Full Length Research Paper

ABSTRACT
The study of prescribing pattern is a significant constituent of medical review, which helps in monitoring, evaluating and building required modifications in the prescribing practices to attain a rational and cost effective medical care. The present study determined the trends in drug prescription pattern of clinicians in private and general hospitals in Makkah, Saudi Arabia. One thousand two hundred and thirty two prescriptions were collected from private and general hospitals between March and September, 2013. The prescriptions were subjected to analysis using the World Health Organization (WHO) drug use indicators. The study cleared that all collected prescriptions were titled with the name of hospital and some were handwritten and the others were computer printouts. Readability was evident in 58.3% of handwritten prescriptions. The name, address, date, license number, and signature of the prescriber was presented in 71.8, 95.1, 71.8, 47.4 and 77.9% of all prescriptions, respectively. Name of patient, age, sex and address were presented in 81.5, 64.0, 61.0 and 20.5% in all prescriptions, respectively. The diagnosis of complaint or a history of allergy was presented in 44.5 and 12.7%, respectively of all prescriptions. The prescribed drugs in a generic name were 32.8% of all prescriptions. The strength, the drug dosage form, the route and frequency of administration of the prescribed drug were presented in 84.1, 58.1, 33.8 and 93.2% of all prescriptions, respectively whereas, duration of treatment was mentioned in only 12.0% of total prescriptions. The average number of drugs per encounter was 2.8. Prescribers were prescribed one, two, three, four, five or more than five drugs per prescription in 1.7, 41.1, 35.3, 16.2, 3.7 and 2.3%, respectively. This study revealed that it is necessary to further improve drugs prescribing practice. This calls for sustained interventional strategies and periodic review at all levels of healthcare for the avoidance of negative consequences of inappropriate prescription. Polypharmacy and low rate of generic prescriptions remain problems in healthcare facilities.
Key words: Prescribing practice, drug use indicator, hospitals, prescriptions.
INTRODUCTION
Once a patient with a health problem has been evaluated and a diagnosis has been reached, the clinician usually selects a drug therapy regimen from a variety of therapeutic approaches. This requires a writing of a drug prescription. Prescription writing is not simply putting a few drug names on a piece of paper, rather it is a skill which can be attained only after years of practice, hard work and sound knowledge of the basic subject (Sharif et al., 2008; Sawalha et al., 2010; Ather et al., 2013).
Several studies have explored irrational drug use (Sharif et al., 2008; Tamuno and Fadare, 2012; Mathew et al., 2013; Sharif et al., 2013). A set of core drug use indicators which are useful for studying patterns of drug prescriptions in healthcare services was designed by World Health Organization (WHO) (How to investigate drug use in health facilities, EDM Research Series No.: WHO/DAP/93.1, 1993; Quick et al., 2002). The main way to study the prescribing physician and the dispensing pharmacist responsible for any misconduct in prescribing or dispensing is through issued drug prescriptions (The Pharmaceutical Professions and Institutions, 1983). Consequences of irrational drug prescribing include exhaustion of the limited health budget, increased incidence of serious adverse effects, drug interactions, non-compliance and emergence of antibiotics-resistant microbial strains (Sharif et al., 2008).
In accordance to Kingdom of Saudi Arabia (KSA) health regulations, the ideal prescription should contain the patient’s demographic and health information such as name, age, sex, address, and a provisional diagnosis of the case targeted by the drug therapy. Equally, the prescriber’s information should include name, address, and signature, means of contact, specialty, and medical license number (DeVries et al., 1995). Analysis of prescriptions can pinpoint defects and the results of such studies can be utilized as an effective interactive by discussing it with the prescribers and health authorities to promote rational drug prescribing. Adherence by the physician, to good quality prescribing will minimize errors and ultimately improve patient care. Prescribing errors can occur as a result of errors in decision making or the prescription writing process (Sharif et al., 2013).
To the best of our knowledge, this study is the first of its kind that explored secondary healthcare in Makkah region of Saudi Arabia as other study was carried out in private and public primary healthcare centers (Neyaz et al., 2011). The present study aimed to analyze the prescriptions issued in some private and general hospitals, covering many medical specialties’ in Makkah, Saudi Arabia. The objective was to study the prescribing pattern of consultant physicians and to explore areas in need of improvement in order to enhance communication between physicians and pharmacists in order to minimize medication errors and improve therapeutic outcomes.
1. Improved rational drug prescribing through stressing the importance of periodical prescription analysis studies.
2. Information gathered from this study will be useful for continuing education programs, which are suitable for integration in daily practice.
3. The study may help in establishing a sound national drug policy which is an integral part of our healthcare system.
4. It provides physicians with feedback on their performance and also assists to design educational programs that may improve prescribing and drug use.
METHODOLOGY
Background to the study areas
Makkah region of Saudi Arabiaserved by several private and government hospitals, for this study we randomly selected two government and two private health centers which were offering services to large population of the community.
Materials
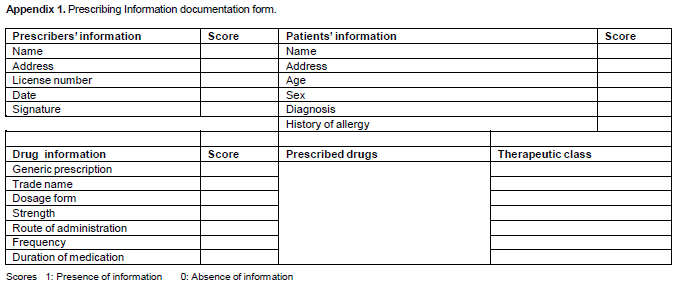
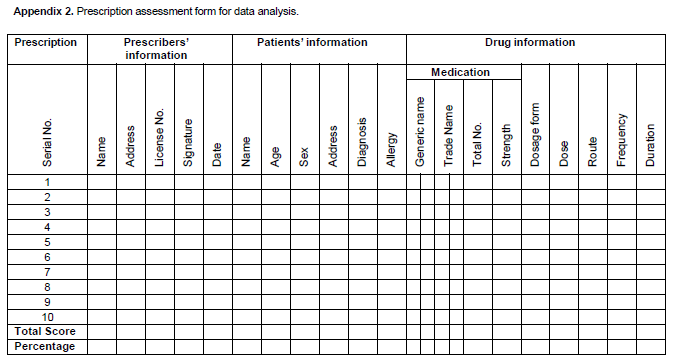
Prescriptions written by consultants were collected randomly from the pharmacies of the hospitals and examined to record information about prescribing indicators using a predesigned form shown in Appendices 1 and 2. The prescriptions were subjected to analysis using the WHO drug use indicators (How to investigate drug use in health facilities, EDM Research Series No.: 7[WHO/DAP/93.1], 1993; DeVries et al., 1995).
Data collection analysis and management
Study design
It was a retrospective descriptive study with sample a size of 1232 patients. The study was carried out over a period from March, 2013 to September, 2013.
Sampling technique
In each prescription, we analyzed the presence and deficiencies in information of patient, prescriber and the prescribed drug(s). Patient’s information includes name, age, sex, and address, provisional diagnosis, and history of drug allergy. The prescriber`s information covered name, signature, license number, and address. Regarding the prescribed drug(s), presence or deficiency of the drug strength, drug dosage form, and frequency and route of administration were determined. We also studied the readability of the prescription, the number of drugs per prescription and the extent of prescribing using generic/trade drug names. Average number of drugs per encounter were computed by simple mathematical formula as given:
Results are expressed as figures and percentage of present indicators of total number of prescriptions and presented using tables according to the types of tool used.
Ethics
The study protocol was approved by the Umm Al-Qura University Institutional Review Board (UQUIRB) for ethical clearances (dated 20 February 2013).
RESULTS
All collected prescriptions were titled with the name of hospital and some were handwritten and the others were computer printouts. The readability confirmed by pharmacists was evident in 58.3% of handwritten prescriptions.
Data of prescriber
The name, address, date, license number, and signature of the prescriber were documented in 71.8, 95.1, 71.8, 47.4 and 77.9% of all prescriptions, respectively (Figure 1).
Data of patient
Name of patient, age, sex and address were documented in 81.5, 64.0, 61.0 and 20.5% of all prescriptions, respectively. The patient`s diagnosis, complaints or history of allergy were indicated in 44.5 and 12.7%, respectively of all prescriptions (Figure 2).
Data on prescribed drugs
The prescribed drugs in a generic name were 32.8% of all prescriptions. The strength, the dosage form, the route and frequency of administration of the prescribed drugs were presented in 84.1, 58.1, 33.8 and 93.2% of all prescriptions respectively, whereas duration of treatment was only mentioned in 12.0% of prescriptions (Table 1). The average number of drugs per encounter in our study was 2.8. The prescribers prescribed one, two, three, four, five or more drugs per prescription in 1.7, 41.1, 35.3, 16.2, 3.7 and 2.0% cases, respectively (Table 2).
DISCUSSION
The present study was aimed to assess physician`s prescribing practices which influence the patient`s compliance and therapeutic success or failure. Analysis of different parameters in the prescriptions in the present study provided an idea about the prescribing pattern of the consultant physicians in Makkah, Saudi Arabia. WHO developed a core prescribing indicators to measure the degree of the tendency to prescribing drugs using generic name. The prescriptions are a legal document that can be used for or against the physician or the pharmacist in case of prescribing or dispensing error (The Pharmaceutical Profession and Institutions) (Irshaid et al., 2005; Sharif et al., 2013). A prescription provides an insight into a prescriber’s attitude to the disease being treated and the nature of healthcare delivery system in the community (DeVries et al., 1995). Using the WHO prescribing indicators, this study has provided a better understanding of the prescribing practices in the ability being studied and has shown areas that need interference.
The difficulty associated with reading of handwritten prescriptions was obvious in all analyzed cases. It is similar to some other studies conducted in Saudi Arabia (Irshaid et al., 2005) and United Arab Emirates (Sharif et al., 2013) while it was much higher than another study from Saudi Arabia (Balbaid and Al-Dawood, 1988), Sudan (Yousif et al., 2006) and in USA (Meyer, 2000). In the previous study (Irshaid et al., 2005), a single unclear word or dose units were encountered but in this present study unreadable drug names was observed. Harmful drug effects could occur due to unclear drug names and lookalike drugs that may lead to dispensing errors (Charatan, 1999).
In this study, prescriptions analysis explored that diagnosis of the complaints targeted by the prescribed drug was indicated in 44.5% this was 15% higher than the case recorded in another study from Saudi Arabia (Irshaid et., 2005) and a history of drug allergy was indicated in 12.7% cases. In this context, it is noted that the name of the prescribed drug does not always reflect its therapeutic indications particularly, for drugs with multi-therapeutic uses. Moreover, ignorance of history of allergy, if any, may prove hazardous to the patient. Although the dosage forms of the drug was mentioned in 58% of prescriptions, it was not indicated in more than 40% of prescriptions. In addition, route of administration did not feature in about 66% of prescriptions. This may add to the role of the dispensing pharmacist as complimentary to that of the prescribers. A competent pharmacist plays a role as an active member of the healthcare team for the benefit of the patient. This is easier for a hospital pharmacist who can communicate with the prescribing physician in the same health organization as compared to a community pharmacist. However, with the drugs prescribed, it is important for the prescriber to be in charge of dose, route and frequency of administration especially, where the doses are selected on basis of various parameters that require frequent monitoring by the physician in case of chronic diseases. Prescribing by generic names is the expected standard for clinicians. However, only 32.8% of prescribed drugs in this study were prescribed by generic names. Increasing generic prescribing could significantly reduce the cost of drugs not only for the patients but also for pharmacies. This low generic prescribing appears to be consistent with studies from Nigeria (Isah et al., 2002; Chedi et al., 2004) and Nepal (Kafle et al., 1992). But, it is still much lower than that reported for Cambodia (Chareonkul et al., 2002), Bangladesh (Guyon et al., 1994), China (Jun et al., 2011), India (Vijayakumar et al., 2011) and Iran (Ghadimi et al., 2011), where generic prescribing reached 78, 73, 72 and 96%, respectively. Prescribing by generic names though higher than that of 4% in the earlier study was conducted in Dubai (Sharif et al., 2008).
The low percent (32.8) generic prescribing in our study can be attributed to the lack of emphasis on that aspect in medical training and practice and also to the influence of promotional activities of local and international pharmaceutical companies on physicians` decisions (Sharif et al., 2013). Generic prescribing tends to reduce cost and rationalize drug use (Quick et al., 2002). Introduction of concepts of list of essential drugs, generic prescribing and good prescription writing in medical curriculum seems to be necessary.
It is on record that over 120 developing countries have adopted the essential drugs concept and developed a national essential drugs list (Model list of essential medicines 16th list WHO, 2010). Prescribing by trade or brand names negates this concept. In addition to the lower economic cost to patients and health systems, generic prescribing will eliminate or reduce the incidence of therapeutic duplication errors (Model list of essential medicines 16th list WHO, 2011). Duplicate drug ingestion accidentally occurs when the patient takes the generic and brand name drugs for example, Digoxin plus Lanoxin® (Glaxo Smith Kline). In health facilities and systems loaded with high levels of polypharmacy, where patients fight with proper compliance with their old regimen, low generic prescribing will add to their confusion and possibly increase the incidence of adverse events (Lazarou et al., 1998).
Average number of drugs per encounter is a significant index for the scope of educational intervention in prescribing practices. Our results showed 2.8 drugs per prescription. which is higher than WHO recommended limit of < 2. Higher average number of drugs per visit were reported in some studies from India (Vijayakumar et al., 2011; Mathew et al., 2013) and Nigeria (Tamuno and Fadare, 2012) 3.01, 2.99 and 3, respectively. All of these studies reflected poor quality of pharmacotherapy. In our study, 16.2 and 3.7% of prescriptions contained four and five drugs, respectively while only 2.0% contained more than five drugs per visit. Our results for prescriptions with more than four drugs are slightly less than that of recently reported study from India (Vijayakumar et al., 2011). Polypharmacy is a common fault in prescription writing which contributes to the risk of increased incidence of serious drug interactions and harmful drug adverse reactions. Dispensing errors and patient`s compliance could also occur.
Prescribing more than one drug per common practice in general and private clinic and findings from our study are consistent with other studies showing high rates of polypharmacy. However, polytherapy is generally dispirited, but it is adequate in certain conditions and is perhaps predictable in elderly patients who are often suffering from multiple chronic diseases (Chobanian et al., 2003).
The process of drug prescribing evaluation, that provide feedback concerning prescribers, offers a way of relaying data which has been subjected to assessment and may help in getting better quality prescribing. This may be achieved if the prescriber is aware that there is a problem and he is ready to devise his own drug prescribing pattern (Harding et al., 1985).
Any drug prescribing study based on WHO core drug use indicator has limitations. The major limitation of this study is the fact that it was limited to only one city/area hence the result cannot be generalized. However, the study represents a preliminary analysis in a complex area of prescribing. The one-day prescription selection strategy can be expanded to improve the sample size. A larger sample size may help in achieving further statistical and significant power for the results obtained. This research was conducted in Makkah region of Saudi Arabia and therefore the extent to which its findings could be generalized throughout Saudi Arabia is unknown. Future
studies should explore prescribing trends in rural regions of Saudi Arabia. Computerized prescribing data collection systems would facilitate a more detailed analysis of prescribing. Computerization of dispensing in healthcare services has potential for large-scale analyses of prescribing in the future which should not be underestimated.
CONCLUSION AND RECOMMENDATIONS
The present study indicated the need for further improvement to prescription writing and assessment of drug use for clinical, educational and economic purposes. It seems reasonable to promote rational drug prescribing by emphasizing the importance of periodic prescription analysis studies and the need to include concepts of essential drug list and prescription writing in medical curriculum and continuing medical education programs.
The results may be beneficial to Ministry of Health (MOH) officials in their overall health policy planning. Such data collection provides baseline data for the drug prescribing patterns in Saudi Arabia. Taking advantage of this insight into current prescribing patterns may provide the possibility of evaluating prescribing practices and in developing policies for drug use. The information and experience gathered from this study are useful elements, serving as a feedback for continuing education programs, which are suitable for integration in daily practice.
Establishing a sound national drug policy is an integral part of any healthcare system. These data need to be collected and analyzed on a continuous basis and the recommendations and feedback provided to policy makers. To achieve this, MOH and other institutions providing healthcare services in Saudi Arabia may be able to establish a pharmaco-epidemiology or drug utilization unit in cooperation with the Colleges of Pharmacy and Medicine.
ACKNOWLEDGEMENTS
This research received no specific grant from any funding agency. We gratefully acknowledge the assistance of our students throughout the study period.
CONFLICTS OF INTEREST
The author(s) declare(s) that they have no conflicts of interest.
REFERENCES
|
Ather A, Neelkanthreddy P, Anand G, Manjunath G, Vishwanath J, Riyaz M (2013). A study on determination of prescription writing errors in out patient department of medicine in teaching hospital. Indian J. Pharm. Pract. 6(2):21-24. |
|
|
Balbaid OM, Al-Dawood KM (1988). Assessment of physician's prescribing practices at Ministry of Health hospitals in Jeddah city, Saudi Arabia. Saudi Med. J. 19:28-35. |
|
|
Charatan F (1999). Family compensated for death after illegible prescription. Br. Med. J. 319(7223):1456. |
|
|
Chareonkul C, Khun VI, Boonshuyar C (2002). Rational Drug Use in Cambodia: Study of Three Pilot Health Centers in Kampong Thorn Province. South-East Asian J. Trop. Med. Public Health 33:418-424. |
|
|
Chedi BAZ, Abdu-Aguye I, Kwanashie HO (2004). WHO Core Prescription Indicators: Field Experience in Public Health Facilities in Kano, Nigeria. BEST J. 6(3):66-70. |
|
|
Chobanian AV, Bakris GL, Black HR, Cushamn WC, Green LA, Izzo JL (2003). The seventh report of the joint national committee on prevention, detection, evaluation and treatment of high blood pressure. The JNC 7 report. J. Am. Med. Assoc. 289:2560-75. |
|
|
DeVries TPGM, Henning RH, Hogerzeil HV, Fresle DA (1995). Guide to good prescribing: a practical manual. Geneva, World Health Organization; 515 WHO/DAP/94.11 Available at: http://apps.who.int/medicinedocs/pdf/whozip23e/whozip23e.pdf |
|
|
Ghadimi H, Esmaily HM, Wahlstrom R (2011). General practitioners' prescribing pattern for the elderly in a province of Iran. Pharmacoepidemiol. Drug Saf. 20(5):482-487. |
|
|
Guyon AB, Barman A, Ahmed JU, Ahmed AU, Alam MS (1994). A baseline survey on use of drugs at the primary healthcare level in Bangladesh. Bull. WHO 72(2):265-71. |
|
|
Harding JM, Modell M, Freudenberg S, MacGregor R, Rea JN, Steen CA, Wojciechowski M, Yudkin GD (1985). Prescribing: the power to set limits. Br. Med. J. 290:4503. |
|
|
How to investigate drug use in health facilities: selected drug use indicators (1993). EDM Research Series No.: 7[WHO/DAP/93.1]. Geneva: World Health Organization. |
|
|
Irshaid YM, Al Homrany M, Hamdi AA, Adjepon-Yamoah KK, Mahfouz AA (2005). Compliance with good practice in prescription writing at outpatient clinic in Saudi Arabia. East Mediterr. Health J. 11(5, 6):922-28. |
|
|
Isah AO, Laing R, Quick J, Mabadeje AFB, Santoso B, Hogerzeil H, Ross-Degnan D (2002). The Development of Reference Values For the World Health Organization (WHO) Health Facility Core Prescribing Indicators. West Afr. J. Pharmacol. Drug. Res. 18(1 and 2): 6-11. |
|
|
Jun Z, Linyun L, Che Z, Yuanrong Y, Fengxi G, Heng Z (2011). Analysis of outpatient prescription indicators and trends in Chinese Jingzhou Area between September 1and 10, 2006-2009. Afr. J. Pharm. Pharmacol. 5(2):270-275. |
|
|
Kafle KK, Karkee SB, Prasad RR (1992). INRUD Drug Use Indicators in Nepal: Practice Patterns in Health Post in Four Districts. INRUD News. 3:15. |
|
|
Lazarou J, Pomeranze BH, Corey PN (1998). Incidence of Adverse Drug Reactions in Hospitalized Patients: A Meta-Analysis of Prospective Studies. JAMA. 279(15):1200-1205. |
|
|
Mathew B, Rahul S, Kumar S, Doddayya H (2013). Assessment of drug prescribing practices using WHO prescribing indicators in a privative tertiary care teaching hospital. Int. Res. J. Intervent. Pharm. Sci.1(2):26-31. |
|
|
Meyer TA (2000). Improving the quality of the order-writing process for inpatient orders and outpatient prescriptions. Am. J. Health Syst. Pharm. 57(Suppl. 4): S18-2. |
|
|
Neyaz Y, Khoja T, Qureshi NA, Magzoub MA, Haycox A, Walley T (2011). Medication prescribing pattern in primary care in Riyadh city. Eastern Mediterr. Health J. 17(2):149-155. |
|
|
Quick JD, Hogerzeil HV, Velasquez G, Rago L (2002). Twenty-five years of essential medicines. Bull. WHO 80(11):913-14. |
|
|
Sawalha AF, Sweileh WM, Zyoud SH, Al-Jabi SW, Bni Shamseh FF, Odah AA (2010). Analysis of prescriptions dispensed at community pharmacies in Nablus, Palestine. East. Mediterr. Health J. 16(7):788-492. |
|
|
Sharif SI, Al-Shaqra M, Hajjar H, Shamout A, Wess L (2008). Patterns of drug prescribing in a hospital in Dubai, United Arab Emirates. Libyan J. Med. 3(1):10-12. |
|
|
Sharif SI, Aladfouli AH, Sharif SR (2013). Drug prescribing trends in a general hospital in Sharjah, United Arab Emerates. Am. J.Pharmacol. Sci. 1(1):6-9 |
|
|
Tamuno I, Fadare J (2012). Drug prescription pattern in a Nigerian tertiary hospital. Trop J Pharm Res. 11(1):146-125. |
|
|
The Pharmaceutical Professions and Institutions (1983). UAE Federal Law No: 4. |
|
|
Vijayakumar TM, Sathyavati D, Subhashini T, Sonika G, Dhanaraju MD (2011). Assessment of prescribing trends and rationality of drug prescribing. Int. J. Pharmacol. 7(1):140-43. |
|
|
Yousif E, Ahmed AM, Abdalla ME, Abdelgadir MA (2006). Deficiencies in medical prescriptions in a Sudanese hospital. East Mediterr. Health J. 12(6):915-18. |
|
|
WHO (2010) Model list of essential medicines 16th list. Available at: http;//www.who.int/medicines/publications/essentialmedicines/en/. |
|
|
WHO (2011) Model list of essential medicines 16 list. Available at: http://www.who.int/medicines/publications/essentialmedicines/en/. |
|
APPENDIX
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


