Short Communication
ABSTRACT
In some studies in diabetic people, chromium picolinate supplementation has lowered readings for both plasma triglycerides and blood sugar. In the present study, relatively low dose supplementation (200 µg chromium) did not lower blood sugar readings, but did lower triglyceride values in people with the following characteristics: type 2 diabetes, moderately elevated blood sugar, and not using insulin therapy. These results support the supposition that chromium picolinate can affect triglyceride concentrations independently of effects on carbohydrate metabolism.
Key words: Chromium, diabetes, triglycerides.
INTRODUCTION
Chromium (Cr) is a trace element that can affect carbohydrate, lipid, and protein metabolism (Anderson, 1998a; Evans, 1989). Cr supplementation can affect blood glucose, total cholesterol, HDL and triglycerides in some circumstances (Abdollahi et al., 2013; Anderson et al., 1997; Cefalu and Hu, 2004; Heimbach and Anderson, 2005; Morris et al., 1999). This has led to classifying Cr as an essential nutrient (Anderson, 1998b), though others have suggested that Cr acts only as a drug in some unhealthy situations (Vincent, 2013). One argument against the essential nutrient role has been a lack of consistent positive effects of Cr supplementation in healthy people (Masharani et al., 2012). A counter argument states that Cr supplementation will not have such effects in all healthy people, but only in people with at least a moderate Cr deficiency. However, no accurate method for evaluating Cr status has been verified (DiSilvestro, 2005).
In people with diabetes, Cr supplementation has produced a decrease in fasting blood glucose values (Abdollahi et al., 2013; Bahijiri et al., 2000; Geohas et al., 2007; Pei et al., 2006; Rabinovitz et al., 2004). However, in other studies, Cr fails to affect blood glucose values (Abdollahi et al., 2013; Lee and Reasner, 1994; Preuss et al., 2000; Uusitupa et al., 1983). If Cr does indeed function as an essential nutrient, these variations could arise due to variations in the subjects’ Cr status. If Cr acts solely as a drug, then the variations would depend on other factors. There have also been studies examining the effect of Cr on triglyceride levels in humans. A number of studies show a decrease in triglyceride values while also showing improved glucose control (Bahijiri et al., 2000; Geohas et al., 2007; Rabinovitz et al., 2004). These results reinforce an earlier proposed concept that Cr effects on lipid metabolism are mediated by effects on carbohydrate metabolism (Mertz, 1993). In contrast to this concept, in one human study, blood glucose readings are unchanged, but triglyceride values decrease (Lee and Reasner, 1994). Such a result suggests that Cr could affect lipid metabolism through either drug or nutritional mechanisms that go beyond modulation of carbohydrate metabolism. In this study lowering triglyceride but not glucose values, the study subjects had the following characteristics:
a) Mainly a US Hispanic population,
b) Diabetic people with fairly high fasting glucose values,
c) People using insulin injections and/or oral glucose-lowering drugs.
It needs to be determined if in other types of subjects, Cr supplementation can lower triglyceride concentrations without lowering glucose levels. Moreover, such additional studies should modify one protocol detail of the previous study. That study only compared post supple-ment values to post placebo values. New studies should also look at changes pre-to post-treatment with Cr or placebo. The present study did this for type 2 diabetic subjects who had the following characteristics:
a) Live in the central Ohio area,
b) Have just moderately elevated glucose levels,
c) Do not take insulin injections.
This new study examined the same dose, intervention time, and Cr complex as the previous work where Cr affected readings for triglycerides, but not blood sugar (Lee and Reasner, 1994).
MATERIALS AND METHODS
Subjects
The protocol was approved by The Ohio State University Human Subjects Biomedical Institutional Review Board. All subjects signed an Institutional Review Board (IRB) approved consent form. Adult males and non pregnant females were recruited from in and around Columbus, Ohio and Wooster/Canton, Ohio. Subjects fit the following inclusion criteria:
1. Age 40-60 years old,
2. Physician confirmed type 2 diabetes.
3. Glycosylated hemoglobin (HbA1c) greater than 7.0%,
4. Fasting plasma glucose between 7.6 and 10 mmol/L,
5. No use of insulin,
6. Body mass index (BMI) between 25 and 35,
7. Non-smoking,
8. No intake history of Cr supplementation within the last 3 months,
9. No major health problems other than type 2 diabetes.
Conformance to these criteria was based on answers to an eligibility questionnaire.
Research design
Subjects were randomly assigned to one of two groups:
1. Placebo (starch capsules).
2. Cr picolinate (200 µg Cr/day/1 capsule) supplied by Kelatron Corporation of Ogden, UT, USA.
Neither the subjects nor the person giving the supplements knew the group assignment. Subjects were instructed to maintain their previous dietary and exercise practices during participation. Subjects consumed the assigned product for 8 weeks and had blood samples taken before and after the supplementation period. Each sampling followed an overnight fast.
Blood analysis
Blood was collected by venipuncture into heparinized tubes. The tubes were centrifuged for approximately 10 min at 3000 rpm. Plasma was removed and stored at -70°C. Plasma glucose and triglycerides was assessed using the Roche Cobas C111 Clinical Chemistry Analyzer (Indianapolis, Indiana, USA).
RESULTS
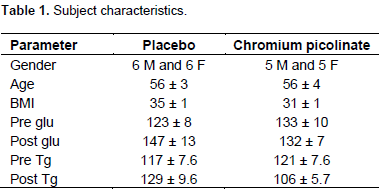
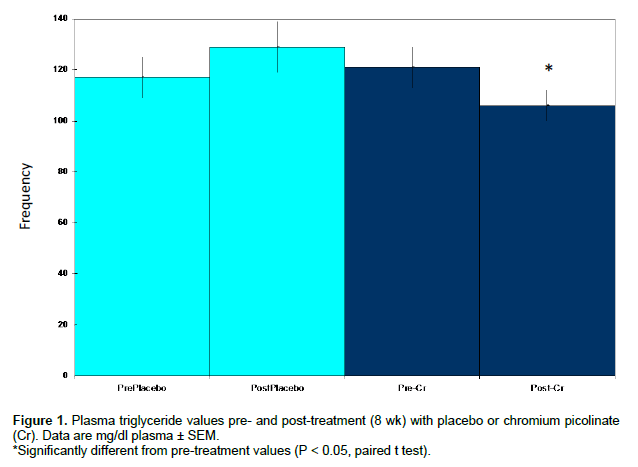
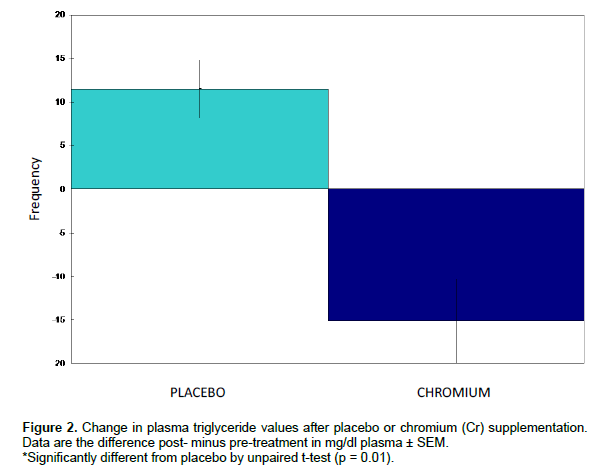
Subject characteristics are noted in Table 1. Neither Cr supplementation nor placebo affected plasma glucose readings (Table 1). Cr supplementation, but not placebo, lowered plasma triglyceride values (Figure 1). The mean change in triglyceride values for the Cr group was significantly different than the change in the placebo group (Figure 2). In fact, in the placebo group, the mean value increased. Power values for the Cr matched samples, as well as the change comparison between groups, were over 0.99 for p < 0.05, two sided test. Plasma cholesterol values [total, high density lipoprotein (HDL) and low density lipoprotein (LDL)] were unchanged by either placebo or Cr (data not shown).
DISCUSSION
A number of studies in diabetic subjects have reported that Cr supplementation improves glucose status and decreases plasma triglycerides (Bahijiri et al., 2000; Geohas et al., 2007; Rabinovitz et al., 2004). However, not all studies on Cr supplementation in diabetic subjects show an effect on glucose status. Most of these studies do not look at triglyceride readings. On the other hand, one study has shown a decrease in triglyceride values without a change in blood glucose values (Lee and Reasner, 1994). This study was done in a US Hispanic type 2 diabetic population with fairly high fasting glucose values. Some of the subjects in the study had enough problem with controlling blood sugar that they were using insulin injections to try to treat the problem. The present study demonstrated that in subjects with moderately elevated blood glucose, and who were not using insulin injections, Cr supplementation can lower triglyceride concentrations without lowering glucose levels. The subjects studied here were recruited from a typical USA mid-western diabetic population. Thus, the results of this study expand on the previous study. Taken together, the two studies indicate that Cr supplementation can impact lipid metabolism via mechanisms not directly related to carbohydrate metabolism.
Since plasma cholesterol concentrations were not changed by Cr, Cr would seem to affect this aspect of lipid metabolism via different mechanisms than the effects of triglyceride metabolism. Any Cr effects on cholesterol may be tied more directly to the effects on carbohydrate metabolism, which appeared to not occur in the present study. It is not yet certain why Cr supple-mentation impacts blood glucose related parameters in some studies but not others (DiSilvestro, 2005). Cr dose does not appear to be the only factor, though the dose used in the present study falls in the lower end of what has been used in diabetes studies (DiSilvestro, 2005). In the present study, the mean percent decrease in triglyceride values in the Cr picolinate group was not especially large (15%). However, in this study group, the mean initial triglyceride value was not extremely high. A larger decrease might occur when diabetics have a high starting blood triglyceride level. It is also possible that a higher Cr dose than used here might produce a bigger response.
It is not yet possible to determine whether the Cr dose used here worked by correcting some degree of deficiency or via a pharmacological effect. Unfortunately, a good means of assessing Cr status has not yet emerged (DiSilvestro, 2005). The present study’s dose, 200 µg/day, is the upper end of what was established in 1989 as the estimated safe and adequate daily dietary intake range for Cr (National Research Council, Food and Nutrition Board, 1989). On the other hand, as noted earlier, this dose falls at the lowest end of what typically has been employed in diabetes studies (Di Silvestro, 2005). It is difficult to relate the current study’s dose to a dietary Cr requirement for four reasons. One, no recommended dietary allowance has been established yet for healthy people (Institute of Medicine, Food and Nutrition Board, 2001). Two, the possibility that diabetes raises Cr needs has not been ruled in or out yet. Third, if some degree of Cr deficiency does commonly exist in people with type 2 diabetes, a corrective action may temporarily require giving a dose above the normal requirement. Four, Cr has been suggested to not even be an essential nutrient for humans (Vincent, 2013).
Lipidemia in diabetic populations presents a major risk for heart disease (Vijayaraghavan, 2010). Controlling triglyceride level with an inexpensive Cr supplement could decrease this risk. The current study showed that a Cr effect on triglycerides can occur without affecting blood glucose values, and without extreme conditions such as very high triglyceride readings or extremely poor glucose control.
ACKNOWLEDGEMENTS
The authors thank Karen Myers, RN, for logistical arrangements for the blood draws done in Wooster.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
|
Abdollahi M, Farshchi A, Nikfar S, Seyedifar M (2013). Effect of chromium on glucose and lipid profiles in patients with type 2 diabetes; a meta-analysis review of randomized trials. J. Pharm. Pharm. Sci. 16:99-114. Pubmed |
||||
|
Anderson RA (1998a). Chromium, glucose intolerance and diabetes. J. Am. Coll. Nutr. 17:548-555. Crossref |
||||
|
Anderson RA (1998b). Recent advances in the clinical and biochemical manifestation of chromium deficiency in human and animal nutrition. J. Trace Elem. Exp. Med. 11:241-50. Crossref |
||||
|
Anderson RA, Cheng N, Bryden NA, Polansky MM, Cheng N, Chi J, Feng J (1997). Elevated intakes of supplemental chromium improve glucose and insulin variables in individuals with type 2 diabetes. Diabetes 46:1786-1791. Crossref |
||||
|
Bahijiri SM, Mira SA, Mufti AM, Ajabnoor MA (2000). The effects of inorganic chromium and brewer's yeast supplementation on glucose tolerance, serum lipids and drug dosage in individuals with type 2 diabetes. Saudi Med. J. 21:831-837. Pubmed |
||||
|
Cefalu WT, Hu FB (2004). Role of chromium in human health and in diabetes. Diabetes Care 27:2741-2751. Crossref |
||||
| DiSilvestro RA (2005). Handbook of Minerals as Nutritional Supplements, CRC Press, Boca Raton. p. 272. | ||||
| Evans GW (1989). The effect of chromium picolinate on insulin controlled parameters in humans. Int. J. Biosci. Med. Res. 11:163-180. | ||||
|
Geohas J, Daly A, Juturu V, Finch M, Komorowski JR (2007). Chromium picolinate and biotin combination reduces atherogenic index of plasma in patients with type 2 diabetes mellitus: A placebo-controlled, double-blinded, randomized clinical trial. Am. J. Med. Sci. 333:145-53. Crossref |
||||
|
Heimbach JT, Anderson RA (2005). Chromium: Recent studies regarding nutritional roles and safety. Nutr. Today 40:2-8. Crossref |
||||
| Institute of Medicine, Food and Nutrition Board (2001). Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. National Academy Press, Washington, DC. p 773. | ||||
|
Lee NA, Reasner CA (1994). Beneficial effect of chromium supplementation on serum triglyceride levels in NIDDM. Diabetes Care 17:1449-1452. Crossref |
||||
|
Masharani U, Gjerde C, McCoy S, Maddux BA, Hessler D, Goldfine ID, Youngren J (2012). Chromium supplementation in non-obese non-diabetic subjects is associated with a decline in insulin sensitivity. BMC Endocr. Disord. 12:31. Crossref |
||||
|
Mertz W (1993). Chromium in human nutrition: A review. J. Nutr. 123:626-633. Pubmed |
||||
|
Morris BW, MacNeil S, Hardisty CA, Heller S, Burgin C, Gray TA (1999). Chromium homeostasis in patients with type II (NIDDM) diabetes. J. Trace Elem. Med. Biol. 13:57-61. Crossref |
||||
| National Research Council, Food and Nutrition Board (1989). Recommended Dietary Allowances, 10th Edition. National Academy Press, Washington. p. 285. | ||||
|
Pei D, Hsieh CH, Hung YJ, Li JC, Lee CH, Kuo SW (2006). The influence of chromium chloride-containing milk to glycemic control of patients with type 2 diabetes mellitus: a randomized, double-blind, placebo-controlled trial. Metabolism 55:923-927. Crossref |
||||
|
Preuss HG, Wallerstedt D, Talpur N, Tutuncuoglu SO, Echard B, Myers A, Bui M, Bagchi D (2000). Effects of niacin-bound chromium and grape seed proanthocyanidin extract on the lipid profile of hypercholesterolemic subjects: A pilot study. J. Med. 31:227-246. Pubmed |
||||
|
Rabinovitz H, Friedensohn A, Leibovitz A, Gabay G, Rocas C, Habot B (2004). Effect of chromium supplementation on blood glucose and lipid levels in type 2 diabetes mellitus elderly patients. Int. J. Vitam. Nutr. Res. 74:178-82. Crossref |
||||
|
Uusitupa MI, Kumpulainen JT, Voutilainen E, Hersio K, Sarlund H, Pyörälä KP, Koivistoinen PE, LehtoEvans JT (1983). Effect of inorganic chromium supplementation on glucose tolerance, insulin response, and serum lipids in noninsulin-dependent diabetics. Am. J. Clin. Nutr. 38:404-410. Pubmed |
||||
|
Vijayaraghavan K (2010). Treatment of dyslipidemia in patients with type 2 diabetes. Lipids Health Dis. 9:144. Crossref |
||||
|
Vincent JB (2013). Chromium: Is it essential, pharmacologically relevant, or toxic? Met. Ions Life Sci. 13:171-198. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


