Full Length Research Paper

ABSTRACT
Female genital mutilation is still a serious health problem in Ethiopia. Female genital mutilation conceptualizes harmful traditional practice and is among existing traditional attitudes and practices on practice in different corners of the world. Other than demographic and health survey data, studies showing the prevalence of female genital mutilation is scarce and in some areas nonexistent. Its existence is only, time and again recognized as the practice has various health, social and psychological adversities. This study team found it imperative as the problem warranty study with the aim to assess prevalence of female genital mutilation (FGM) as well as identifying its associated factors among high school students. Institution based cross sectional study design was employed. 95% confidence level and 3% margin of error were used to study the magnitude and associated factors of FGM among 798 high school and preparatory students. A multi stage sampling procedure was employed to select female students in the schools. This research showed percentages and association among the variables by univariate, bivariate and multivariate analysis. Data were collected from 769 study participants with a response rate of 96.4%. About 78%, 95% CI (74.9%, 80.7%) of the study participants underwent the procedure. Age ≥17 [AOR=1.8, 95% CI (1.28, 2.61)], grades 11 and 12 [AOR =2.98; 95% CI (1.45, 6.12)] and [AOR=6.52, 95% CI (1.85, 22.94)], respectively, being from rural area [AOR= 1.6, 95% CI (1.01, 2.52)], and house wife and merchant mother occupation [AOR= 2.38, 95% CI (1.07, 5.29)] and [AOR= 2.72, 95% CI (1.04, 7.12)], respectively were independently associated to higher prevalence of female genital mutilation. Irrespective of different forms of interventions in the country, the prevalence of female genital mutilation is still very high in the study area. This study thus revealed that palatable and very convenient intervention strategies need to be crafted to curb the problem at large and for those rural villagers who are at higher risk in particular.
Key words: Female genital mutilation (FGM), high school students, Ethiopia.
INTRODUCTION
Female genital cutting, also termed female genital mutilation (FGM), pertains to any interventions that may involve injury or removal of the female external genitalia either partial or total for any reasons other than therapeutic (World Health Organization, 2006, 2008). The practice was first known as female circumcision, but since the late 1970s this was replaced by the term female genital mutilation (FGM) to give a better reflection of the violation of the woman or girl's basic human rights (World Health Organization, 2008; UNICEF, 2005a; Emam et al., 2011). The practice is widespread in 28 African countries, concentrated around the belt of the Sahel (Wagner, 2011; World Health Organization, 2011; USAID, 2012). Besides, it transcends the aforementioned geographical patterns and similarly practiced in some parts of Middle East and Asia. The practice is also found among immigrants from these areas to Europe, North America, and Australia. Although the practice has been exercised in most developing countries of various cultures, there is no definitive evidence documenting when or why this ritual begun. Some theories suggest that FGM might have been practiced in ancient Greece, Rome, Pre-Islamic Arabia and the Russian Federation (Konjit, 2002).
According to World Health Organization (WHO), about 130 million women and girls in the world have been victims of some kind of FGM. It has also been estimated that each year about three million girls are at risk or are subjected to some kind of ablation, essentially in the 28 countries in sub-Saharan Africa, where this type of ritual has strong, ancestral roots (Mitike and Deressa, 2009; Kaplan et al., 2009). During 2005/2006, the prevalence of FGM/FGC in 27 African countries ranges from 97.9% in Somalia to 0.6% in Uganda and according to EDHS 2005, this value was 74.3% in Ethiopia and 87.2% in Oromia National Regional State (Population Reference Bureau, 2010).
In Ethiopia, if not all or completely holistic for the whole society there are traditional practices that are mostly indigenous in almost all ethnic cultures, which affect the healthy functioning of people, goals, of equality and hinder developmental strategies proposed in different walks of life time. Women and children are more prone to the problem resulted from traditional practices and as a result suffer the negative impacts in which FGM particularly is among the violent traditional action against women. Female genital mutilation (FGM) or mutilating genitals of female is not a new phenomenon and it was in existence long before the beginning of Christianity and Islam as described earlier in this article. It is a national problem because not only it does and influence the physical, mental, and social life of more than half of Ethiopian population that is women or concerned sex, it also has its own impacts on the socio economic development of the country. Study of this type targeting on prevalence and factors associated is of remarkable input for designing very sound evidence based intervention with the desire to bring sound achievements in the area.
MATERIALS AND METHODS
Study design and population
A descriptive cross-sectional study was utilized in conducting this study during January, 2012. The study was conducted in Dale Wabera Woreda of Kelem Wollega zone, Oromia regional state. The source population were all female students who were enrolled in the two high schools and one preparatory school of the study area in the academic year 2011/2012.
Sample size and sampling procedures
The sample size for the quantitative study was estimated using the single population proportion formula with the assumption of 3% margin of error (d), 95% confidence level (zα/2 =1.96) and 87% proportion of FGM of Oromia region taken from Ethiopian Demographic and Health Survey (EDHS) 2005 (Central Statistical Agency, 2005) and using a design effect of 1.5, the calculated sample size with 10% contingency for non-response was 798.
A multi stage sampling procedure was applied to select sample of female students in the schools (stratification in to grades and simple random sampling to select sections and again simple random sampling to select respondents in respective sections).
The calculated sample size was proportionally allocated to the three schools based on the student population they have. First, each school was stratified by grades (9th, 10th, 11th, and12th). Proportional allocation of sample was done to the respective grades. Secondly, sections were randomly selected from each grade and study subjects were selected by simple random sampling technique.
Data collection procedures
Instrument
Self-administered structured questionnaire which was adopted from Ethiopian Demographic and Health Survey (Central Statistical Agency, 2005) were used to collect data on socio-demographic, status of FGM and other important data related to the objective of the study.
Pre-test was done before the actual data collection started on 30 (4%) female students in the Kebe High Schoolwhich is found in the Gawo Kebe wereda.
Data collection
Data collection facilitators were experienced individuals and training was given by the principal investigator for two days specially how to create conducive environment for the respondents during data collection, how to give clarity, if there is any inconvenience.
Following an orientation, respondents filled the questionnaire in private by arranging their seat far apart from one another and not allowing their teachers to enter the room.
Data analysis
Data were entered using epi data version 3.1 and exported to Statistical Package for Social Science (SPSS) version 16 for further analysis. Data cleaning took place, during data entry by use of double entry and after data entry by simple frequency and cross tabulation and their consistency was checked. After data cleaning was completed, data were exported to SPSS version 16 for analysis. Data analyses were done through Univariate analysis to see the frequencies of the categories under each variable and the corresponding percentage for each category. We also did bivariable analysis to see association between the dependent variable (in our case female genital mutilation) and independent variables like socio-demographic variables and finally logistic regression was conducted to see the independent effect of the selected independent variables on the status of FGM using odds ratio.
Operational definitions
Female genital mutilation/cutting: This is partial or total removal of the external female genitalia or other injury to the female genital organ whether for cultural or non-therapeutic reasons (World Health Organization, 2006, 2008).
Clitoridectomy: Partial or total removal of the clitoris, with or without excision of part or all of prepuce (World Health Organization, 2006, 2008).
Infibulations: Narrowing the vaginal opening through the creation of a covering seal by cutting and repositioning the labia minora and/or the labia majora, and with or without removal of the clitoris (World Health Organization, 2006, 2008).
Defibulation: Defibulation is a surgical procedure wherein a vertical incision is made on the scar to expose the introitus and create new labia majora.
RESULTS
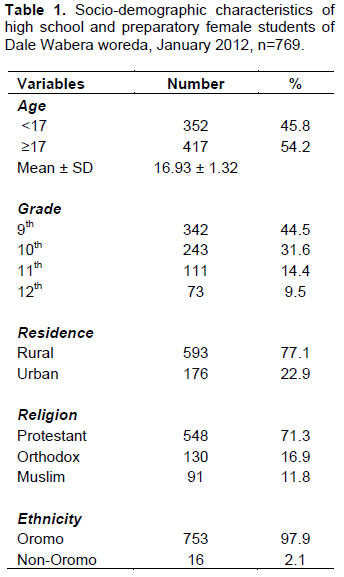
Socio-demographic characteristics
More than half of the participants (54.2%) were seventeen years old and above with a mean and SD of 16.93 and ±1.32 respectively. Three hundred and forty-two of the study participants, 44.5% (342) were from grade nine, 31.6% (243) were grade ten, and 14.4% (111) were from grade eleven. More than two-third of the study participants (77.1%) were from rural area and almost all of the study participants (97.9%) were Oromo in terms of their ethnic background, while protestant was the dominant religion in the area (71.3%) (Table1).
Ninety-five of the practice was done by traditional circumcisers and the rest was done by health professionals. Among 704 (91.5%) of the study subjects who reported that they have one or more sister(s), 63.6% of the sisters have FGM. From the total number of study subjects who reported mutilation and having sister (s), 56.4% of them have been mutilated with one or more of their sister (s) at the same time. The majority of procedure (64%) was done during night time which was followed by early morning (27.5%) and only 8.5% of it was performed at day time. About 24% of the study participants reported that FGM is required by their religion.
The majority of the respondents (77.7%) agreed with the idea of terminating the practice while 22.3% of them supported to perform FGM in the future.
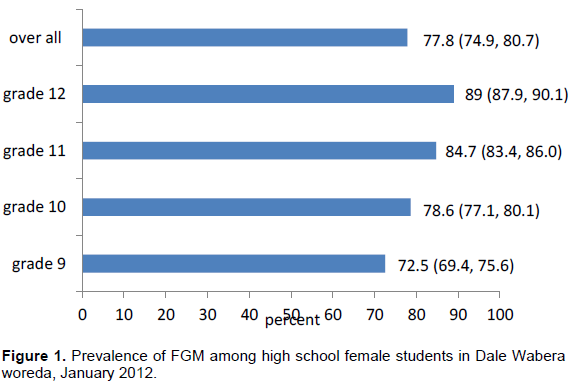
Prevalence of FGM among the high school and preparatory female students, Dale Wabera, January 2012
The overall prevalence of FGM among the study participants was 77.8%; 95% CI (74.9%, 80.7%). As it is shown below the prevalence increased from 72.5%; 95% CI (69.4%, 75.6%) in grade 9 to 89%; 95% CI (87.9%, 90.1%) in grade twelve (Figure 1).
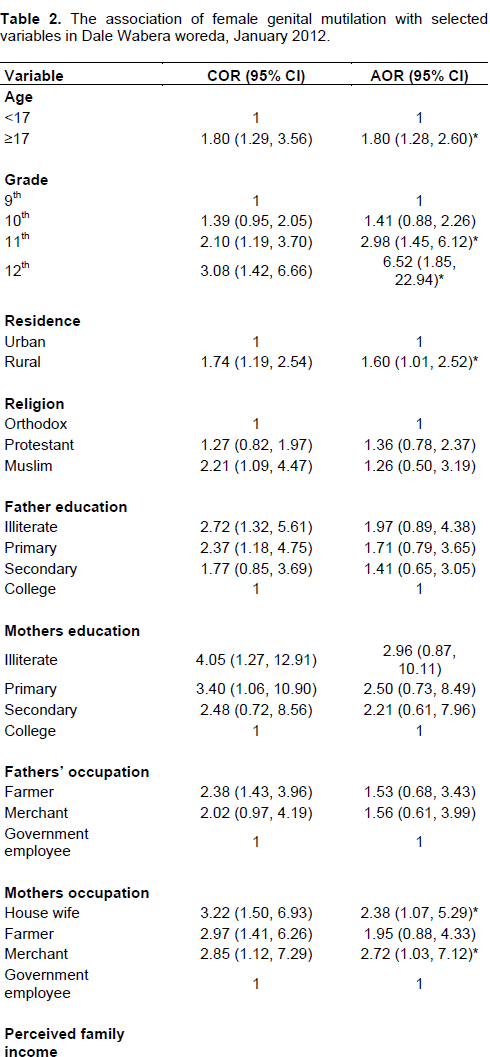
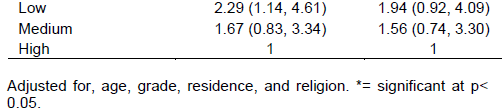
Associated factors of female genital mutilation
From those factors significantly associated with dependent variable (age, grade, residence, religion, father education, mother education, father occupation, mother occupation, and perceived monthly income) during crude analysis, four of them (age, grade, residence, and mother occupation) remained independently associated with the dependent variable on multivariate analysis.
Among the age groups, those ≥17 years were at higher odds of practicing FGM compared to the other age group [AOR 1.8; 95% CI (1.28, 2.6). The odds of FGM was higher in grades eleven and twelve students compared to grade nine [AOR=2.98, 95% CI (1.45, 6.12)] and [AOR=6.52, 95%CI (1.85, 22.94)], respectively.
Residence was one of the factors independently associated with magnitude of FGM given that the chance of being mutilated was higher in students from rural area compared to those urban residents [AOR=1.6, 95% CI (1.01, 2.52)].
The other factor independently associated with FGM was mother occupation. The odds of practicing FGM was higher among female students whose mothers were housewives and merchants compared to those with government employee mothers after adjusting for age, grade, and residence [AOR 2.38; 95% CI (1.07, 5.29)] and [AOR 2.72; 95% CI (1.04, 7.12)], respectively (Table 2).
DISCUSSION
As indicated in the study, based on data revealed from the field 77.8% (74.9%, 80.7%) of the students that underwent the procedure which is higher than the Demographic and Health Survey (DHS) (2005) country prevalence (74.3%) but lower than the Oromia regional prevalence (87.2%) (Central Statistical Agency, 2005), this lower prevalence in this study may be due to their age that in DHS those in age group of 15-49 were included and in this current study the maximum age was 23. The finding of this study is also lower than the finding of the base line survey which was 89.4% in Kelem Wollega zone, but higher than that of follow up survey which was 61.3% (EGLDAM, 2011) in the same zone. It is also lower than the finding of the study conducted in West Showa zone which was 96.4%, and the difference may be due to inclusion of higher age group (24-33) years in the former study (Oduro et al., 2006). So, if we would include higher age of the study participants the current prevalence might be higher. The prevalence is lower than the finding of the study conducted among high school female students in south Ethiopia which was 82.2% (Tamire and Molla, 2011) and the possible explanation is the difference in age at which FGM is performed. When we compare finding of our study with some other countries, the finding of this study is higher than the finding of the study conducted among high school students in Egypt which was 50.3%(17). It is also much higher than that of primary school girls in Addis Ababa which was 25.8% (Tamire and Molla, 2011; Zewde et al., 2009) and might be due to the difference in age of the study participants included and the other may be those of Addis Ababa with more educated parents and has higher access to information.
The age at which FGM is performed on girls varies between countries and even from area to area within the same country. In most countries it is practiced on girls between four and twelve years but it can be done as early as before one year of age and in some areas it can be delayed up to just before their marriage (Population Reference Bureau, 2010; Tag-Eldin et al., 2008; Kerubo, 2010; Olenja and Kamau, 2001; Boyden et al., 2011; Kaplan et al., 2011).
According to the research conducted in Egypt, the average age of mutilation was 10.1±2.3 years (Afifi and Bothmer, 2007), while the figure was 2.9±0.65 years from the study conducted in the primary school girls in Addis Ababa (Zewde et al., 2009). The finding of this study showed that the average age of FGM is 12.95±2.23 years which is much higher than that of the study conducted in Addis Ababa and also slightly higher than the value from the Egypt. As confirmed by different studies, this age varies based on the culture of the specific population (Kaplan et al., 2011).
More than 95% of the procedure was done by traditional practitioners and the rest was done by health professionals. This finding agrees with results of most studies that FGM is mostly done by traditional practitioners commonly known by the name of the village women (World Health Organization, 2008).
Educational level of the study participants were independently associated with the prevalence of FGM especially in those grades eleven and twelve students. The odds of the practice was about three times higher in grade eleven and about 6.5 times higher in grade twelve students when compared with grade nine female students. This finding should be cautiously interpreted because one could be confused with the idea of decreasing trend of FGM as a result of increased community awareness, but the reality may be those who did not undergo FGM this year are candidates for the coming year as the community is still highly in favour of its continuation. This finding is in line with that of study conducted in Egypt and south Ethiopia which showed increased magnitude of the practice along with their grades (Njue and Askew, 2004; Stewart et al., 2002; Tag-Eldin et al., 2008).
The age of the study participants was the other variable independently associated with FGM that those seventeen years and above were with a higher odds of the practice; however, like that of the grades of the study participants, the association with the age needs cautious interpretation. This also agrees with the findings of other studies that the prevalence of FGM increased with the age of the participants (Mitike and Deressa, 2009; Tamire and Molla, 2011).
Even though it is marginal, residence of the study participants was the other factor independently associated to the practice of FGM as those who were from rural areas were at higher odds of the practice and this may be due to the discrepancy in access to information about harmful effects of FGM. This finding agrees with that of high school based study in Egypt and EDHS (2005) findings in which the residence of students was independently associated with the prevalence of FGM (Central Statistical Agency, 2005; Tamire and Molla, 2011; Tag-Eldin et al., 2008).
Mothers’ occupation was the other factor significantly associated to FGM. Female students whose mothers were housewives and merchants were at higher odds of practicing FGM compared to those students whose mothers were government employees even though it had no significant association in previous researches with increased prevalence of FGM (Tamire and Molla, 2011). This may be because of those mothers who were government employees that have had better access to information about harmful effects of the practice when compared to housewives mothers who spent most of their time at home and merchants who are mostly busy with their work. Although this study showed no association between magnitude of FGM and education of the parents, other studies showed the presence of significant association with parental educational status (Central Statistical Agency, 2005; Tamire and Molla, 2011; Zewde et al., 2009; Tag-Eldin et al., 2008; UNICEF, 2005b). This may be due to fear of the challenges they would face from the community even if they have information about harmful consequences of FGM.
As a limitation, the research was conducted among high school students and is not community based and it may not reveal realistic and very precise image of the issue figure in the general community.
CONCLUSIONS
Currently most people assume that the prevalence of FGM is decreasing in most parts of the country, but this study showed that this figure is very high (77.8%) in the current study area.
Study participants with age ≥17, grades 11 and 12, residing in rural area, and having housewives and merchant mothers’ occupation were at higher odds of FGM. Female genital mutilation is one among traditional practices that is still ongoing across society either in severe or less form in both urban and rural areas. The practice is harmful and cause serious problem on the circumcised women and girls that may be categorized as both short term and long term pain. Community sensitization about the negative impacts of FGM should be designed through different mechanisms such as media, health personnel, community leader, religious leader, and seminar presentation, community education to increase awareness resulting in behavioral change over time. The governmental and nongovernmental organizations working towards building community or girls free from such harmful traditional practice especially in remote areas should rely on evidence based interventions. Women’s affairs bureaus and different gender based association should actively work starting from regional to international level collaboratively with both governments based and non – governmental organizations to curb the practice from the root. A community based study with stronger study design is also recommended.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Afifi M, Bothmer M (2007). Egyptian women's attitudes and beliefs about female genital cutting and its association with childhood maltreatment. Nurs. Health Sci. 9:270-276. |
|
|
Boyden J, Pankhurst A, Tafere Y (2011). Harmful Traditional Practices and Child Protection: Contested Understandings and Customs of Female Early Marriage and Genital Cutting in Ethiopia. Available at: |
|
|
Central Statistical Agency (2005). Ethiopian Demographic and Health survey. Available at: |
|
|
EGLDAM (2011). Survey on Harmful Traditional practices in Ethiopia, Oromiya Regional Report. Available at: |
|
|
Emam EA, EL-Maghawri AM, Labeeb SA (2011). Cultural Awareness about Female Genital Mutilation among Female Employees of Minia University. J. Am. Sci.7 (4):611-617. |
|
|
Kaplan A, Hechavarría S, Martín M, Bonhoure I (2011). Health consequences of female genital mutilation/cutting in the Gambia, evidence into action. BMC Reprod. Health 8(1):26. |
|
|
Kaplan MA, Torán MP, Moreno NJ, Fàbregas MJC, Mu-oz OL (2009). Perception of primary health professionals about Female Genital Mutilation: from healthcare to intercultural competence. BMC Health Serv. Res. 9:11. |
|
|
Kerubo KR (2010). Female Genital Mutilation -effects on women and young girls P 31. |
|
|
Konjit K (2002). Gender based violence-an impediment to sexual and reproductive health of women. Timar Bull. 3:14. |
|
|
Mitike G, Deressa W (2009). Prevalence and associated factors of female genital mutilation among Somali refugees in eastern Ethiopia: a cross-sectional study. BMC Public Health 9:264. |
|
|
Njue C, Askew I (2004). Medicalization of Female Genital Cutting among the Abagusi in Nyanza Province, Kenya. |
|
|
Oduro AR, Ansah P, Hodgson A, Afful TM, Baiden F, Adongo P, Koram KA (2006). Trends in the prevalence of female genital muti-lation and its effect on delivery outcomes in the kassena-nankana district of northern Ghana. Ghana Med. J. 40(3). |
|
|
Olenja J, Kamau J (2001). Olenja, J., & Kamau, J. (2001). Baseline Survey on Female Genital Mutilation Practices in Koibatek District, Rift Valley Province. Ministry of Health/GTZ FGM Project. |
|
|
Population Reference Burea (2010). Female Genital Mutilation/Cutting: Data and Trends. Available at: |
|
|
Stewart H, Morison L, White R (2002). Determinants Of Coital Frequency Among Married Women In Central African Republic: The Role Of Female Genital Cutting. J. Biosoc. Sci. 34:525-539. |
|
|
Tag-Eldin MA, Gadallah MA, Al-Tayeb MN, Abdel-Aty M, Mansour E, Sallem M (2008). Prevalence of female genital cutting among Egyptian girls. Bull. World Health Org. 86(4):269-274. |
|
|
Tamire M, Molla M (2011). Prevalence and believe in the continuation of Female Genital Cutting among high school girls in Hadiya zone Southern Ethioipia. BMC Public Health 13(1):1120. |
|
|
UNICEF (2005). Innocent Digest Web site. Changing a harmful social convention: Female genital mutilation/ cutting. Available at: |
|
|
UNICEF (2005b). Female Genital Mutilation/Cutting. P 40. |
|
|
USAID (2012). Gender Equality and Female Empowering Policy. P 7. |
|
|
Wagner N (2011). Violence against women: Female genital cutting a practice impossible to abandon.Available at: |
|
|
World Health Organization (WHO) (2006). Department of Gender and Women's Health, Female genital mutilation: Integrating the prevention and the management of the health complications into the curricula of nursing and midwifery. Tech. Rep.WHO/RHR/01.17.144. |
|
|
World Health Organization (WHO) (2008). Eliminating Female Genital Mutilation: an interagency statement UNAIDS, UNDP, UNECA, UNISCO, UNFPA, UNHCHR, UNICEF, UNIFEM, WHO. Geneva, Switzerland. Tech. Rep. 48. |
|
|
World health organization (WHO) (2011). An update on WHO's work on female genital mutilation (FGM). |
|
|
Zewde T, Haidar J, Kogi W (2009). Magnitude of and driving factors for female genital cutting in schoolgirls in Addis Ababa, Ethiopia: A cross sectional study. South Afr. J. Child Health 4(3):78-82. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


