants of medication use in a multi-ethnic population of pregnant women: a cross-sectional study. Eur. J. Contracept. Reprod. Health Care 19:108-20. Crossref |
||||
|
Baylis F (2010). Pregnant women deserve better. Nature 465:689-690. Crossref |
||||
|
Berglund F, Flodh H, Lundborg P, Prame B, Sannerstedt R. (1984). Drug use during pregnancy and breast-feeding. A classification system for drug information. Acta Obstet. Gynecol. Scand. Suppl. 126:1-55. Crossref |
||||
|
Borges ALV, Cavalhieri FB, Hoga LAK, Fujimori E, Barbosa LR (2011). Planificación del embarazo: prevalencia y aspectos asociados. [Planning pregnancy: prevalence and associated aspects]. Rev. Esc. Enferm. 45:1679-1684. Crossref |
||||
|
Boubred F, Vendemmia M, Garcia-Meric P, Buffat C, Millet V, Simeoni U (2006). Effects of maternally administered drugs on the fetal and neonatal kidney. Drug Saf. 29(5):397-419. Crossref |
||||
| Brasil RDC no 138, de 29 de maio de (2003). Dispõe sobre o enquadramento de medicamentos categoria de venda livre. [Provides the framework for OTC drugs category]. Diário Oficial da União, Brasília, DF, 29 maio. | ||||
|
British Nutrition Foundation (BNF). Nutrition and development: short- and long-term consequences for health. London: Wiley-Blackwell, 2013. Crossref |
||||
| Brum LFS, Pereira P, Felicetti LL, Silveira RD (2011). Prescribed and unprescribed drug use among pregnant patients attended by the Unified Health System in Santa Rosa (State of Rio Grande do Sul, Brazil). Ciênc. Saúde Colet. 16:2435-2442. | ||||
|
Carmo TA, Nitrini SM (2004). Drug prescription for pregnant women: a pharmacoepidemiological study. Cad. Saude Publica 20:1004-1013. Crossref |
||||
|
Cogswell ME, Parvanta I, Ickes L, Yip R, Brittenham GM (2003). Iron supplementation during pregnancy, anemia, and birth weight: a randomized controlled trial. Am. J. Clin Nutr. 78:773-81. Pubmed |
||||
|
Collaborative Group on Drug use in Pregnancy (CGDUP) (1992). Medication during pregnancy: an intercontinental cooperative study. Int. J. Gynecol. Obstet. 39:185-96. |
||||
|
Czeizel AE, Dudás I (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N. Engl. J. Med. 327:1832-1835. Crossref |
||||
|
Daw JR, Hanley GE, Greyson DL, MLIS, Morgan SG (2011). Prescription drug use during pregnancy in developed countries: a systematic review. Pharmacoepidemiol. Drug Saf. 20:895-902. Pubmed |
||||
|
de Jonge L, Bos HJ, van Langen IM, de Jong-van den Berg LT, Bakker MK (2013). Antibiotics prescribed before, during and after pregnancy in the Netherlands: a drug utilization study. Pharmacoepidemiol. Drug Saf. 23:60-8. Crossref |
||||
|
Domingues RMSM, Hartz ZMA, Dias MAB, Leal MC (2012). Avaliação da adequação da assistência pré-natal na rede SUS do Município do Rio de Janeiro, Brasil. Cad. Saúde Pública 28:425-437. Crossref |
||||
|
Fonseca MRCC, Fonseca E, Bergsten-Mendes G (2002). Prevalence of drug use during pregnancy: a pharmacoepidemiological approach. Rev. Saúde Pública 36:205-12. Pubmed |
||||
|
Gagne JJ, Maio V, Berghella V, Louis DZ, Gonnella JS (2008). Prescription drug use during pregnancy: a population-based study in Regione Emilia-Romagna, Italy. Eur. J. Clin. Pharmacol. 64:1125-1132. Crossref |
||||
| Geib LTC, Vargas-Filho EF, Geib D, Mesquita DI, Nunes ML (2007). | ||||
|
Prevalência e determinantes maternos do consumo de medicamentos na gestação por classe de risco em mães de nascidos vivos. Cad Saúde Pública 23:2351-62. Crossref |
||||
|
Giaginis C, Theocharis S, Tsantili-Kakoulidou A (2012). Current toxicological aspects on drug and chemical transport and metabolism across the human placental barrier. Expert Opin Drug Metab Toxicol. Crossref |
||||
|
Guerra GCB, Silva AQB, França LB, Assunção PMC, Cabral RX, Ferreira AAA (2008). Utilização de medicamentos durante a gravidez na cidade de Natal, Rio Grande do Norte, Brasil. Rev. Bras. Ginecol. Obstet. 30:12-18. Crossref |
||||
|
Henderson AJ, Shaheen SO (2013). Acetaminophen and asthma. Paediatr. Respir. Rev. 14:9-16. Crossref |
||||
|
Hosmer Jr DW, Lemeshow S, Sturdivant RX (2013). Applied logistic regression, 3rd Edition. Hoboken: Wiley. Crossref |
||||
|
Kebede B, Gedif T, Getachew A (2009). Assessment of drug use among pregnant women in Addis Ababa, Ethiopia. Pharmacoepidemiol. Drug Saf. 18:462-468. Crossref |
||||
| Lacy CF, Armatrong LL, Goldman MP, Lance LL (2008). Drug infor-mation handbook with international trade names index. 17th edition. | ||||
|
Lenz W (1962). Thalidomide and congenital abnormalities. Lancet. 279:45. Crossref |
||||
|
Lo WY, Friedman JM (2002). Teratogenicity of recently introduced medications in human pregnancy. Obstet. Gynecol. 100:465-473. Crossref |
||||
| Lockerbie L, Lutz W (1986). Community health surveys. A practical guide for health workers: Questionnaire design. International Epidemiological Associaton. 14:121p. | ||||
|
Lunet N, Rodrigues T, Correia S, Barros H (2008). Adequacy of prenatal care as a major determinant of folic acid, iron, and vitamin intake during pregnancy. Cad. Saúde Pública. 24:1151-1157. Crossref |
||||
|
Lupattelli A, Spigset O, Nordeng H (2013). Adherence to medication for chronic disorders during pregnancy: results from a multinational study. Int. J. Clin. Pharm. DOI 10.1007/s11096-013-9864-y. |
||||
|
Martínez-Frías ML (2012).Talidomida: 50 a-os después. [The thalidomide experience: review of its effects 50 years later]. Med. Clin. (Barc). 139:25-32. Crossref |
||||
|
McCarter-Spaulding DE (2005). Medications in pregnancy and lactation. Am. J. Matern. Child Nurs. 30:10-7. Crossref |
||||
|
McNulty B, McNulty H, Marshall B, Ward M, Molloy AM, Scott JM, Dornan J, Pentieva K (2013). Impact of continuing folic acid after the first trimester of pregnancy: findings of a randomized trial of Folic Acid Supplementation in the Second and Third Trimesters. Am. J. Clin. Nutr. 98:92-8. Crossref |
||||
|
Mengue SS, Schenkel EP, Duncan BB, Schmidt MI (2001). Uso de medicamentos por gestantes em seis cidades brasileiras. [Drug use by pregnant women in six Brazilian cities]. Rev. Saúde Pública. 35:415-420. Crossref |
||||
|
Milman N, Bergholt T, Eriksen L, Byg KE, Graudal N, Pedersen P, Hertz J (2005). Iron profilaxy during pregnancy: how much iron is needed? A randomized doseresponse study of 20-80mg ferrous iron daily in pregnant women. Acta Obstet Gynecol Scand. 84:238-247. Crossref |
||||
|
Mitchell AA, Gilboa SM, Werler MM, Kelley KE, Louik C, Hernández-Díaz S (2011) National Birth Defects Prevention Study. Medication use during pregnancy, with particular focus on prescription drugs: 1976-2008. Am J Obstet Gynecol. 205:51.e1-8. |
||||
| Mitchell AA (2000). Special considerations in studies of drug induced birth defects. In: Strom B, 3ed. Pharmacoepidemiology. Hoboken, NJ: John Wiley & Sons. ISBN: 9780470842553 | ||||
|
Myren M, Mose T, Mathiesen L, Knudsen LE (2007). The human placenta – an alternative for studying foetal exposure. Toxicol in Vitro. 21(7):1332-1340. Crossref |
||||
|
Nakamura MU, Kulay-Junior L, Pasquale M. (2008). Uso de fármacos na gravidez: benefício e custo. Rev. Bras. Ginecol. Obstet. 30:1-4. Crossref |
||||
| Oliveira ACP, Fonseca, TMM (2007). Estudo epidemiológico sobre o uso de medicamentos durante a gravidez na população atendida pelo serviço de obstetrícia do hospital municipal de Confresa – MT. Interseção. 1:102-109. | ||||
|
Oliveira MA, Bermudez JAZ, Souza ACM (1999). Talidomida no Brasil: vigilância com responsabilidade compartilhada? [Thalidomide in Brazil: monitoring with shared responsibility?] Cad. Saúde Pública 15:99-112. Crossref |
||||
|
Olney RS, Mulinare J (2002). Trends in neural tube defect prevalence, folic acid fortification, and vitamin supplement use. Semin Perinatol. 26:277-285. Crossref |
||||
|
Orbach H, Matok I, Gorodischer R, Sheiner E, Daniel S, Wiznitzer A,Koren G, Levy A (2013). Hypertension and antihypertensive drugs in pregnancy and perinatal outcomes. Am. J. Obstet. Gynecol. 208:301.e1-6. |
||||
| Oxford Dictionaries (2014). Available at: <http://www.oxforddictionaries.com/definition/english/medication> Accessed 22nd July 2014. | ||||
| Pangle BL (2006). Drugs in Pregnancy and Lactation. In: Herfindal ET, Gourley DR (eds.), Text book of Therapeutics, Drug and Disease Management 8th ed. Philadelphia: Lippincott William Wilkins. pp. 434-448. | ||||
|
Papaseita E, Garcia-Algarb O, Farré M (2013). Talidomida: una historia inacabada. [Thalidomide: an unï¬nished history]. An. Pediatr. 78:283-287. Crossref |
||||
|
Persky V, Piorkowski J, Hernandez E, Chavez N,Wagner-Cassanova C, Vergara C, Pelzel D, Enriquez R, Gutierrez S,Busso A l (2008). Prenatal exposure to acetaminophen and respiratory symptoms in the first year of life. Ann. Allergy Asthma Immunol. 101:271-8. Crossref |
||||
|
Rachel Lévy, Céline Faure,Valentina A. Andreeva,Pilar Galan,Serge Hercberg,Mathilde Touvier (2013). Socioeconomic, Lifestyle and Dietary Factors Associated with Dietary Supplement Use during Pregnancy. PLoS ONE. 8: e70733. Crossref |
||||
|
Prévot A, Martini S, Guignard JP (2002). In útero exposure to immunosuppressive drugs. Biol. Neonate 81(2):73-81. Crossref |
||||
|
Ramoz, LL, Patel-Shori NM (2014). Recent Changes in Pregnancy and Lactation Labeling: Retirement of Risk Categories. Pharmacotherapy 34:389-395. Crossref |
||||
|
Rashmi S, Bhuvneshvar K, Ujala V (2006). Drug utilization pattern during pregnancy in North Índia. Indian J. Med. Sci. 60:277-87. Crossref |
||||
|
Rebordosa C, Kogevinas M, Bech BH, Sørensen HT, Olsen J (2009). Use of acetaminophen during pregnancy and risk of adverse pregnancy outcomes. Int. J. Epidemiol. 38:706-14. Crossref |
||||
|
Rebordosa C, Kogevinas M, Horváth-Puhó E, Nørgård B, Morales M, Czeizel AE, Vilstrup H, Sørensen HT, Olsen J (2008). Acetaminophen use during pregnancy: effects on risk for congenital abnormalities. Am. J. Obstet. Gynecol. 198:178.e1-7. |
||||
|
Rebordosa C, Kogevinas M, Sørensen HT, Olsen J (2008). Pre-natal exposure to paracetamol and risk of wheezing and asthma in children: A birth cohort study. Int. J. Epidemiol. 37:583-590. Crossref |
||||
| Reveiz L, Gyte GM, Cuervo LG, Casasbuenas A (2011). Treatments for iron-deficiency anaemia in pregnancy (Review). Cochrane Database Syst. Rev. 2: CD003094. | ||||
|
Rocha RS, Bezerra SC, Lima JW, Costa Fda S (2013). Consumption of medications, alcohol and smoking in pregnancy and assessment of teratogenic risks. Rev. Gaucha Enferm 34:37-45. Crossref |
||||
|
Schantz SL (1996). Developmental neurotoxicity of PCBs in humans: what do we know and where do we go from here? Neurotoxicol. Teratol. 18:217-227. Crossref |
||||
|
Smithells RW, Sheppard S, Schorah CJ, Seller MJ, Nevin NC, Harris R, Read AP, Fielding DW (1980). Possible prevention of neural-tube defects by periconceptional vitamin supplementation. Lancet 1:339-340. Crossref |
||||
|
Swan SH (2008). Intrauterine exposure to diethylstilbestrol: long-term effects in humans. APMIS 108:793-804. Crossref |
||||
|
Thorpe PG, Gilboa SM, Hernandez-Diaz S, Lind J, Cragan JD, Briggs G, Kweder S, Friedman JM, Mitchell AA, Honein MA (2013). Medications in the first trimester of pregnancy: most common exposures and critical gaps in understanding fetal risk. Pharmacoepidemiol. Drug Saf. 22:1013-1018. Pubmed |
||||
|
Tilson HA, Kodavanti PR, Mundy WR, Bushnell PJ (1998). Neurotoxicity of environmental chemicals and their mechanism of action. Toxicol. Lett. 102-103, 631-635. Crossref |
||||
|
Torres M, Moayedi S (2012). Gynecologic and other infections in pregnancy. Emerg. Med. Clin. North Am. 30:869-884. Crossref |
||||
|
Ward RW (2001). Difficulties in the study of adverse fetal and neonatal effects of drug therapy during pregnancy. Semin Perinatol. 25:191-195. Crossref |
||||
| West JR, Blake CA. (2005). Fetal alcohol syndrome: an assessment of the ï¬eld. Exp. Biol. Med. 230:354-356. | ||||
|
Williamson C, Wyness L (2013). Nutritional requirements in pregnancy and use of dietary supplements. Community Pract. 86:44-47. Pubmed |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


